

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the outbreak of coronavirus disease 2019 (COVID-19) in December 2019, several studies undertaken in different regions and countries around the world have revealed sex-based differences of this disease. Whilst males and females appear to be equally vulnerable to contracting the disease, there are differences in the severity of the infection, with males suffering more severely.1 Multiple potential factors have been proposed to account for such sex-based difference including biological factors, such as hormones, immunity, enzymes, genetic diversity and lifestyle factors.23 Some studies have focused on androgen and suggested that androgen in males might have influenced immunity and made males more vulnerable to severe infection or that hormones might have potentially increased the virulence of COVID-19.45
Thus far, only three cohort studies have explored the relationship between androgen deprivation therapy (ADT) and the severity of COVID-19,456 showing inconsistent results. Compared to patients not receiving ADT, those who have received ADT are four times less likely to experience severe COVID-19 infection. The risk of severe infection is five times less in patients who are receiving ADT for prostate cancer than in patients who have other cancers.45
The evidence provided by these studies suggests that the severity of COVID-19 is intensified by elevated concentrations of androgen. Moreover, ADT could be an alternative treatment for severe COVID-19 in addition to currently introduced vaccines and remedies. More research studies are needed to determine whether there is a relationship between androgen level and the severity of COVID-19. If such relationship is confirmed, responsible biochemical and molecular mechanisms involved in such relationship need to be elucidated.
This study performed a systematic review of published cohort studies. The aim of this study was to characterize the relationship between ADT and the severity of COVID-19 in patients with prostate cancer. It considers the quality of cohort studies’ methodologies in relation to the existing body of knowledge about biochemistry and immunology.
MATERIALS AND METHODS
This systematic review is registered in PROSPERO, CRD 42021235232.
Search strategy
In the present study, PubMed, Embase, and Cochrane Library databases were systematically searched for English language studies published from the inception of each database until February 31, 2020. All studies that examined the effect of ADT on the risk of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) in patients with prostate cancer were identified. Search terms consisted of MeSH terms of “prostate cancer,” “coronavirus infections,” “SARS-CoV-2,” and “androgen deprivation therapy.” Natural headings in the abstract or title included “prostate cancer,” “androgen-deprivation,” “androgen deprivation therapy,” and “SARS-CoV-2.” Searches were limited to human and English studies. All study designs were searched. All conference and meeting abstracts and non-English articles were excluded regardless of relevance.
Trial inclusion and exclusion criteria
The PICOS (participants, interventions, comparators, outcomes, and study design) approach was used to assess the eligibility of identified studies in accordance with the PRISMA guidelines.7 Human research studies on patients with prostate cancer and the effect of ADT on SARS-CoV-2 infection with outcomes of the present study were included. Exclusion criteria were: non-human study, no control group, and non-English study. Final included articles were determined through assessment and discussion among all authors.
Data extraction
Two independent authors extracted the data of included studies using a predesigned form. Any conflicts between them were resolved via discussion and consensus. Final included studies were agreed by all authors. Extracted data included the first author, publication year, country, study design, treatment and control groups, number and mean age of patients, definition of ADT, inclusion and exclusion criteria, follow-up period, and outcomes.
Types of interventions and outcomes
Patients with prostate cancer who were treated with ADT were assigned to the treatment group while those patients who were not treated with ADT were assigned to the control group. Patients in both groups had undergone a SARS-CoV-2 test. The primary outcome was SARS-CoV-2 positivity. Secondary outcomes were hospitalization, intensive care unit (ICU) admission, and death.
Study quality assessments and quality of evidence
The risk of bias in each included study was evaluated using ROBINS-I (Risk Of Bias In Non-randomized Studies of Interventions) tool. Bias domains included in the ROBINS-I tool: 1) confounding, 2) selection of participants for the study, 3) classification of interventions, 4) deviations from intended interventions, 5) missing data, 6) measurement of outcome, and 7) selection of reported result.8 Based on judgements for each bias domain, the overall risk of bias was classified into four levels: ‘Low,’ ‘Moderate,’ ‘Serious,’ and ‘Critical.’
The certainty of evidence reported in the present study was assessed using Grading of Recommendations, Assessments, Developments, and Evaluation (GRADE).9 The GRADE system assesses the methodology, precision, consistency of results, directness, and risk of publication bias constitute. Based on these five criteria, the certainty of evidence was assessed at four levels: high, moderate, low, and very low.
Statistical analysis
We performed meta-analysis for dichotomous outcomes to compare the efficacy of ADT with respect to outcomes using the random effects model. Outcomes were evaluated as risk ratios (RRs) in stratified 2 × 2 contingency tables. Results are reported as RRs and 95% confidence intervals (CIs) of included studies.
Statistical heterogeneity among included studies was identified by Cochran Q statistic and I2 statistic. A P value < 0.05 of the Cochran Q statistic or an I2 statistic > 50% suggested significant heterogeneity.10 We used funnel plot to evaluate publication bias. Symmetry reversal funnel diagrams meant no publication bias.
Meta-analysis was performed using Review Manager v.5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark, 2008). All P values were two-sided and P < 0.05 was considered statistically significant.
RESULTS
Systematic review process
Fig. 1 shows the process of systematic review in the present study. Literature searches found a total of 18 studies, with 13 remaining after removing duplicates. After reviewing titles and abstracts, 10 were removed as they were Editorials, letters, review articles, or case reports. The remaining three full-text articles were assessed for eligibility for final inclusion. Through this process, all three studies were included in qualitative synthesis.456 However, one study had no control group. It was excluded. Finally, the present study included two studies for quantitative synthesis,56 with a total of 44,213 patients. Detailed information of each included study is shown in Table 1.

Table 1
Characteristics of eligible studies
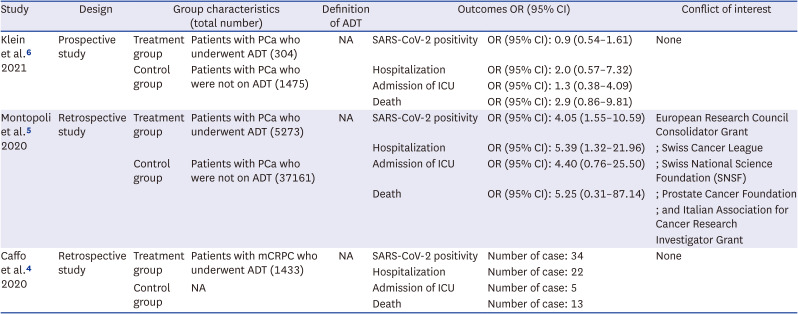
| Study | Design | Group characteristics (total number) | Definition of ADT | Outcomes OR (95% CI) | Conflict of interest | ||
|---|---|---|---|---|---|---|---|
| Klein et al.6 2021 | Prospective study | Treatment group | Patients with PCa who underwent ADT (304) | NA | SARS-CoV-2 positivity | OR (95% CI): 0.9 (0.54–1.61) | None |
| Control group | Patients with PCa who were not on ADT (1475) | Hospitalization | OR (95% CI): 2.0 (0.57–7.32) | ||||
| Admission of ICU | OR (95% CI): 1.3 (0.38–4.09) | ||||||
| Death | OR (95% CI): 2.9 (0.86–9.81) | ||||||
| Montopoli et al.5 2020 | Retrospective study | Treatment group | Patients with PCa who underwent ADT (5273) | NA | SARS-CoV-2 positivity | OR (95% CI): 4.05 (1.55–10.59) | European Research Council Consolidator Grant |
| Hospitalization | OR (95% CI): 5.39 (1.32–21.96) | ; Swiss Cancer League | |||||
| Control group | Patients with PCa who were not on ADT (37161) | Admission of ICU | OR (95% CI): 4.40 (0.76–25.50) | ; Swiss National Science Foundation (SNSF) | |||
| Death | OR (95% CI): 5.25 (0.31–87.14) | ; Prostate Cancer Foundation | |||||
| ; and Italian Association for Cancer Research | |||||||
| Investigator Grant | |||||||
| Caffo et al.4 2020 | Retrospective study | Treatment group | Patients with mCRPC who underwent ADT (1433) | NA | SARS-CoV-2 positivity | Number of case: 34 | None |
| Hospitalization | Number of case: 22 | ||||||
| Control group | NA | Admission of ICU | Number of case: 5 | ||||
| Death | Number of case: 13 | ||||||
Outcome
SARS-CoV-2 positivity
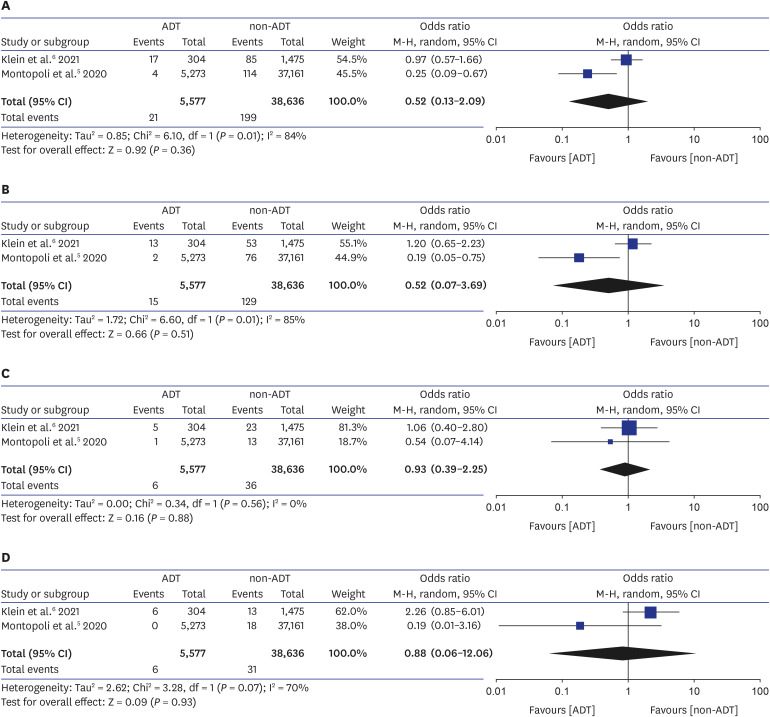
For the two included studies, there was no significant difference in SARS-CoV-2 positive rate between ADT and non-ADT groups (OR, 0.52; 95% CI, 0.13–2.09; P = 0.362, Fig. 2A). Heterogeneity among included studies was observed (P = 0.01; I2 = 84%).
Hospitalization
The two included studies showed no significant difference in hospitalization rate between ADT and non-ADT groups (OR, 0.52; 95% CI, 0.07–3.69; P = 0.514, Fig. 2B). Heterogeneity among included studies was observed (P = 0.01; I2 = 85%).
ICU admission
Two included studies showed no significant difference in ICU admission rate between ADT and non-ADT groups (OR, 0.93; 95% CI, 0.39–2.23; P = 0.881, Fig. 2C). Heterogeneity among included studies was not observed (P = 0.56; I2 = 0%).
Death
Two studies showed no significant difference in death rate between ADT and non-ADT groups (OR, 0.88; 95% CI, 0.06–12.06; P = 0.934, Fig. 2D). Heterogeneity among included studies was observed (P = 0.07; I2 = 70%).
Quality assessment, qualitative risk of bias, and certainty of evidence
The risk of bias graph and assessment results using the ROBINS-I tool are presented in Figs. 3 and 4. The study of Klein et al.6 had a relatively lower risk of bias than other studies. Results of assessment of the certainty of evidence using the GRADE approach are presented in Table 2. The certainty was low for SARS-CoV-2 positivity, hospitalization, and ICU admission. The certainty was very low for death. Funnel plots for publication bias demonstrated a certain degree of symmetry (Fig. 5).
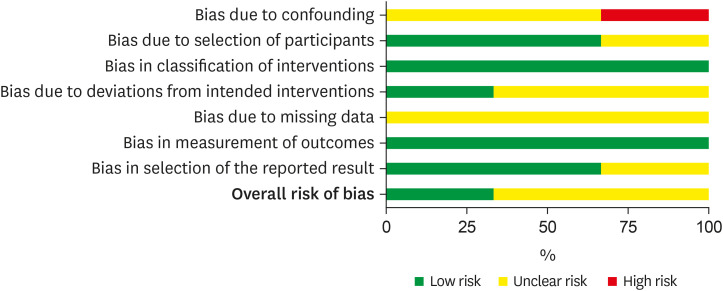
Fig. 4
Risk of bias assessment. Green plus: low risk of bias; Yellow question: unclear risk of bias; Red minus: high risk of bias.

Table 2
Grading of Recommendations, Assessments, Developments, and Evaluation (GRADE) quality assessment for direct evidence of each comparison
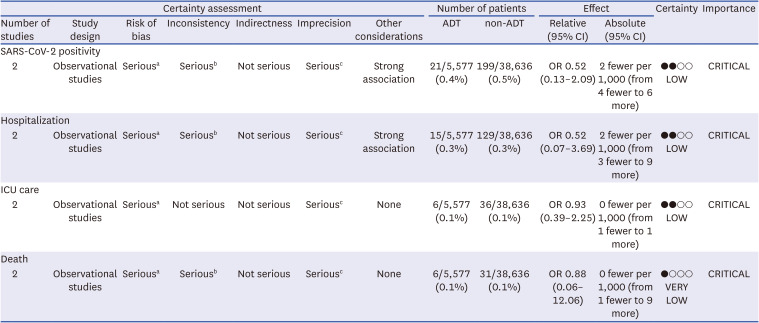
ADT = androgen deprivation therapy, CI = confidence interval, SARS-CoV-2 = severe acute respiratory syndrome-coronavirus-2, OR = odds ratio, ICU = intensive care unit.
aThere were some moderate and serious domains; bSignificant heterogeneity was observed; cUpper and lower limits of 95% CI included both meaningful benefit and harm.

DISCUSSION
To the best of our knowledge, this is the first systematic review about the relationship between ADT for prostate cancer and risk of SARS-CoV-2 infection. We found that there was no significant difference in SARS-CoV-2 positive rate, hospitalization, ICU admission, or death between ADT and non-ADT groups of patients with prostate cancer. Due to limited number of relevant cohort studies available, more evidence will be required to confirm the relationship between COVID-19 and ADT. However, we proposed fundamental methodological elements as shown in methodological qualities.
The importance of methodological quality includes the point that current studies could not reflect various aspects such as biochemical and immunological background. Covariate data such as comorbidities, such as asthma, coronary artery disease, diabetes, heart failure, hypertension and immune suppressive disease, use of steroids, and smoking status should be incorporated into cohort studies. To determine severity, outcome measures of admission to hospital, admission to ICU, and death were used. Montopoli et al.5 failed to report COVID-19 mortality rate. However, Caffo et al.4 found that the mortality rate in those under 70 years was 25%, which was higher than that (< 13%) expected for the whole population of infected Italian men with the same age. These findings suggest that ADT is unlikely to be a suitable intervention for patients with acute respiratory distress syndrome as it potentially could initiate or aggravate a cytokine storm.
No cohort studies included for the present study used matched controls. One failed to include key covariates. To determine the risk of bias in results, we used the ROBINS-I tool, which showed that the study of Klein et al.6 had a relatively lower risk of bias than other studies.45 ROBINS-I tool has been designed to compare health effects of two or more interventions in non-randomized studies.
Among various aspects that future COVID-19 severity research should focus on is the relationship and functional effect that androgen has on TMPRSS2, an androgen-regulated gene. Upregulated TMPRSS2 can facilitate tumor progression in prostate cancer.1112 Moreover, the expression of TMPRSS2 in tissues other than prostate (such as lung tissue) appears to be regulated by the same androgen receptor.11 Based on the activity and expression of TMPRSS2 downregulated by ADT, there is an implied positive correlation between expression levels of TMPRSS2 and androgen.12 Despite this, results of some studies have suggested that the role of TMPRSS2 in the severity of COVID-19 infection is probably minimal. The evidence supporting a role of overexpressed TMPRSS2 protein in SARS-CoV-2 lung pathology so far has only been from in vitro studies. There has been no patient data to support such hypothesis. In addition, expression levels of AR and TMPRSS2 proteins in lung tissues do not seem to be high, although high levels of TMPRSS2 mRNA isolated from human lung tissues have been reported.13
Secondly, research into the role of androgen in COVID-19 should also examine the relationship between oestrogen and COVID-19. It is well recognized that oestrogens exerts protective effects as demonstrated in pregnant women whose oestrogen levels, particularly E3 levels, are elevated.14 Murine SARS studies have verified the immunomodulatory capacity of oestrogen.15 This evidence, along with other immunomodulatory effects of oestrogen reported, lends weight to the hypothesis that oestrogen confers some protection against severe COVID-19 infection. Consequently, oestrogen therapy should be regarded as a potentially significant intervention. Thus, clinicians should fully consider its use for treating COVID-19. Indeed, there are ongoing studies evaluating a short-term use of oestrogen in COVID-19 patients to limit disease progression and patient deterioration.1617
Thirdly, it is important to explore the relationship between immunological factors and COVID-19 outcome in male patients who also have prostate cancer. In the presence of single-strand RNA viruses, like SAR-CoV-2, innate immune cells such as B cells, circulating monocytes, dendritic cells, and macrophages overexpress toll-like receptor 7 (TLR7).1819 In a study of SARS-CoV infected male and female mice, it was found that levels of proinflammatory cytokine (IL-6) and chemokines (CCL2 and CXCL-1) during the early phase of infection were comparable in both sexes with similar efficacy. However, by the third day, expression levels of these inflammatory cytokines and chemokines in male mice were significantly greater than those in females.20 This finding indicates that, when challenged with SARS-CoV-2, male mice would be more susceptible to the infection with an elevated recruitment of inflammatory cells. This phenomenon can account for the protracted inflammation instigated by SARS-CoV-2 infection, which is more commonly experienced by males than females. It may also contribute to the severity of COVID-19 in men.
Fourthly, by studying the protective effect of soluble ACE2 in prostate cancer patients, a deeper understanding may emerge about the relationship between androgen and severe COVID-19. Plasma concentration of renin is increased in response to the androgen hormone. Androgen can stimulate the transcription of angiotensinogen mRNA and the translation of angiotensinogen protein. Functionally active angiotensin is a vasoconstrictor. It has implications in severe COVID-19 as it is associated with complications. Therefore, androgen may nullify protective effects conferred by high levels of soluble ACE2. The corollary of the androgen-angiotensin relationship is that males are more vulnerable to severe infection.20
Finally, more studies are needed to explore interactions between new-generation androgen signalling inhibitors and testosterone. According to Caffo et al.,4 patients with mCRPC frequently receive taxane treatments and new-generation androgen-targeting therapies in addition to ADT. It is noteworthy that none of those studies reported here has addressed the effect of total testosterone (TT) on immune responses in males or the extent of that effect on infectious respiratory diseases. The activity of respiratory muscles, general strength, and exercise capacity can be adversely affected when testosterone levels are low.21 On the other hand, a number of respiratory outcomes are improved when circulating levels of testosterone are normal, indicating a protective effect.22 From observed effects of androgens, their roles in immune responses and, their changing levels throughout life,23 it is possible that hypogonadism could confer some protection against the onset of COVID-19 infection. However, it could also increase the risk of severe infection in patients with comorbidities who have high basal levels of pro-inflammatory cytokines. This scenario is borne out by evidence collected by Rastrelli et al.24 These researchers noted that baseline TT levels were lower in 31 male SARS-CoV-2 pneumonia patients who were followed-up in the respiratory ICU. These researchers concluded that low TT levels were predictive of poor prognosis and mortality in men with COVID-19.
COVID-19 can affect almost all organ systems of the body. This complex disease caused by infection with SARS-CoV-2 can stimulate secretion of pro-inflammatory cytokines, which in turn stimulates chronic systemic inflammation and persistent activation of the innate immune system. Autopsies of COVID-19 patients have commonly revealed heightened immune response that leads to organ failure. The risk of severe infection is greater in individuals with pre-existing comorbidities. This study reviewed previous studies qualitatively and quantitatively and found that there was no significant effect of ADT on COVID-19. However, more higher quality studies that explore biochemical and immunological factors involved are needed to confirm this finding in the future.
 XML Download
XML Download