

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension is one of the major chronic diseases, and the number of patients with hypertension was nearly 1.1 billion in 2015 globally. In Korea, the number of patients diagnosed with hypertension has shown steadily increasing trends, from 3 million in 2002 to nearly 9 million in 2016.1
Hypertension is associated with various complications; in particular, it may seriously affect the cardiovascular system. Excessive pressure hardens the arteries, reducing the flow of blood and oxygen to the heart. This high pressure and reduced blood flow block the blood supply, and a lack of oxygen in myocardial cells may cause heart problems such as angina and heart failure (HF). Additionally, HF may occur due to insufficient blood and oxygen, and an irregular pulse may be related to sudden death. In addition to the cardiovascular system, hypertension may also lead to stroke by blocking or rupturing arteries that supply blood and oxygen to the brain and renal failure by causing renal injury.23 Thus, hypertension is the most important modifiable risk factor for cardiovascular and cerebrovascular diseases.4
Continuous management of hypertension may lower the risk of complications and mortality. Continuous management may be achieved by the concept of continuity of care (COC). COC refers to continually visiting the same medical institution, forming a close relationship with physicians or treatment teams, and working together toward the goal of improving disease.5 In terms of physicians’ aspect, high COC is related to a better understanding of patients’ blood pressure, dietary behaviors, and physical activity patterns.6 In terms of patients’ aspect, a close rapport with physicians may be related to improving lifestyle patterns and medical adherence.7
Unlike other countries, such as the United States, which operates management care systems such as Accountable Care Organizations and Health Maintenance Organizations, or England, which operates the National Health Service system and conducts patient-centered care, Korea is devoid of a high demand for improving COC because of the Fee for Service payment. Thus, a supplementary policy for improving COC is needed. In April 2012, a chronic disease management program for hypertension and diabetes was launched in Korea, which is only applied in primary care clinics.8 This program reduces the out-of-pocket expenses of patients from 30% to 20% of the consultation fee when patients enroll in this program by agreeing to visit the same clinic for the treatment of hypertension or diabetes. Thus, enhanced COC is expected by prompting patients to use the same medical institute. In addition, reestablishment of a healthcare delivery program is expected by encouraging patients with non-severe chronic disease to use clinics for treating those diseases instead of hospitals or tertiary hospitals.
After implementing a chronic disease management program, few studies have studied the association between chronic disease management programs and continuity of care. However, they could not investigate the program and the onset of complications because long-term data have not been accumulated. Thus, the aim of this study was to investigate the association between participating in a chronic disease management program and the onset of complications among patients with hypertension using whole-nation claims data. Additionally, we conducted sensitivity analysis by limiting the study population with health examination data or those with local clinic visits comprising at least 70% of all medical institution visits for treating hypertension.
METHODS
Data source and study population
For this study, we used National Health Insurance Service (NHIS) data (2011–2018). The data provided by the NHIS included medical history details, information on health insurance qualifications and medical institutions, health checkup results, and birth and death information of all Korean National Health Insurance and medical aid beneficiaries from 2002 to 2018, which comprises more than 95% of the entire nation. The subjects’ data were anonymized and collected.9
In this study, using data from the NHIS, patients with newly detected hypertension from 2012 to 2014 were selected and followed up until December 2018. Patients with newly developed hypertension were defined as those who were prescribed hypertension drugs for a new diagnosis of hypertension (I10) after 2012, without a history of being prescribed a hypertension drug for a diagnosis of hypertension before 2012.
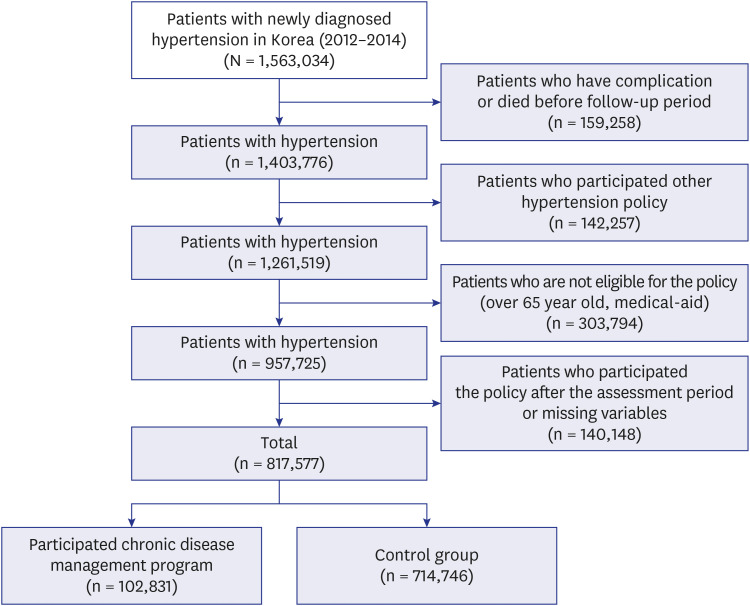
For exclusion criteria, patients with hypertension complications such as acute myocardial infarction (MI), stroke, chronic kidney disease (CKD), and heart failure (HF) before the enrollment period (2012–2014) were excluded. Those who died during the measurement period for participation in the chronic disease management program (1 year from the onset of hypertension) were also excluded from this study. In order to determine the effects of the chronic disease management program, subjects who participated in policies related to chronic diseases other than the chronic disease management program were excluded from the study. Subjects older than 65 years of age or receiving medical aid who gained limited benefits from the chronic disease management program were excluded from the study. Lastly, subjects who participated in the chronic disease management program after the measurement period were excluded. After excluding patients with missing data, the final subjects included 817,577 patients, among which 102,831(12.6%) subjects participated in the chronic disease management (Fig. 1).
Independent variable
The independent variable was participation in the chronic disease management program. It reduces the out-of-pocket expenses of consultation fee from 30% to 20% when patients enroll in this program by agreeing to visit the same clinic for the treatment of hypertension or diabetes. The subjects were divided into two groups, depending on whether they participated in the chronic disease management program within one year of the onset of hypertension. Subsequently, hypertension complications were investigated until the end of 2018.
Dependent variable
As the dependent variable, acute MI, stroke, CKD, and HF were selected as hypertension complications. Acute MI, stroke, and HF were defined as hospitalizations due to the International Classification of Diseases (ICD)-10 codes corresponding to each disease (acute MI, I21-24; stroke, I60-67; HF, I50), and CKD was defined as hospitalization and outpatient status due to an ICD-10 code of N18.10111213
Two sensitivity analyses were conducted to examine the effects of the chronic disease management program in various aspects. First, since the chronic disease management program was only implemented at the clinic level, the analysis was only conducted for patients who visited primary medical institutions for more than 70% of the hypertension treatment for one year after the onset of hypertension in order to match the severity and tendency of the patients. Second, in order to adjust for blood pressure control and lifestyle habits of the study subjects, the analysis was conducted for subjects who had a medical examination record within one year after the onset of hypertension, and we adjusted for blood pressure control, fasting blood sugar levels, exercise habits, and smoking status. Also, we tried to prevent overcorrection and report the sequential results according to the covariates by additionally analyzing the unadjusted model and the model adjusted for sex and age (Supplementary Tables 1, 2, 3, 4).
Covariates
The covariates included in the analysis were age (younger than 40, 40–44, 45–49, 50–54, 55–59, and 60–64 years), gender (male, female), income (quartile for employee National Health Insurance, quartile for local subscribers), underlying disease (Charlson Comorbidity Index; CCI), diabetes (with or without), residential area (13 cities and provinces), and the year of hypertension onset. In addition, we adjusted the health examination results in the sensitivity analysis for subjects who underwent a health checkup within a year of hypertension onset for the following factors: diabetes (non-fasting blood sugar disorders, diabetes), blood pressure (greater than 140/90, 140/90 to 120/80, normal), total cholesterol levels, triglyceride levels, low-density lipoprotein levels, high-density lipoprotein levels, body mass index (low, normal, pre-obesity stage, obesity stage 1, obesity stage 2), smoking status (smoking, past smoking, non-smoking), and exercise habits (low, moderate, and high activity).
Statistical analysis
For statistical analysis, the χ2 test, t-test, and analysis of variance were used to determine the differences in basic characteristics depending on participation in the chronic disease management program. Additionally, the Cox proportional hazards model was used to determine the risk of complications according to participation in the chronic disease management program. Results of the cox proportional hazards model were expressed as hazard ratio (HR) and their 95% confidence interval (CI). All covariates were adjusted and calculated and calculated P values were two sided, and assumed significant at P < 0.05. All results were analyzed using SAS 9 (SAS Institute, Cary, NC, USA).
RESULTS
Table 1 shows the general characteristic and distribution of the study population by hypertension complication. Of 817,577 patients with hypertension, 12.6% (n = 102,831) participated in the management program. Among the study population, 0.6% (n = 4,672), 2.4% (n = 19,974), 1.3% (n = 10,668), and 1.0% (n = 8,468) had MI, stroke, CKD, and HF, respectively. Regarding complications, 0.5%, 2.1%, 1.3%, and 0.7% of the program’s participants and 0.6%, 2.5%, 1.3%, and 1.1% of non-participants had MI, stroke, CKD, and HF, respectively.
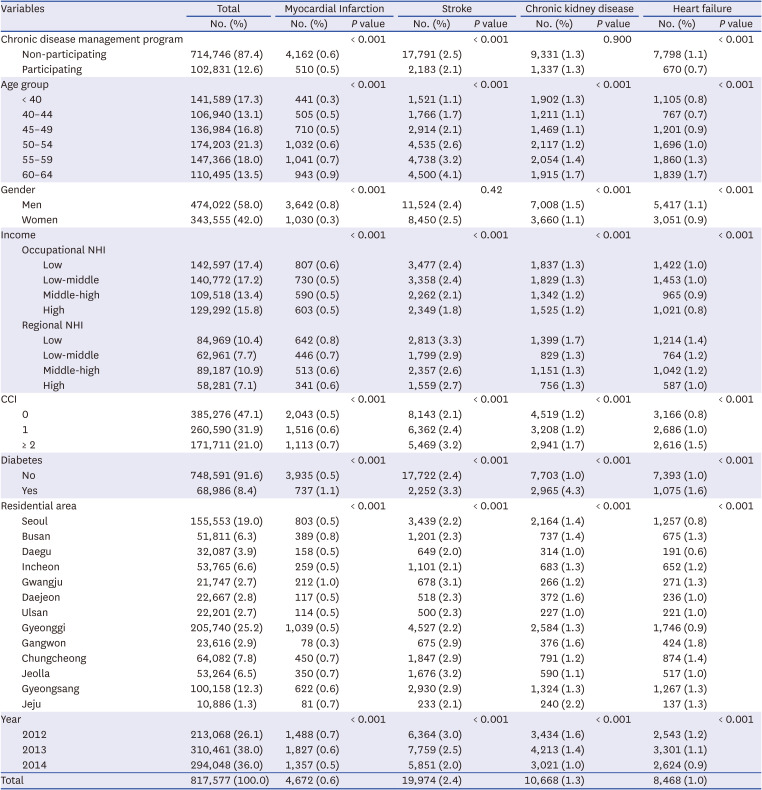
Table 1
Frequency of hypertension complications
![]()
Table 2 shows the results of survival analysis related to participation in the chronic disease management program and the onset of complications. Participants of the chronic disease management program were more likely to show lower HRs than those of non-participants in terms of all complications (MI: HR, 0.75; 95% CI, 0.68–0.82; stroke: HR, 0.75; 95% CI, 0.72–0.78; CKD: HR, 0.90; 95% CI, 0.85–0.96; HF: HR, 0.56; 95% CI, 0.52–0.61).
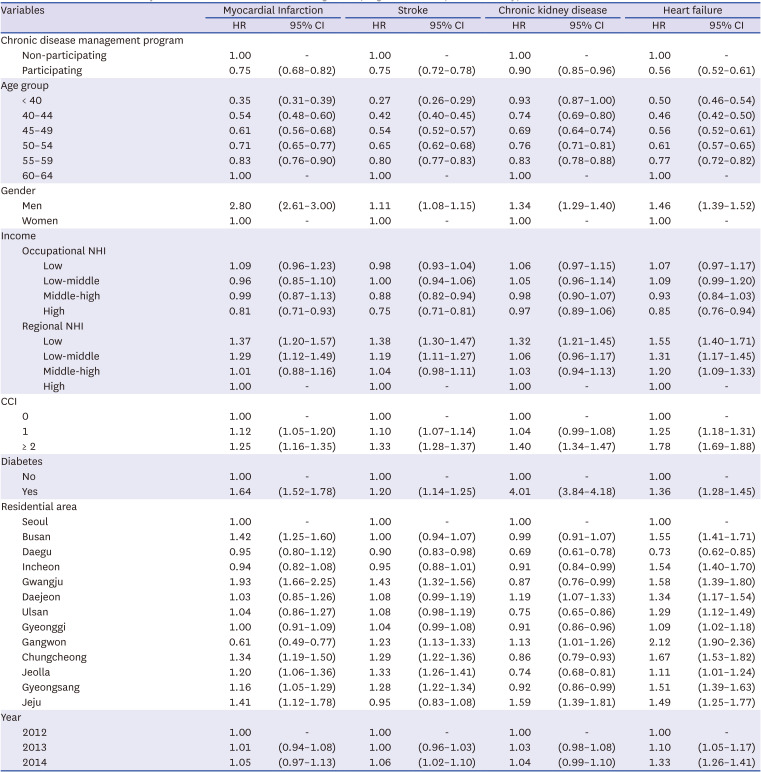
Table 2
Results of survival analysis related to chronic disease management program and complications of hypertension
HR = hazard ratio, CI = confidence interval, NHI = National Health Insurance, CCI = Charlson Comorbidity Index.
![]()
Table 3 shows the sensitivity analysis of different study populations. Despite the different study populations, basic trends were sustained, except for those associated with CKD. In model 1, which restricted the study population with health examination records, the HRs for complications were lower when participating in the program, but only stroke and HF showed statistically significant results (MI: HR, 0.85; 95% CI, 0.71–1.01; stroke: HR, 0.74; 95% CI, 0.68–0.80; CKD: HR, 0.97; 95% CI, 0.87–1.09; HF: HR, 0.61; 95% CI, 0.52–0.71). In model 2, which restricted the study population to those with local clinic visits comprising at least 70% of all medical institution visits for hypertension treatment, patients who participated in the program showed lower HRs for MI (HR, 0.84; 95% CI, 0.76–0.93), stroke (HR, 0.85; 95% CI, 0.81–0.89), and HF (HR, 0.80; 95% CI, 0.74–0.88) compared to those in non-participants. In the case of CKD, participants showed higher HRs for CKD compared to those of non-participants (HR, 1.15; 95% CI, 1.07–1.22).
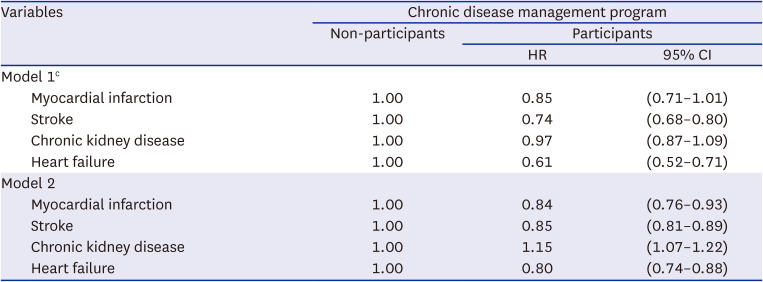
Table 3
Results of sensitivity analysis with different study populationsa,b
aStudy population for each model; Model 1: Hypertension patients who conducted health examination; Model 2: Hypertension patients who used local clinic for hypertension treatment at least 70%.
bAge group, sex, income, Charlson Comorbidity Index, diabetes, residential area, and hypertension onset year were adjusted in each model.
cBlood pressure, total cholesterol, triglycerides, low-density lipoprotein, high-density lipoprotein, body mass index, smoking, physical activity were additionally adjusted in model 1.
![]()
DISCUSSION
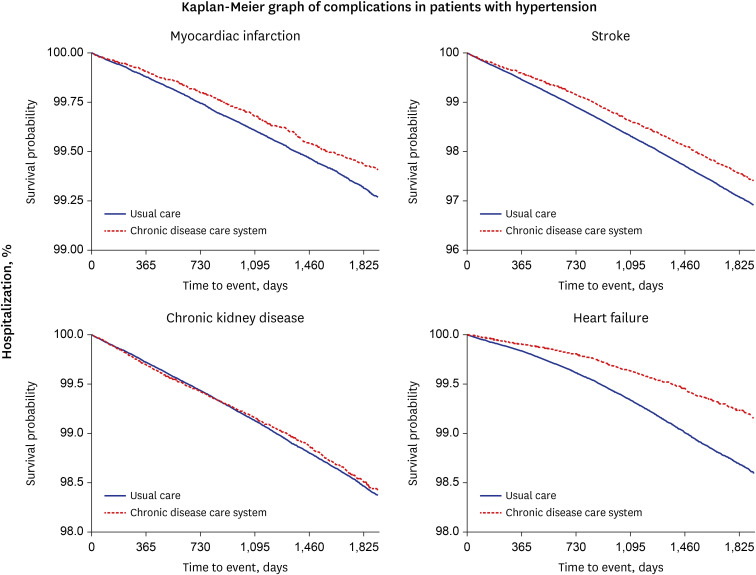
The results of this study showed that participants of the chronic disease management program were less likely to have hypertension complications (MI, stroke, CKD, and HF) compared to non-participants (Table 3, Fig. 2). Analysis of patients who primarily visited primary care clinics for the treatment of hypertension or had medical examination records also revealed that the participants had low risks of all complications except CKD.
Previous studies have demonstrated that patients enrolled in chronic disease management programs show higher COC compared to that in non-participants.1415 COC is one of the important concepts for treating chronic diseases because these diseases cannot be perfectly cured, and patients must be continuously monitored and taught how to perform self-management.16 To control blood pressure and prevent the onset of complications in patients with hypertension, lifestyle modifications such as sodium intake restriction, smoking cessation, moderation of body weight and alcohol consumption, and increase in dietary potassium intake and physical activity must be implemented.17 To enhance these activities, physicians’ continuous directions according to patients’ condition and adherence to those directions are needed. High COC is associated with better communication between physicians and patients with chronic disease, improving adherence to follow-up schedules or medications.18 In addition, improving the quality of care provided has also been reported by accumulating rapport between physicians and patients and knowledge of patients’ underlying diseases.619 Thus, better quality of care due to COC seems to be associated with a lower risk of complication onset.
Aside from the chronic disease management program, men were more likely to have all types of complications, and regional National Health Insurance beneficiaries with low income were more likely to have all types of complications compared to that in beneficiaries with high income. In addition, patients with hypertension and diabetes showed higher HRs for complications compared to those in patients without diabetes, and the HR for CKD was the highest among the HRs for all complications.
Regarding the sensitivity analyses, the HRs for complication onset decreased but the trends were maintained except in that for CKD. It seems that restricting the study population to those who mainly visited clinics for hypertension treatment may have attributed to these results by approximating the severity of hypertension among participants and non-participants. The study population with health examination records was also separately analyzed including adjustments for lifestyle patterns between participants and non-participants, showing similar results to those of the main analysis. However, CKD onset was higher in participants compared to that in non-participants in sensitivity analysis model 2. The chronic disease management program targeted two diseases: hypertension and diabetes. Therefore, there was a higher proportion of patients who had both hypertension and diabetes among program participants than that among non-participants, and we assume this is the magnitude of the effect on CKD. Based on the results in Tables, patients with hypertension and diabetes were more likely to participate in the program and have CKD (Table 2, Supplementary Table 1). Thus, the risk of CKD onset, which is directly affected by diabetes, seems to be higher.
The chronic disease management program was launched as a part of reorganizing medical institution function.20 The healthcare delivery system in Korea has become merely nominal, and the concentration of patients in large hospitals or distortion of functional differentiation among healthcare providers has worsened.21 Thus, the purpose of this program is to reorganize the healthcare delivery system by urging patients with non-severe chronic disease to visit primary care clinics instead of hospitals or tertiary hospitals. In addition, because the primary care system in Korea generally does not promote continuity or coordination, enhanced COC has also been expected in accordance with the objective of this program, which encourages patients use the same primary clinic for chronic disease treatment.22
However, the participation rate of this program was only 12.6% among patients with hypertension. The absence of direct incentives for clinics to participate in this program leads to the lack of clinics’ motives to encourage their patients to participate in this program. In addition, the lack of promotion of the program may be a reason for the low participation rate. Despite this low participation rate, previous studies have indicated high COC and low medical expenditures in participants,1415 which was the main purpose of this program, and the results of this study imply that participation in the program may be related to better outcomes among patients with hypertension.
The program only promotes patients to use the same primary care clinic for chronic disease treatment but does not change the current healthcare delivery system on a large scale and does not incur high expenses. Considering this efficiency, enhancing the participation rate may be related to better patient outcomes and a reduction in medical expenses. Thus, it is possible to think of ways to increase the participation rate by promoting the program and providing direct incentives to medical institutions per participant to urge patients to participate in the program. Also, chronic disease management program is only limited to hypertension and diabetes. Regarding the effect of the program, gradually expanding the target diseases is also needed.
This study has some limitations. First, the characteristics of participants and non-participants differed. Participating in the program was not mandatory; thus, participants may have been those who were easier to approach in terms of health policy or were more interested in health. To alleviate this limitation, we utilized health examination data for controlling smoking status, physical activity levels, blood pressure control, or fasting blood sugar levels, but it may have been insufficient to control these factors perfectly using claims data. Second, disease severity between participants and non-participants may have been different. The chronic disease management program only applied to clinics; thus, participants might have had a less severe status than that in non-participants. To overcome this, we first restricted the index case to patients with hypertension. We then adjusted for underlying diseases using the CCI. We conducted sensitivity analysis by restricting the study population to those who mainly visited local clinics for treating hypertension (at least 70% of all medical institution visits for hypertension treatment). Even though supplementing the limitation perfectly was difficult because of the characteristics of the claims data, our results revealed a positive effect in participants. In addition, our study has strength in terms of using whole-nation data. Considering that there are few studies in which chronic disease management programs and outcomes have been studied, our study may provide evidence for the positive effects of chronic disease management programs.
In conclusion, the results of this study revealed that participants of the chronic management program are less likely to have hypertension complications, including MI, stroke, CKD, and HF, and these results may offer evidence on the effect of the program. The results of this study imply that implementing policies aiming to improve care continuity can enhance outcomes in patients with hypertension.
 XML Download
XML Download