

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Asthma and chronic obstructive pulmonary disease (COPD) are both airway diseases with similar clinical manifestations, despite different pathophysiologies. Asthma-COPD overlap (ACO) is a condition that is characterized by overlapping clinical features from both diseases.1 There have been increasing numbers of studies regarding the classification and clinical features of ACO.2 However, there remains no consensus regarding definite diagnostic criteria; the reported prevalences of ACO vary widely according to the diagnostic criteria used.3456789 Although there have been many reports of studies in asthma and COPD cohorts, there have been few reports regarding the prevalence of ACO in combined COPD and severe asthma cohorts.
Asthma and COPD are heterogeneous disorders with variable phenotypes, and there are several phenotypes of ACO. To our knowledge, there have been few studies of the clinical characteristics of ACO phenotypes.21011 There have been several attempts to classify the phenotypes of ACO, but a consensus has not yet been reached concerning appropriate classification criteria. Patients with ACO can be classified according to differences in ACO phenotype, mainly on the basis of eosinophilic inflammation and smoking history.12 Using these criteria, COPD patients have been classified and compared according to phenotype, revealing differences in clinical features.10 There have been no studies in which participants were divided into different phenotype groups in cohorts of severe asthma and COPD patients.
This study was performed to analyze the prevalence of ACO in COPD and severe asthma cohorts. In addition, this study compared baseline characteristics among ACO patients according to phenotype.
METHODS
Study population
Patients with COPD were prospectively enrolled into the Korean COPD subgroup study (KOCOSS) cohort, a multicenter cohort study of COPD patients recruited from 54 medical centers in South Korea. In this study, we extracted KOCOSS data from the cohort enrolled between April 2012 and September 2020. Inclusion criteria were South Korean patients age ≥ 40 years with post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) < 70% of the normal predicted value.
Patients with severe asthma were prospectively enrolled into the Korean Severe Asthma Registry (KoSAR) of the Korean Academy of Asthma, Allergy, and Clinical Immunology, the Working Group on Severe Asthma. The KoSAR is a prospective multicenter observational study for adult severe refractory asthma from 31 institutions in Korea.1314 In total, 832 patients with severe asthma enrolled between January 2010 and February 2021 were included in this study. The inclusion criteria were patients with severe asthma, defined as follows: treatment by asthma specialists under regular follow-up for at least 1 year or inability to consistently achieve a well-controlled status after Global Initiative for Asthma treatment steps 4 or 5; alternatively, achievement of well-controlled status after Global Initiative for Asthma treatment step 4 or 5 but presentation to an emergency department more than once annually, receipt of steroid burst treatment more than three times annually, asthma worsening on tapering of oral corticosteroids or inhaled corticosteroids, or near-fatal asthma attack onset at any time in the past.
Definitions
ACO was defined in accordance with the updated Spanish criteria.15 In the COPD cohort, ACO was defined as bronchodilator response (BDR) ≥ 15% and ≥ 400 mL from baseline or blood eosinophil count (BEC) ≥ 300 cells/μL. In the severe asthma cohort, ACO was defined as age ≥ 35 years, smoking ≥ 10 pack-years, and post-bronchodilator FEV1/FVC < 0.7.
Classification of ACO phenotype
We classify patients into light smokers (more asthma feature predominant) and moderate to heavy smokers (more COPD feature predominant) based on their 20 pack-year smoking history.1617 BEC 300 cells/uL is well known criterion for eosinophilic inflammation.1819 An eosinophilic COPD phenotype based on a peripheral BEC of at least 300 cells/μL is associated with an increased risk of acute exacerbations of COPD.2021 Patients with ACO were divided into four groups according to smoking history (threshold: 20 pack-years) and BEC (threshold: 300 cells/μL): group A (smoking 10–20 pack-years and BEC ≥ 300 cells/μL); group B (smoking 10–20 pack-years and BEC < 300 cells/μL); group C (smoking ≥ 20 pack-years and BEC ≥ 300 cells/μL); and group D (smoking ≥ 20 pack-years and BEC < 300 cells/μL). Patients with BEC ≥ 300 cells/μL at the time of enrollment were classified as the high blood eosinophil group. Characteristics were analyzed and compared among the four groups.
Clinical evaluation
Demographic information—e.g., sex, age, smoking history, comorbidities, body mass index (BMI), and questionnaire results (asthma control test and COPD Assessment Test [CAT; GlaxoSmithKline Services, Brentford, UK])—was collected along with the results of pulmonary function and laboratory tests, as well as details concerning medication use.
Statistical analysis
Categorical data were analyzed using the χ2 test or Fisher’s exact test. For normally distributed data, Student’s t-test or one-way analysis of variance was used for between-group comparisons. For non-normally distributed data, the Mann–Whitney U test or the Kruskal–Wallis test was used for between-group comparisons. All statistical analyses were performed using SPSS (version 23.0; SPSS Inc., Chicago, IL, USA). In all analyses, P < 0.05 was considered to indicate statistical significance.
Ethics statement
For both KOCOSS and KoSAR patients, written informed consent was obtained from all study participants. Ethics approval for the both cohorts was obtained from the Institutional Review Board of Konkuk University Medical Center (IRB No. KHH1010338). We also received approval from each center to use clinical record for their subjects for the study while maintaining patient confidentiality with regard to the data. The official name of each approving ethics committee is listed in Supplementary Fig. 1.
RESULTS
Patients and comorbidities
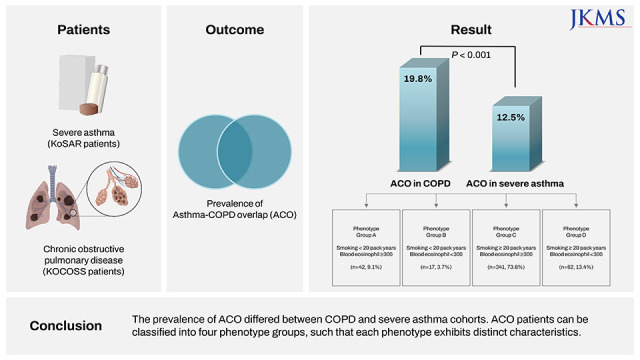
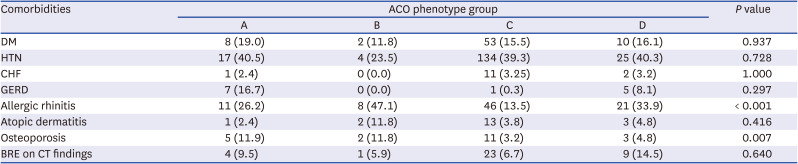
The prevalence of ACO significantly differed between the COPD and severe asthma cohorts (19.8% [365/1,839] vs. 12.5% [104/832], respectively; P < 0.001) (Fig. 1). In total, 462 ACO patients were divided into four groups: group A, 42 (9.1%); group B, 17 (3.7%); group C, 341 (73.8%); and group D, 62 (13.4%) (Supplementary Fig. 1). Table 1 shows the baseline characteristics of the four phenotype groups. The mean age significantly differed among groups (P < 0.001). Patients in Group C were oldest and patients in group B were youngest. The proportion of men significantly differed among groups (P < 0.001). The proportion of men was high in group C (almost all patients were men in that group); group B had the highest proportion of women. Smoking histories significantly differed between groups C and D (48.99 ± 23.95 and 44.83 ± 29.88 pack-years, respectively) and between groups A and B (15.22 ± 3.33 and 13.92 ± 3.01 pack-years, respectively; P < 0.001 for each pairwise comparison). There was no statistical difference in the rate and the incidence of acute exacerbation. Among all patients, 39.0% had hypertension and 15.8% had diabetes, but these parameters did not significantly differ among groups. The proportion of allergic rhinitis significantly differed among groups (P < 0.001); group B exhibited the highest proportion (40%). There were no significant differences in congestive heart failure, gastroesophageal reflux disease, atopic dermatitis, or osteoporosis among groups (Table 2).
Fig. 1
Flow diagram for participant enrollment.
BD = bronchodilator, BDR = bronchodilator response, COPD = chronic obstructive pulmonary disease, KOCOSS = Korean COPD subgroup study, KoSAR = Korean Severe Asthma Registry.
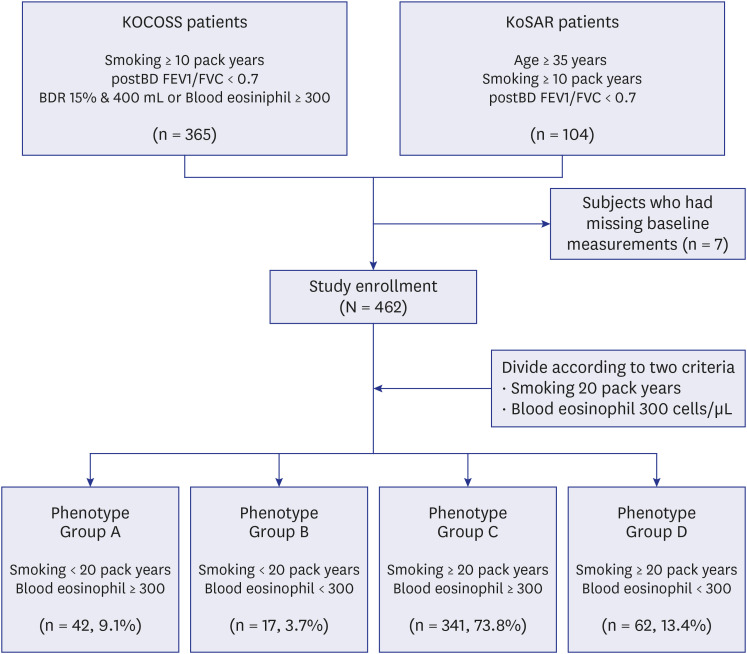
Table 1
Demographic and clinical characteristics of ACO phenotype groups (N = 462)
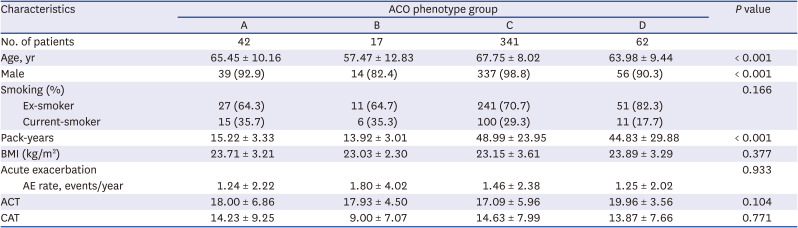
Table 2
Comorbidities in ACO phenotype groups
Pulmonary function tests and laboratory findings
Table 3 shows the results of pulmonary function tests and laboratory findings among the four phenotype groups. Post-bronchodilator FVC (L, % predicted) and FEV1 (L, % predicted) did not significantly differ among the four groups. The FEV1/FVC ratio was lower in groups C and D (moderate to heavy smokers) than in groups A and B (light smokers). BDR (%) was lowest in group A and highest in group D; BDR (mL) was lowest in group C and highest in group B. The differences in BDR (mL) and BDR (%) were statistically significant (P < 0.001 for both comparisons among groups). There were no differences in white blood cell counts between groups, but there were significant differences among groups in BEC (P < 0.001). BDR was lower in the high BEC group, but this difference was not statistically significant. Immunoglobulin E levels did not significantly differ among the four groups (P = 0.869). FeNO was measured in some patients, and there was no statistical significance (P = 0.235).
Table 3
Lung function and laboratory findings in ACO phenotype groups
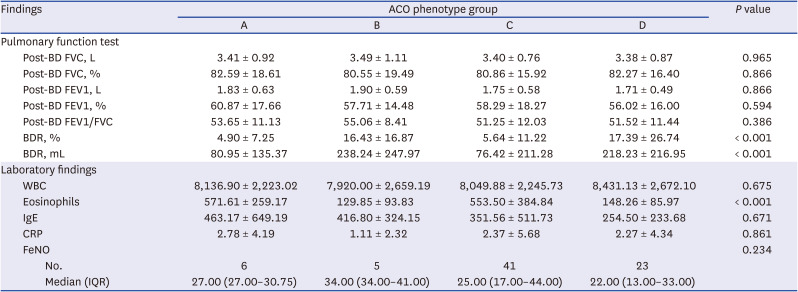
Data are expressed as mean ± standard deviation not otherwise specified.
COPD = chronic obstructive pulmonary disease, ACO = asthma-COPD overlap, BD = bronchodilator, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, BDR = bronchodilator response, WBC = white blood cells, IgE = immunoglobulin E, CRP = C-reactive protein, FeNO = fractional exhaled nitric oxide, IQR = interquartile range.
Inhaler use
Table 4 shows the use of inhalers in the four phenotype groups. The patterns of inhaler use differed among the four phenotype groups. The frequency of inhaled corticosteroid (ICS)-long-acting beta agonist (LABA) use was highest in group C, followed by group A. The difference in ICS-LABA use among the four groups was statistically significant (P < 0.001). The frequency of ICS-LABA-long-acting muscarinic antagonist (LAMA) use was highest in group C, followed by groups A, D, and B. There was no significant difference in triple inhaler use among the four groups (P = 0.196).

Comparison of characteristic of ACO patients in KOCOSS and KoSAR
Table 5 shows baseline characteristics and the results pulmonary function tests of ACO patients in KOCOSS and KoSAR. The mean age is significantly higher in KOCOSS than KoSAR (P < 0.001). And KOCOSS patients had more exposure to smoking. However, except for BDR (mL), there was no significant difference in the results of pulmonary function tests. Table 6 shows comparison of proportion of ACO phenotype group between KOCOSS and KoSAR. In KOCOSS, the ratio of group C was the highest, and in KoSAR, the ratio of group D was the highest.
Table 5
Comparison of characteristics of ACO patients in KOCOSS and KoSAR
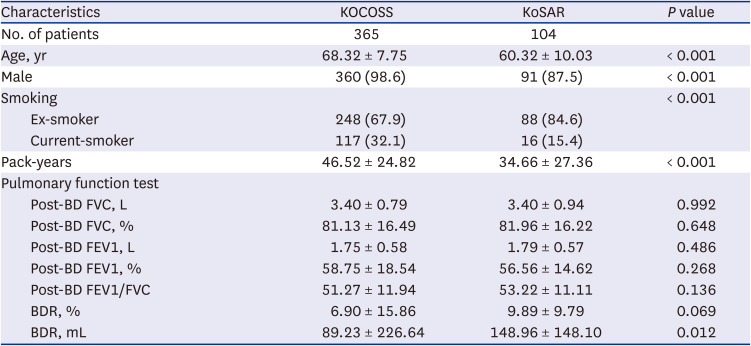
Data are expressed as mean ± standard deviation or number (%).
COPD = chronic obstructive pulmonary disease, ACO = asthma-COPD overlap, KOCOSS = Korean COPD subgroup study, KoSAR = Korean Severe Asthma Registry, BD = bronchodilator, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, BDR = bronchodilator response.

DISCUSSION
Gibson et al.22 first proposed the definition of ACO using the combined physiological criteria for COPD and asthma. Since then, various alternative definitions of ACO have been proposed.91523 Moreover, several studies investigated the prevalence of ACO using these various definitions.24 The opinion of a specialist, albeit subjective, may also be an important criterion in ACO diagnosis.24 In another study, smoking history was considered the most important factor by a specialist in ACO diagnosis.14 Therefore, this study examined the prevalence of ACO using the updated Spanish ACO guidelines, which require a smoking history ≥ 10 pack-years for definitive diagnosis. To our knowledge, this is the first study to investigate the prevalence of ACO in two combined nationwide cohorts. The results showed that the prevalence of ACO was significantly higher in the COPD cohort than in the severe asthma cohort (19.8% vs. 12.5%, respectively, P < 0.001). The prevalence in the COPD cohort was comparable with the prevalence reported in previous studies; in contrast, the prevalence in the severe asthma cohort was lower than in previous studies where smoking history was not an essential component of the diagnosis of ACO.1314
ACO has characteristics of both asthma and COPD, and its phenotype is defined based on the predominant feature. Therefore, many studies have attempted to classify ACO patients according to their phenotype. One study classified ACO patients based on smoking and wheezing,11 while another classified ACO patients into four phenotypes using clustering analysis according to age, BMI, exacerbation, smoking, dyspnea score, and comorbidities.2 Rhee suggested classification of ACO patients into four phenotypes based on simple BEC and smoking history.12 These criteria are similar to the updated Spanish ACO guidelines used in the present study. Analysis of single-center COPD patients based on the suggested classification revealed differences in lung function, medication use, exacerbation, and baseline characteristics.10 In the present study, COPD and severe asthma patients were classified according to ACO phenotypes. Group C (smoking ≥ 20 pack-years and BEC ≥ 300 cells/μL) comprised the largest proportion, similar to previous findings. Furthermore, the phenotype of patients in group C was consistent with ACO, because those patients exhibited features of both asthma and COPD. A notable finding in this study was the distinct inhaler use pattern in each group. Consistent with previous studies, ICS-LABA (a treatment mainly used in asthma) was the most common drug combination overall; it was also used at different frequencies by patients in each phenotype group. There was an asthma-predominant group and a COPD-predominant group; specialists prescribed ICS-LABA only or ICS-LABA-LAMA differently for these groups. For each ACO phenotype, factors related to asthma were investigated; differences were observed in the proportions of features suggestive of asthma for each type. The similarity between groups A and C may reflect endotype is more important than smoking history. Although smoking pack years differs significantly between groups A and C, other characteristic are similar. Interestingly, CAT scores are both high in two groups. This may suggest eosinophilic inflammation plays an important role in ACO.
The multicenter and nationwide enrollment of ACO patients within a large population of asthma and COPD patients represents a major strength of the present study, leading to analysis based on large cohorts of severe asthma and COPD patients. In addition, both cohorts were well controlled with few missing values and high data reliability. Our study provided valuable information regarding the prevalence of ACO and insightful data concerning the characteristics of different ACO phenotype groups. Phenotype classification based on underlying disease physiology is important for the proper management of individual patients.12
This study had several limitations. First, the majority of patients in this study were men. However, the Korean statistics in 2019 indicated that smoking rates were 35.3% and 3.7% in adult men and women, respectively. Overall, the smoking rate of women in Korea is very low; therefore, the relative number of women among patients in this study was not very small. Second, the study may have been subject to bias because all patients were enrolled from specialist centers; the results may have been biased toward patients with higher disease severity. Third, various severity of patients would have been included in COPD cohort while only severe asthma patients would have been included in Severe asthma cohort. However, for the reasons mentioned earlier, more severe COPD patients would also have been included in COPD cohort.
In conclusion, the prevalence of ACO differed between COPD and severe asthma cohorts. ACO patients can be classified into four phenotype groups, each of which showed different characteristics. However, further studies regarding ACO phenotypes are required.
 XML Download
XML Download