

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Death by suicide is a major public health problem that affects not only the patients themselves but also their family members and surrounding relationships.12 As the rate of suicide has increased over the years, emergency department (ED) visit-related suicidal attempts have also increased.345
The ED often serves as a gatekeeper of public health safety nets in terms of screening and providing brief intervention for patients with social and medical public health problems. Various programs have been introduced to obtain better outcomes for patients visiting the ED after suicide attempts by linking the patient to psychiatric management and follow up beyond the ED.5678 In Korea, an ED-based brief psychiatric intervention and follow-up program were implemented from 2013 until the present day.9 However, the preventive effect of such programs on long-term outcomes has not been previously studied or reported.
In this retrospective analysis, we traced the long-term survival outcome and the cause of death of patients visiting the ED after unsuccessful suicide attempts using the national death certificate registration database. We also compared the outcome of patients based on compliance with ED-based psychiatric intervention programs to evaluate the effectiveness of the program.
Go to : 
METHODS
Study design and purpose
This study is a retrospective observational study. The purpose of the study was to investigate the survival outcome of patients visiting the ED after suicide attempts according to compliance with ED-based psychiatric screening and brief intervention programs.
Study setting
In Korea, an ED-based psychiatric screening and intervention program for suicide attempts or self-harm injury was initiated in 2013. This program was funded by the Korea Suicide Prevention Center (KSPC) under the Department of Health and Welfare in Korea.9 EDs participating in the program are designated “Psychiatric Crisis Response Centers” (PCRC) by the KSPC. PCRCs are funded to hire 1–3 social workers to operate the program in their ED. Most centers are operated in a 2-shift system (day/evening) and are not operational during nighttime. The operation hours and process differ for each PCRC. Currently in 2022, 60 PCRCs are operated throughout the nation.10
ED-based screening and intervention program
During the PCRC operation hours, a social worker on duty screens the list of patients visiting the ED for enrollment in the program. The social worker visits possible candidates of the program for a face-to-face interview. After interviewing the patient, the social worker explains the follow-up program. If the patient agrees to participate in the program, informed consent is completed before ED discharge for hospital admission and transfer to another hospital or home discharge. For patients who agreed to join the program, the social workers proceed with case management sessions during the next few weeks of ED discharge. During the case management sessions, the social worker asks about the patient’s well-being, compliance with the medication, outpatient clinic schedules, etc. The social worker also makes inquiries regarding the social needs of the patient and helps them with needs, such as paperwork. Additionally, the patient’s information was transferred to a local community mental health center, where the patient could be followed up routinely after case management by local social workers. Case management is typically performed in 4 sessions, either by face-to-face or telephone interviews based on the patient’s preference.
Study population
Patients visiting 27 ED PCRCs from January 2013 to August 2015 with chief complaints resulting from suicidal attempts during the operation hour were enrolled. The patients were divided into 2 groups according to agreement to participate in the follow-up case management program. Patients who were screened as possible candidates of the program but could not be reached by the social worker or patients denied meeting the social worker even for the initial process of program explanation and asking for the informed consent were excluded.
Database
For all possible candidates of the intervention program, the social workers collect general information and complete the standard PCRC registry. The completed registry from each PCRC was transmitted to the KSPC headquarters for gathering and processing. For research purposes, the KSPC sent the registry database to Statistic Korea,11 where all official national statics data in Korea are processed and handled. The PCRC registry was then merged with the National Death Certificate database in Statistics Korea and sent back to the PCRC for research purposes after eliminating personal identifiable information for privacy issues. The merged database only contains information regarding the number of case management sessions and dates and causes of death if the patient died during the observational period (January 2013 to December 2018). Because personal identifiable information was eliminated in the merged dataset, it could not be reattached to the original PCRC registry database, and detailed demographics were analyzed based on the death of the patient during the observational period.
Variables and outcome measurements
The PCRC registry contains demographic characteristics (age, sex, occupation, companion to ED visit, marital status, health insurance), information regarding suicide attempts (methods, place, any previous suicide attempt, alcohol consumption before event), psychiatric consultation, psychiatric diagnosis in ED and information regarding case management (number of case management sessions).
The database that was obtained upon merger with the national death certificate database contains only 3 variables, including the number of case intervention sessions and information regarding the death of the patient (date of death and cause of death in International Classification of Diseases [ICD]-10 code) if the patient was reported to die during the observation period.
The outcome measure in the study was death caused by suicide during the observation period. We defined death caused by suicide if the ICD code for cause of death included an ICD-10 code corresponding to suicide attempts 2, such as self-harming, poisoning and hanging (Table 1).

Table 1
List of ICD-10 codes that correspond to suicide attempt
![]()
Statistical analysis
Basic characteristics of the study population were described and compared according to compliance with the follow-up program. Categorical variables were compared with the χ2 test, and continuous variables were compared with Student’s t-test. Unadjusted crude mortality rate by suicide according to the number of case management sessions participated by the patient was plotted. All statistical analyses were performed using Stata ver. 16.1 (StataCorp, College Station, TX, USA).
Ethics statement
This study was reviewed by the Institutional Review Board (IRB) of the investigator’s hospital, and informed consent was waived (IRB No. 07-2021-15).
Go to :
RESULTS
During the study period, 12,544 patients who visited the ED after suicide attempts in 27 hospitals during the study period were enrolled. The demographic characteristics of the initially enrolled patients are summarized in Table 2. Among the total population, 5,455 (43.5%) participated in at least one case management session after discharge from the ED (Fig. 1). No significant differences in age or sex were noted between the two groups. The most frequent method of suicide attempt was ingestion of sedative/antidepressant/hypnotics in both groups. (37.2% in the compliance group and 29.9% in the noncompliance group) Proportion of patient who visited ED alone was higher in the non-compliance group (17.7% vs. 14.4%) and proportion of patients who refused psychiatric consultation in ED was also higher in the non-compliance group (24.9% vs. 14.8%).
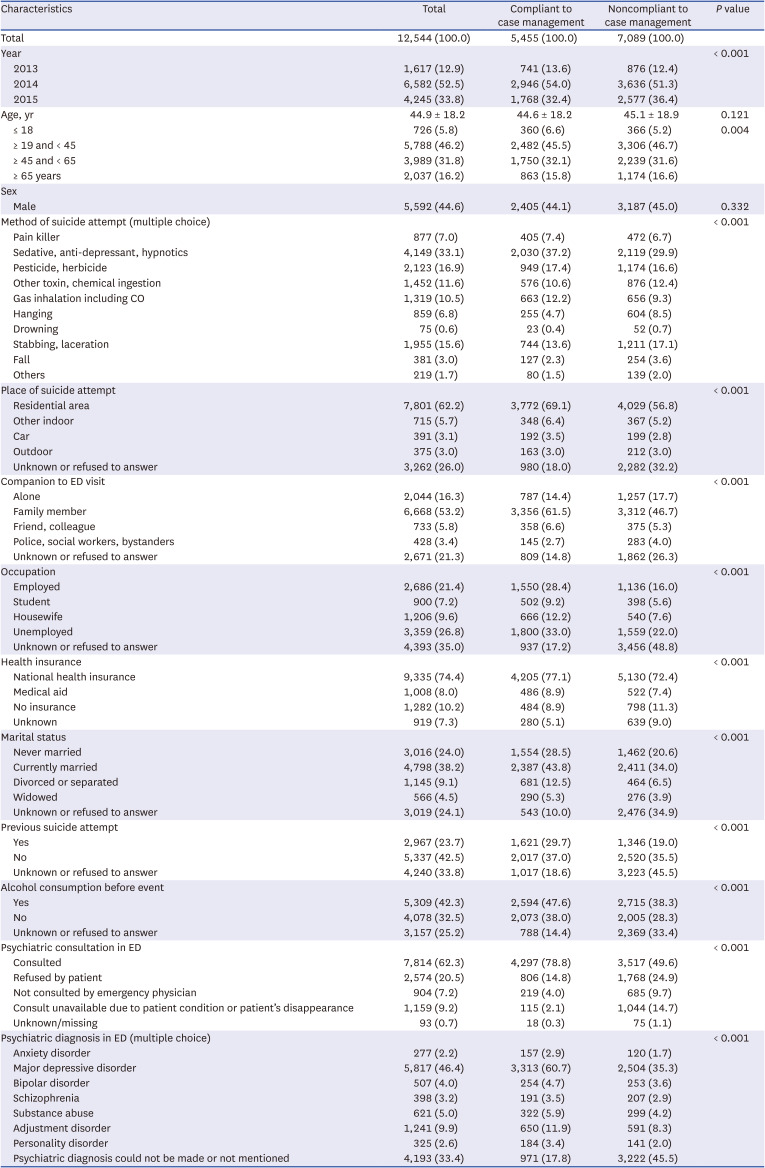
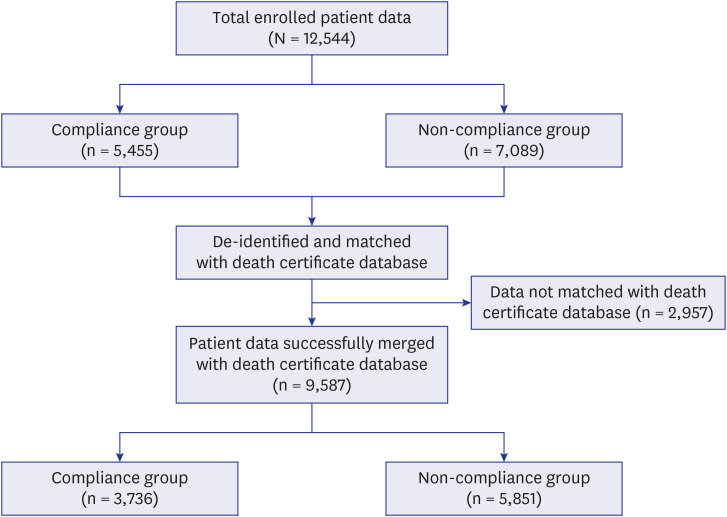
Table 2
Demographic characteristics of patients enrolled in the study based on compliance with the program
![]()
The total rate of death and rate of death according to the cause are shown in Table 3. All-cause mortality was significantly higher in the noncompliance group. (9.3% vs. 17.3%, P < 0.001). Death by suicide was also higher in the noncompliance group (4.5% vs. 12.4%, P < 0.001); however, death caused by factors other than suicide did not different between groups. (4.8% vs. 4.9%, P = 0.906). The mortality rate by suicide based on the number of case management sessions that the patients participated in is shown in Fig. 2.

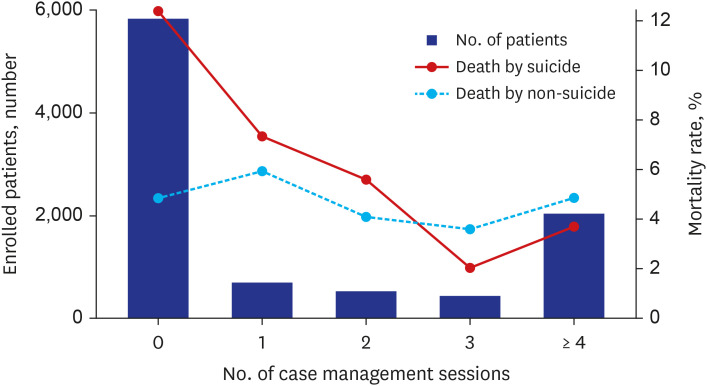
Table 3
Long-term survival outcome of patients based on program compliance
![]()
Go to :
DISCUSSION
The results of our retrospective analysis showed that the mortality rate was lower in patients who complied with the ED-based psychiatric brief intervention and follow-up program. Previous studies have reported the effectiveness of the ED-based psychiatric intervention program,67812131415 however, most of the studies reported short-term outcomes of the program. We believe our study is the first to show the long-term outcomes of ED-based psychiatric intervention programs for patients visiting EDs after suicide attempts. Based on our results, we suggest that ED-based psychiatric intervention programs are an effective intervention to reduce death from suicide and should be expanded to more EDs around the country.
ED is an important place for public health interventions. Especially for patients attempting suicide and self-harming injury, the ED could be a starting point for public intervention programs that could be continued for community service, as noted in our study. In our program, the social workers are recommended to proceed 4 case management sessions with the patient. During the case management sessions, the social workers provided social, psychiatric and emotional support to the patients. The social workers check on the patient, assessing their well-being after ED discharge and outpatient clinic appointments with their primary psychiatric doctors, and they also connect them to community psychiatric support centers for continued support in the community where they live. These types of support during the vulnerable period after suicide attempt might prevent additional suicide attempts and even death from suicide.
Proportion of lesser fatal suicidal methods such as drug ingestion was higher in the compliance group whereas proportion of fatal suicidal methods such as fall and hanging was higher in the noncompliance group. The reason for the difference in distribution of suicidal attempt method might be a result of different level of patient’s aggressiveness. A retrospective study showed drug poisoning was the most common suicidal method in failed suicidal attempt, but it was the least common method of completed suicides.16 Patient with higher level of aggressiveness who selected the more lethal method of suicidal attempt might less compliance to the program and therefore eventually died from completed suicide.
Patient who attempts suicide or self-injury usually visits ED after the incidence, whether the visit is voluntarily or unintentionally by other people. Therefore, ED staffs including doctors and nurses often manage the patients with psychiatric issues.17 However, usually ED staffs focus on the diagnosis and treatment of physical injury and show negative attitude to the patients with psychiatric issues.18 To fulfill the unmet need of emotional and social support that the ED staffs can not provide to the patient in a chaotic ED, strategic reinforcement with trained social worker like PCRC program is needed. Based on our study results we believe expansion of ED-based intervention program for psychiatric patients should be considered in more EDs.
In summary, patients who complied with follow-up case management sessions as part of an ED-based brief psychiatric intervention and follow-up program showed lower long-term mortality rates by suicide. Considering the growing volume of patients visiting EDs after suicide attempts, expanding ED-based intervention programs and developing regionalization strategies might decrease mortality from suicide.
Our study has a few limitations. To protect the personal information of the patients, the database that was generated by merger with death certificate data included variables that were all censored except the number of case management sessions and the variables regarding the death of the patient. Detailed analysis regarding the association between the patient characteristics and the compliance to the program, as well as the timing of death and follow-up period could not be performed because we could not match the initial database with demographics to the merged database with death outcome. The increased mortality in the noncompliance group was potentially exaggerated because it might have resulted from the subacute complication of initial suicidal attempt during admission after ED discharge, which cannot be identified in our database. Additionally, selection bias potentially occurred, and the operation duration and enrollment process were not identical across PCRCs of 27 different hospital EDs. We could also not identify 2,957 patients (Fig. 1) whose data did not merge with the national death certificate database. We believe that mistakes made during the recording of personal security numbers might be the main cause of the inability to match; however, we could not analyze the distribution of excluded patients due to censoring. Additionally in noncompliance group, there were many variables marked as “Unknown or refused to answer” (Table 2). Although our primary population were patient who underwent initial interview process with the social worker, larger proportion of noncompliance group refused or did not answer to basic interview questions causing significant proportion of missing values in multiple variables. Lastly, the outcome measure (death by suicide) was defined according to the ICD-10 code (Table 1). Although using T-codes for are usually used for ED visits after suicide, some of the death with T-codes might not be death from intentional injuries or suicide.
To overcome the listed limitations of our study, a prospective cohort study would be most ideal. However, due to the nature of the population and disease entity, designing a prospective study with informed consent to all eligible patients was practically impossible given the chaotic nature of the ED. We believe our data processing and analysis was an acceptable alternative method to show the effect of the program despite a few methodological limitations.
In conclusion, patients who complied with follow-up case management sessions as part of an ED-based brief psychiatric intervention and follow-up program showed lower long-term mortality rates by suicide. Considering the growing volume of patients visiting EDs after suicide attempts, expanding ED-based intervention programs and developing regionalization strategies might decrease mortality from suicide.
Go to :
 XML Download
XML Download