

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Demand for healthcare is characterized by the number of people seeking healthcare services, and awareness of healthcare services increases the probability that people in need will seek such services.123 People with disabilities (PWD) who have difficulty accessing health services might have a worse perception of service availability, compared to PWD who do not have disabilities.4567 The World Health Organization has summarized several broad categories of barriers to healthcare access: attitude factors (e.g., lack of prejudice and sensitivity to disability), physical factors (e.g., lack of access to medical institutions and the use of inappropriate medical devices), communication factors (e.g., lack of appropriate accommodations, including sign language interpretation or Braille), and economic factors (e.g., high medical cost burden). Primary care, which has a coordinating role in community healthcare services, is essential for improving healthcare access among PWD.8 Because of the current tendency towards deinstitutionalization, the residential base for PWD is shifting from healthcare facilities to the community; thus, there is an increasing need for a community-based primary care system.910
The primary healthcare (PHC) system in some developed countries, including the United Kingdom, Netherlands, the United States, and Japan, provides specific healthcare programs for vulnerable individuals, such as older people and people with severe chronic diseases (e.g., PWD).11 South Korea lacks institutionalized national primary care services; thus, it is difficult to prevent secondary conditions by implementing a holistic approach towards coordinated care services for PWD, and patient satisfaction with such healthcare services is inevitably low. PHC models for PWD incentivize healthcare providers to focus on patient-centered care and coordination; thus, they attempt to unify a fragmented system. Since enactment of the Right to Health and Access to Medical Services for Persons with Disabilities Act (Right to Health Act), the Korean government launched a PHC pilot project for PWD in 2018. This project involves team-based healthcare (including health education) and home visits by physicians or nurses for people who have a registered severe disability.12 The cost is fee-for-services based; PWD who use the service pay 10% of the cost (0% co-payment for some services, such as health assessments), while the government pays the remaining 90% of the cost. A recent study showed that low service costs hinder supply incentives and service quality; such costs also restrict beneficiaries (e.g., by limiting covered types of disabilities). These factors hinder demand incentives and have impacted completion of the PHC pilot project for PWD.11 Accordingly, the government has attempted to improve this PHC initiative for PWD since its launch. The third PHC initiative for PWD (1st project, May 2018–May 2020; 2nd project, June 2020–September 29, 2021) implements two improvements; it includes a comprehensive health assessment and care planning (compulsory), mid-term management (optional), education/consultation (optional), patient monitoring (optional), doctor or nurse visits (optional), and a voucher for a health check-up (optional). PWD who participate in the pilot project can receive the above benefits from participating PHC clinicians; they can also receive treatment, tests, and drug prescriptions from other PHC clinicians. This project has provided valuable insights into the importance of developing an institutionalized national PHC system in Korea.
The pilot project has developed into a core intervention that aims to improve healthcare access for PWD; however, its implementation has been limited among healthcare providers and consumers over the past three years. As of December 2021, only 521 PHC physicians (physicians in clinics or hospitals) nationwide participated in the project; only 127 of those physicians have experience providing care to PWD.13 The low participation rate among PHC physicians and the implementation difficulty encountered during this project are most likely related to poor demand incentives and supply structure. According to the National Health Insurance service, as of December 2020, 863 PWD had participated in the pilot project and received PHC; this number constituted only 0.09% of the 984,965 people with registered severe disabilities.13 Thus, there is a need to explore the reasons that underlie low participation, specifically from the perspective of PWD. Input from PWD is essential with respect to patient-centered care; such input can aid in the development and implementation of new healthcare policies. While the PHC project does not seek to provide a one-size-fits-all option for all PWD, demand and awareness for the project from the perspective of PWD should be explored. Efforts to track patient demand and awareness across care settings can improve healthcare delivery and reduce the likelihood of unmet healthcare service needs. Prior studies on the topic of the PHC pilot project for PWD, explored the experience and perception of disabled people or effectiveness of the pilot using the data only from who participated in the pilot project.12141516 However, there is no study identified the demand for or awareness of the pilot project among the PWD living in the community.
This study aimed to describe the demand for and awareness of a PHC pilot project for PWD among a population-based large sample of PWD; it also sought to identify relevant determinants for demand and awareness using Andersen’s behavioral model of health service use. This model is designed to analyze factors related to health service use,17 considering both individual factors and environmental factors (e.g., social status and cultural background). Therefore, it is widely used to analyze factors that affect unmet healthcare needs, service demand, and service awareness.18192021222324252627 This study provides fundamental evidence to support future PHC-focused healthcare policy measures for PWD.
METHODS
Study design and Data
This study is a secondary analysis of data from the population-based survey conducted in Gyeonggi Regional Health & Medical Center for People with Disabilities (RHMCPWD) funded by Gyeonggi-do and the Ministry of Health & Welfare, Republic of Korea. The data was designed with quota random sampling based on the population with disabilities in each district (city [si] and county [gun]) across the Gyeonggi province (do) to evaluate the health and healthcare accessibility of the disabled people living in the Gyeonggi province. The data was collected through the mobile-based survey of 1,140 PWD living in Gyeonggi-do between March 2021 and June 2021 (during the coronavirus disease 2019 pandemic period). This survey was conducted in cooperation with the government-affiliated community service center that serves the 31 involved administrative districts. Geographically, Gyeonggi-do has the largest number of administrative districts in Korea; There is significant variation in regional characteristics, such as the distribution of living infrastructure and resources for healthcare. In addition, this region includes the largest number of PWD in Korea (> 20% of the country’s total population with disabilities). The distribution of the disabled population that resides across the Gyeonggi administrative districts is diverse (Supplementary Fig. 1). Therefore, this study recruited a sample of 1,140 people by stratification in proportion to the number of populations with disabilities in the 31 administrative districts.
The data comprises five components: health status & social participation, healthcare accessibility, healthcare service utilization & satisfaction, PHC pilot project for PWD & Gyeonggi RHMCPWD, women with disabilities. The questionnaire of all components is built based on the validated national survey, the Korean national survey on persons with disabilities. In addition, this data was constructed by conducting a preliminary survey with some disabled people and experts to secure the validity of the questionnaire conducted in the mobile method. Through the preliminary survey, it was reviewed whether the order of the questions was appropriate and whether the expression of the questionnaire was appropriate.
Measurement and variables
Demand for and awareness of the PHC pilot project for PWD was investigated based on Andersen’s behavioral model of health service use. Environmental factors have a strong impact on healthcare service utilization; however, because this study focused on demand for and awareness of the pilot project, predisposing characteristics (e.g., age) and enabling factors (e.g., resource availability) and need-based factors (e.g., severity of disability) were the main attributes analyzed (Table 1).
Table 1
Frame of “Demand,” “Awareness,” and “Demand but poor awareness” about the primary healthcare pilot project for people with disabilities (using the Andersen’s model of healthcare utilization)
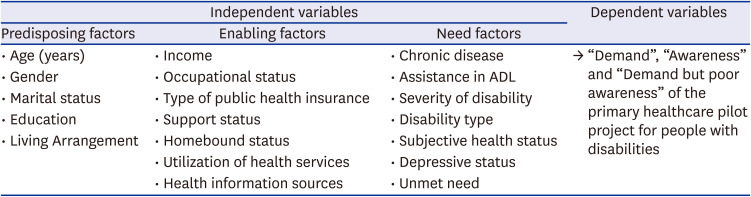
Dependent outcome measures included demand for the project, awareness of the project, and demand with poor awareness of the project. If respondents were unaware of the project, they were provided a brief description prior to completing the survey, which ensured that they could accurately convey their demand for the project. Respondents were asked “Do you think the PHC pilot project for PWD is necessary?”; a “yes” response was regarded as a demand for the project. Similarly, awareness of the project was regarded as a “yes” response to the question “Do you know about the PHC pilot project for PWD?” Demand for the service with poor awareness was defined as a “no” response to the question concerning awareness and a “yes” response to the question concerning demand. Independent variables were categorized into predisposing factors, enabling factors, and need-based factors based on Andersen’s behavioral model of health service use. Though we selected most of the independent variables according to the Andersen’s model,17192122232425 some variables added to the model through the review of the prior studies about the health service demand or awareness or unmet need for healthcare.12262829303132 For example, predisposing factors included socioeconomic characteristics such as age (< 20 years, 20–64 years, and ≥ 65 years), gender, marital status, education level, and living arrangement (e.g., living alone). Enabling factors included income level, occupational status, type of public health insurance, presence of caregivers (including informal caregivers such as family members and formal caregivers such as activity assistants), and homebound status (going out less than once per week and needing help from others for most activities of daily living [ADL]). Among the many tools for assessing homebound, we mixed the idea from the two prior studies for the conciseness and validity; one question used; “how many days they left their home during the previous week?”33 and the other question used; “In the past 30 days, how much difficulty did you have in leaving home?”34. The use of any health services (in-home health services from public health centers, community-based rehabilitation services from public health centers, assistive technology services, health education, or a health promotion program), and use of health information sources were confirmed. Lastly, need-based factors included chronic disease, the degree of need for assistance with ADL (defined as “no need for help” only if the PWD could do everything by his- or herself), severity of disability, type of disability (i.e., external physical, mental and developmental, or internal organ), subjective health status, depression, and an unmet need for medical care (Supplementary Table 1).
Statistical analysis
All analyses were performed using the STATA statistical package. To describe demand, awareness, and demand but poor awareness, we conducted a descriptive analysis that considered the respondents’ predisposing factors, enabling factors, and need-based factors. The χ2 test was used to compare demand, awareness, and demand but poor awareness according to the respondents’ characteristics. Second, multivariate analysis using a logistic regression model was performed to identify factors that affected demand, awareness, and demand but poor awareness.
RESULTS
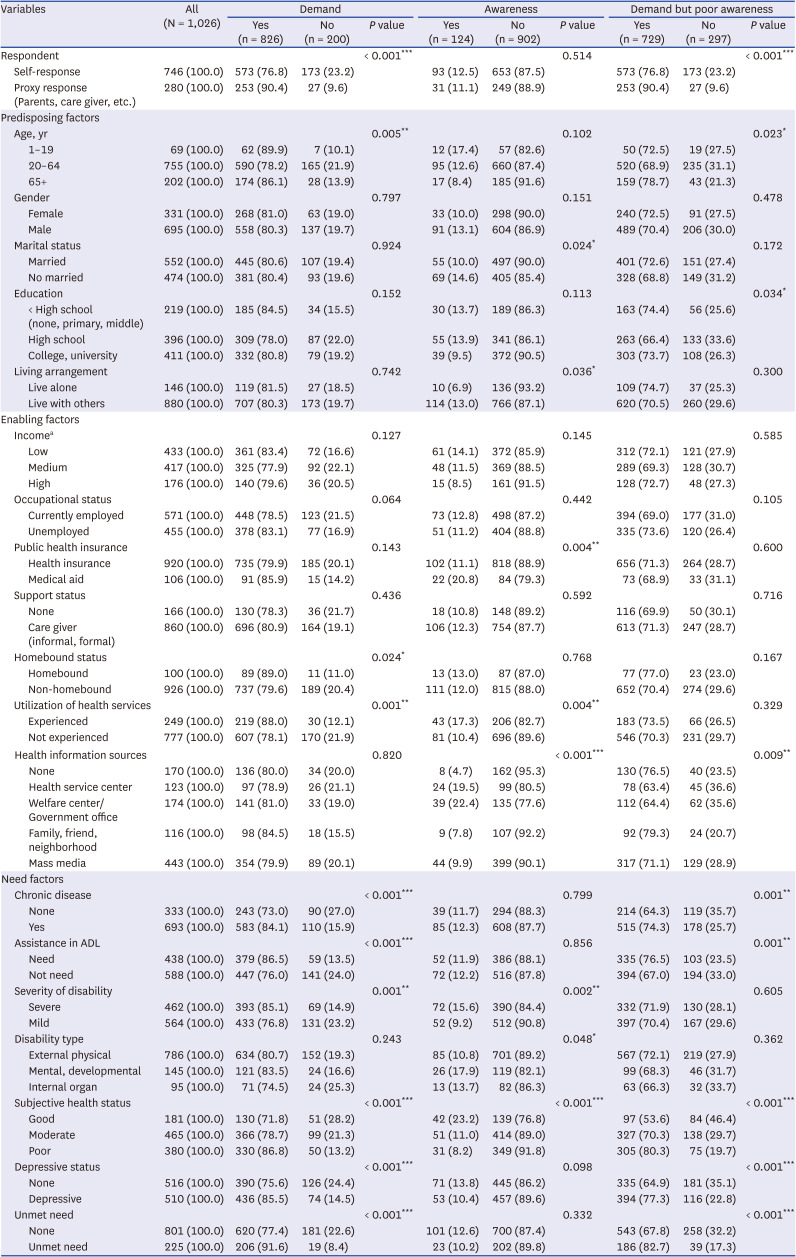
Among the 1,140 respondents, 1,026 responses were analyzed; we excluded respondents who did not provide responses to some variables (e.g., education and income level). In addition, if the respondent was unable to respond because of age or severe disability, a caregiver (e.g., a parent or neighbor) provided a proxy response for analysis. Table 2 presents the characteristics of the respondents who had a demand, who were aware of, and who had a demand but poor awareness of the PHC pilot project for PWD. Overall, 80.5% (n = 826) of the respondents expressed a need for the project, but only 12.1% (n = 124) were aware of it, indicating the existence of a large gap between demand and awareness.
Table 2
Demographic and health related variables according to “Demand,” “Awareness,” and “Demand but poor awareness” about the primary healthcare pilot project for people with disabilities
Demand, awareness, and combination
Demand
There was a significant difference in service demand according to age group. Of the respondents aged 20–64 years, 78% expressed a need for the project, while more than 85% of the respondents aged < 20 years or ≥ 65 years expressed such a need (χ2 = 10.607; P = 0.005). Among the enabling factors, a larger number of PWD who had difficulty going out wanted to receive the service (89.0%), compared to PWD who did not have such difficulty (79.6%) (χ2 = 5.093; P = 0.024). A greater proportion (88.0%) of respondents who had previously utilized health services from a community healthcare center responded that they needed the project, compared to respondents who had not utilized such services (78.1%) (χ2 = 11.613; P = 0.001). Among the need-based factors, more respondents with chronic diseases (84.1%) reported a need for the project, compared to respondents without such diseases (73.0%) (χ2 = 17.831; P < 0.001). There was also a significant difference in demand depending on whether the respondents needed assistance with ADL; respondents who needed assistance expressed a higher demand for the project (86.5%) than did respondents who did lacked such a need (76.0%) (χ2 = 17.666; P < 0.001). In addition, more people with severe disabilities (85.1%) needed the project, compared to people with less severe disabilities (76.8%) (χ2 = 11.127; P = 0.001). A greater proportion of PWD with poor subjective health (86.8%) reported that they wanted to participate in the project, compared to PWD in good health (71.8%) (χ2 = 19.372; P < 0.001). More than 90% of PWD who had an unmet need for medical care said they needed the project; this proportion was greater than the proportion of PWD who lacked an unmet need (77.4%) (χ2 = 22.419; P < 0.001).
Awareness
Among the predisposing factors, fewer married PWD (10%) were aware of the project, compared to unmarried PWD (14.6%) (χ2 = 5.064; P = 0.024). Concerning living arrangements, 13% of PWD not living alone were aware of the project, while only 7% of PWD living alone were aware of it (χ2 = 4.393; P = 0.036). Among the enabling factors, 21% of Medical Aid program beneficiaries were aware of the project, compared to only 11% of National Health Insurance beneficiaries (χ2 = 8.361; P = 0.004). In addition, a greater proportion of PWD who had previously utilized community health services (17.3%) were aware of the project, compared to PWD who had not previously utilized such services (10.4%) (χ2 = 8.314; P = 0.004). More PWD who obtained health information from welfare centers or government institutions (22.4%) or health service centers (19.5%) were aware of the project, compared to PWD who obtained their information from family, neighbors, or mass media (χ2 = 36.545; P < 0.001). Among the need-based factors, awareness of the project was higher in respondents with severe disabilities (15.6%) than in respondents with less severe disabilities (9.2%) (χ2 = 9.682; P = 0.002). Lastly, more PWD in good subjective health (23.2%) were aware of the project, compared to PWD in poor health (8.2%) (χ2 = 27.124; P < 0.001).
Combination (demand-awareness)
On the service consumers’ perspective, we have focused on the gap of “demand” and “awareness” in terms of consumption of medical use. From that point of view, we considered the “aware but no demand” and “demand but poor awareness” among the combination of “demand” and “awareness.” 70.9% (n = 729) of the respondents expressed they had the demand for the pilot project but were not aware of it, but only 2.6% (n = 27) of the respondents expressed they were aware of the pilot project but having no demand for it.
The characteristics of respondents who had high demand but low awareness are shown in Table 2. Among the predisposing factors, more respondents aged < 20 years (72.5%) and ≥ 65 years (68.9%) expressed a need for the project but were not previously aware of it, compared to respondents aged 20–64 years (78.7%) (χ2 = 7.572; P = 0.023). Among the enabling factors, more PWD who obtained health information from family, neighbors, or mass media reported needing the project but were not previously aware of it (79.3%), compared to PWD who obtained information from health service centers (63.4%) (χ2 = 13.463; P = 0.009). Among the need-based factors, there were significant differences according to need for assistance with ADL, chronic disease, depression, subjective health status, and unmet medical care need. More respondents who needed assistance with ADL wanted to participate in the project but were not previously aware of it (76.5%), compared to respondents who did not need such assistance (67.0%) (χ2 = 10.962; P = 0.001). Greater proportions of PWD with chronic diseases (74.3% vs. 64.3%, χ2 = 11.046; P = 0.001), depression (77.3% vs. 64.9%; χ2 = 18.966; P < 0.001), poor subjective health (80.3% vs. 53.6%; χ2 = 42.626; P < 0.001), and unmet healthcare needs (82.7% vs. 67.8%; χ2 = 18.901; P < 0.001) wanted to participate in the project but were not previously aware of it.
Factors associated with demand and awareness
Logistic regression analysis was performed to identify factors that affected the demand for and awareness of the PHC pilot project for PWD, using Andersen’s behavioral model of health service use. When multicollinearity between variables occurs, it may affect the explanatory power and confidence interval of the model. When the mean variance expansion index (VIF) between all variables is ≥ 103536 or the tolerance value is < 0.2, collinearity problems may occur.37 Therefore, we confirmed the absence of multicollinearity by calculating the VIF and tolerance of the variables (VIF 1–2 for each variable, tolerance 0.55–0.95, mean VIF 1.33). The results of the logistic regression analysis are summarized in Table 3. The variable “proxy response to the questionnaire” was adjusted because it could have influenced the “demand”, “awareness” and “demand but poor awareness” responses.
Table 3
Multiple logistic regression of factors affecting “Demand,” “Awareness,” and “Demand but poor awareness” on the pilot project of primary health care for people with disabilities
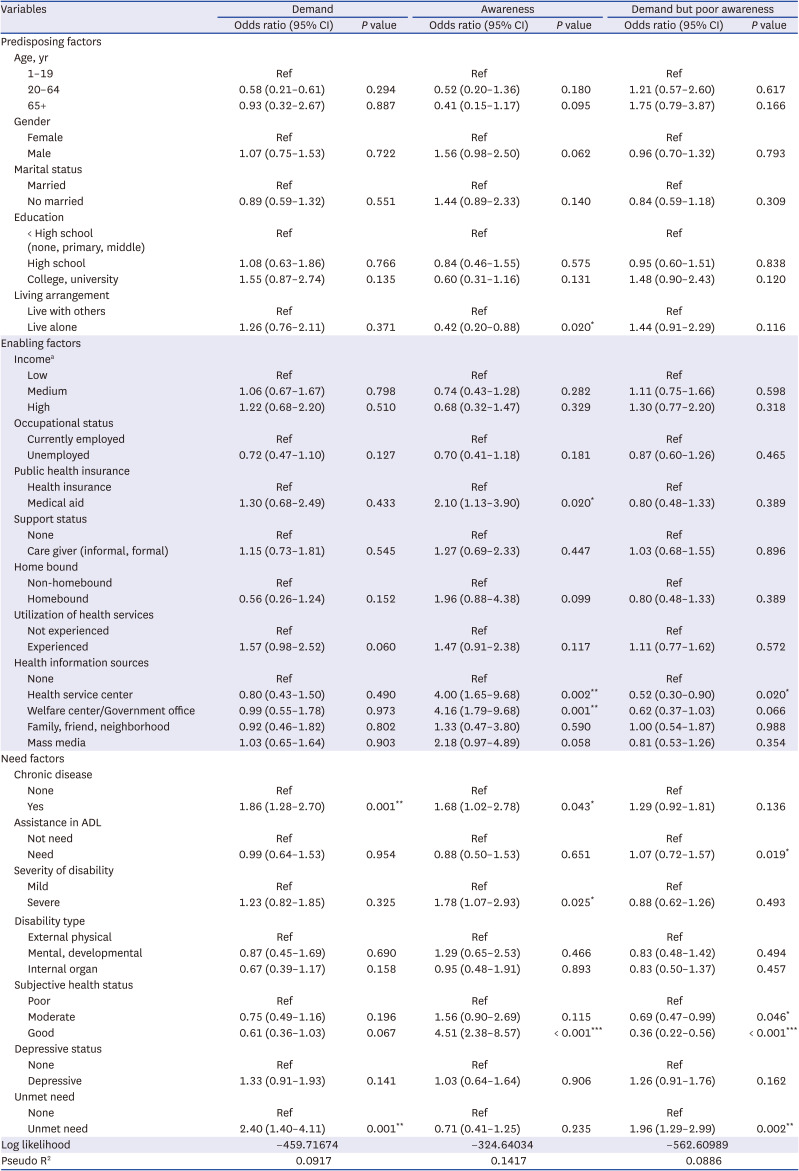
There were no significant variables among the predisposing factors and enabling factors. However, among the need-based factors, chronic disease and unmet need for medical care were significant variables. PWD with chronic diseases were more likely to express a need for the project than were PWD without such diseases (odds ratio [OR], 1.86; 95% confidence interval [CI], 1.28–2.70; P = 0.001); an unmet need for medical care also had a significant influence on demand (OR, 2.40; 95% CI, 1.40–4.11; P = 0.001). These independent variables explained 9.17% of the variation in demand for the project.
Among the predisposing factors, PWD who lived alone (OR, 0.42; 95% CI, 0.20–0.88; P = 0.023) had lower awareness of the project, compared to PWD who did not live alone. Among the enabling factors, medical aid program beneficiaries had higher awareness of the project (OR, 2.10; 95% CI, 1.13–3.90; P = 0.020) than did public health insurance beneficiaries. PWD who obtained health information from welfare centers, government institutions (OR, 4.16; 95% CI, 1.79–9.68; P < 0.001) or health service centers (OR, 4.00; 95% CI, 1.65–9.68; P = 0.002) had significantly higher awareness of the project, compared to PWD who had no health information sources. Lastly, among the need-based factors, chronic disease (OR, 1.68; 95% CI, 1.02–2.78; P = 0.043), severe disability (OR, 1.78; 95% CI, 1.07–2.93, P = 0.025), and good subjective health (OR, 4.51; 95% CI, 2.38–8.57; P < 0.001) significantly influenced awareness of the project. These independent variables explained 14.17% of the variation in awareness of the project.
There were no significant variables among the predisposing factors. However, among the enabling factors, PWD who obtained health information from health service centers expressed a significantly lower need for the project but were less aware of it, compared to PWD who had no health information sources (OR, 0.52; 95% CI, 0.30–0.90; P = 0.020). Among the need-based factors, PWD who needed assistance with ADL expressed a greater need for the project but were not previously aware of it, compared to PWD who did not need assistance with ADL (OR, 1.07; 95% CI, 0.72–1.57; P = 0.019). Also, good subjective health (OR, 0.36; 95% CI, 0.22–0.56; P < 0.001) and an unmet need for medical care (OR, 1.96; 95% CI, 1.29–2.99; P = 0.002) were significant variables. These independent variables explained 8.86% of the variation observed in the demand but poor awareness group.
DISCUSSION
This study investigated the demand for and awareness of the PHC pilot project for PWD, along with influencing factors, using Andersen’s behavioral model of health service use. The awareness of the project was remarkably low, while the demand was high. In particular, demand without awareness was influenced by age, education, health information sources, chronic disease, need for assistance with ADL, depression, subjective health status, and unmet need for medical care. Chronic disease and an unmet need for medical care had significant impacts on demand for the project. Furthermore, living arrangement, type of health insurance, health information sources, chronic disease, severity of disability, and subjective health status had significant impacts on awareness.
Overall, the demand for the project was high but awareness was very low, although 3 years have passed since the project was launched. Policymakers should carefully revise future goals of the project in response to these findings. In 2019, the government conducted a study to evaluate the pilot project, the study identified problems such as low fee-for-services that hinder supply-side incentives, poor detailed services, and limited beneficiaries (only for specific disability types).11 However, the scope of that study was limited in that it included only a small population of physicians and PWD. Our finding of remarkably low project awareness indicates that there was no opportunity to determine project effectiveness from a consumer perspective, prior to governmental evaluation of its effectiveness. Awareness of health services is an essential factor that influences their utilization38; many studies have emphasized a policy approach that separately considers each factor influencing awareness.122830 In particular, PWD have poor access to new policies or information because of limitations related to their disabling condition; thus, strategies to raise awareness must be planned from the perspective of such people.29 To promote PHC utilization, education and advertising programs such as public campaigns to improve awareness should be carried out preemptively; an active and individualized approach is urgently needed that considers the characteristics affecting awareness.
Although this pilot project is a service for people with severe disabilities, we found that the severity of disability did not affect demand for the program. For effective and efficient policymaking, need for healthcare service (based on professional value judgements) as well as demand should be considered.39 The pilot project designed to provide the chronic disease management services and management of disabling conditions for preventing secondary functional decline. However, since there are few primary care providers who can provide professional disability management in the local community, services have been mainly provided for the purpose of chronic disease management. Therefore, policymakers need to reconsider whether the current target population is suitable in terms of the demand and need for the service. For example, although there is demand and need for the service among people with chronic disease, they cannot use the service under the current initiative unless their disability is severe. Based on this unmet need, we suggest benchmarking the “primary care chronic disease management pilot program” as another pilot program for people with chronic disease, regardless of disability. However, this may be inefficient because of limited project budgets when service beneficiaries change. For example, when selecting service beneficiaries based on the presence of chronic diseases, inefficiencies may occur in relation to the provision of in-home care to people who can visit physicians easily. One solution may involve limiting in-home care services to PWD who have poor physical access to clinics or hospitals due to severe disability.
Notably, an unmet need for medical care has a significant impact on demand for the project. As the link between aging with a disability and disability with aging becomes clearer,40 an increase in chronic diseases among the population with disabilities is inevitable. Despite the need for more systemic health-focused healthcare because of the high prevalence of chronic diseases and the risk of secondary functional decline that is distinct from the original disabling condition,414243444546 PWD remain doubly disadvantaged because of their lack of access to healthcare. The PHC pilot project for PWD represents major progress toward improved healthcare access and solution of unmet need for medical care15; however, it is insufficient to address the unmet need for medical care among medically disadvantaged populations. Diverse institutions that provide health services for PWD should cooperate with each other; in particular, interdisciplinary cooperation, interprofessional teamwork, and community participation are key areas for success.4748 Nevertheless, most participating clinics function as a solo practice with only nursing assistants or receptionists for financial reasons; it is difficult for such clinics to hire a healthcare coordinator (currently, the registered nurse’s role), which is a key position within a team approach.121649 Thus, there is a need to expand support for the project at the level of the RHMCPWD, a coordinated health center for PWD in Korea, which already includes multidisciplinary personnel such as nurses, social workers, and therapists. In particular, it is important for the RHMCPWD to participate in the development, management, and connection of local resources.50 This will help to establish community-based, team-based PHC by leading community participation through a network with various local organizations that provide healthcare and welfare services for PWD.
Among the predisposing factors, we found that living alone had a significant effect on awareness of the project. Some previous studies have indicated that living alone has an impact on the awareness of health or welfare services,24 while others have not indicated such an impact.2832 However, these studies have been focused on older adults; it is difficult to compare their results with the present findings. Because the household composition of PWD is diverse (e.g., spouses, parents, brothers, sisters, and children), living arrangement may have a greater impact than marital status. Because of population aging and the current tendency towards deinstitutionalization, the proportion of PWD living alone is increasing (27% of the population in 2020).51 Accordingly, there is a need to identify methods to improve awareness for PWD living alone. In particular, this group experiences various physical and emotional barriers when using medical services; simply providing information about policies may not lead to use of the project. Therefore, more active guidance and individually tailored help should be provided to PWD living alone; such information could include other welfare services (e.g., transportation support to the clinic), rather than solely focusing on information about the project.
Among the enabling factors, the type of health insurance and health information sources were significant variables associated with awareness of the project. The influential role of the type of health insurance can be interpreted in relation to the out-of-pocket expenses that are incurred when using the project. Generally, many PWD use the program upon recommendation by a physician.1214 It might be difficult for physicians to give information about or recommend the use of the project to PWD with health insurance—the project is free for beneficiaries of a medical aid program but requires copayments for PWD with health insurance. This finding is consistent with a previous study52 where physicians participating in the project reported that the greatest obstacle to recommending enrollment was an increase in patient copayments. However, because inappropriate service costs are known to limit physician participation in the project,52 the government should re-evaluated the fees and copayments from various perspectives. In addition, careful consideration is needed regarding the acceptability of the additional cost when using the project, compared to the cost when using other non-participating clinics. Affordability directly affects access to healthcare. Acceptable costs include direct costs for services and opportunity costs associated with reduced revenue; the perceived cost may be higher than the actual service cost.53 There is also a need to consider that PWD have worse healthcare access for financial reasons, compared to individuals without disabilities.54
In terms of demand-side incentives, there should be clear advantages for PWD (i.e., the consumers) when using the project. In addition to costs, there must be clear differences in service quantity or quality, compared to the services provided by other non-participating clinics. Currently, the detailed services of the project include a comprehensive health assessment and care planning (compulsory), mid-term management (optional), education/consultation (optional), patient monitoring (optional), visiting care (doctor or nurse visiting, optional), and a voucher for a health check-up (optional). Because only the comprehensive health assessment and care planning aspects are compulsory, the other services are not widely available. Specifically, only 6% of all PHC institutions participating in the pilot program provide mid-term management or education/consultation services, which are considered services for continuous health management; only 4% of institutions provide in-home care services to improve poor physical accessibility.12 These results indicate that the PHC institutions participating in the project do not provide services that substantially differ from the services of other non-participating clinics. The prior study about experience of the disabled people participated in the PHC pilot project reported the limited services as a problem of the pilot project14. From the consumer perspective, there is no incentive to use a service that requires additional costs if there is no difference in service.
The finding that health information resources have significant impacts on awareness of the project is consistent with the results of previous studies.1931 In particular, the observation that PWD who receive information from health service centers (e.g., clinics, hospitals, and public health centers) were more likely to be aware of the project is supported by the previous finding that most PWD who utilized the project were referred by a physician.14 Furthermore, in the 2020 Survey on Persons with Disabilities conducted by the Ministry of Health and Welfare, mass media was the second most common source of healthcare information among PWD; thus, it may be effective to use mass media (in addition to health service centers) when promoting the project.
There were some limitations in our study. First, this study might have involved selection bias. Because the study focused on regional stratification without considering gender, age, or type of disability in relation to the sample composition, care is needed when interpreting the generalizability of the results. To alleviate selection bias, we conducted a large-scale survey in Gyeonggi-do, which has the largest population with disabilities. Second, we conducted a mobile-based survey during the coronavirus disease 2019 pandemic; the survey was not accessible to some PWD because of their disability characteristics or because of illiteracy. In addition, respondents may have misunderstood the contents of the survey; such misunderstanding might have been minimized in a face-to-face survey. We allowed parents or caregivers to respond on behalf of PWD, in an effort to address the limited accessibility of a mobile-based survey; we also added sufficient explanations for each question to encourage comprehension. Third, we only assessed overall demand for the services that PWD specifically want among the PHC pilot programs, such as in-home care and patient monitoring. Nonetheless, our findings are meaningful in that they can contribute to the successful implementation of the pilot project by identifying the gap between demand and awareness; they can also help to identify determinants in terms of predisposing factors, enabling factors, and need-based factors.
Our policy recommendations for the successful implementation of the PHC pilot project for PWD are summarized as follows. First, there is a need to carefully review the initiative and enact publicity programs to improve awareness of the service among PWD. Second, there is a need to clarify the policy objectives for each severity and type of disability. Accordingly, a detailed initiatives should be established that covers service content, service beneficiaries, service providers, service delivery methods, and costs. Third, because PHC physicians have a crucial role in the community-based health management system, they should cooperate with local health resources for PWD. For example, a service delivery system should be prepared in cooperation with the RHMCPWD. Additional studies are needed to assess the perspectives of PWD and the effectiveness of their healthcare services.
Notwithstanding the above suggestions, careful consideration is required because it may not be consistent with the results of our study when the survey is conducted with a larger sample of PWD considering the proportion by age and type of disability, or when the study is conducted in other regions. Therefore, there is a need for further research exploring the PHC access for PWD from both supply and demand sides with a representative large sample.
 XML Download
XML Download