

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
METHODS
Data sources
Study population
Inclusion criteria
1) Patients aged ≥ 18 years
2) Patients who had at least one diagnosis code of pneumonia (J10.x–J18.x and J20.x as primary or diagnosis within 2nd position) from the International Classification of Disease, Tenth Revision (ICD-10)
3) Patients who were treated using intravenous (IV) antibiotics for more than 3 days
4) Hospitals which claimed at least five cases of hospitalized CAP
Exclusion criteria
1) Patients who had the following conditions not meeting the criteria of CAP: a) hospital acquired pneumonia, b) ventilator-associated pneumonia, c) postoperative pneumonia, d) patients who had transferred from other health care facilities, and e) patients who were admitted to the hospital for more than 2 days in the recent 90 days
2) Patients who were not treated with IV antibiotics first at the hospitals, such as those who were transferred from other hospital with previous antibiotics use or who were not administered antibiotics within 72 hours of admission
3) Patients who were delayed appropriate treatment owing to inevitable causes such as emergent operation
4) Patients who had the following conditions: a) patients who were recently diagnosed with malignant cancer (≤ 3 months), b) patients who received chemo- or radiation therapy within 3 months, c) patients who take immunosuppressant agents, d) patients who were treated with high dose steroids with a composition greater than 20 mg/day (≥ 14 days), e) patients who regularly underwent dialysis, and f) patients who have human immunodeficiency virus or acquired immune deficiency syndrome
5) Hospitals which claimed less than 5 cases of hospitalized CAP
6) Patients who are in or transferred from nursing hospitals
Definition of class of hospitals in South Korea
Core Assessment of CAP score measurement
Comorbidities
Statistical analyses
RESULTS
Hospitalized CAP demographics
Fig. 1
Schematic diagram of the study. Both QA database and medical claims database were manipulated by the HIRA of South Korea. All the data were matched by anonymous join keys. From 1st to 3rd QA rounds, 54,307 hospitalized CAP cases were collected, after excluding the non-CAP cases.
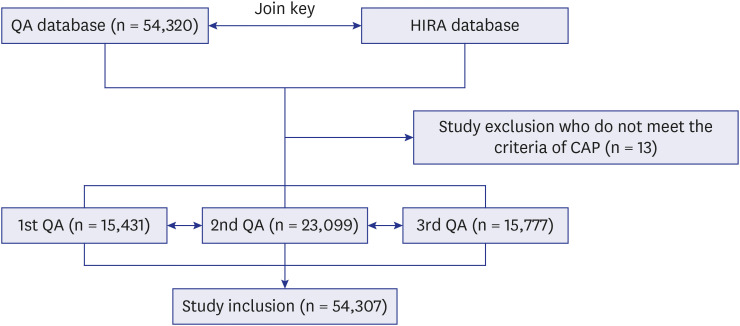
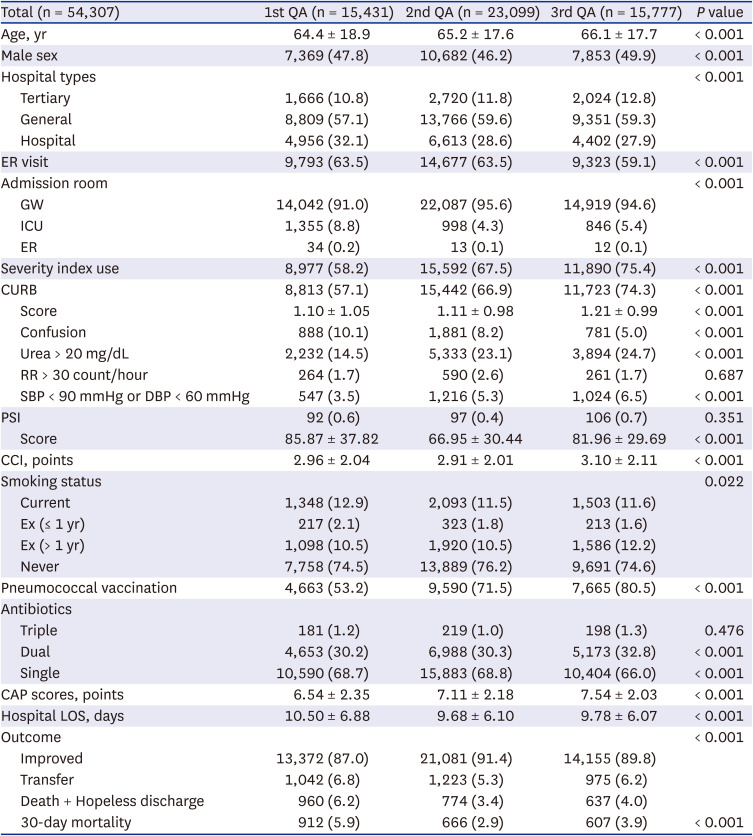
Table 1
Demographics of hospitalized CAP in Korea
CAP changes by proceeding of QA program
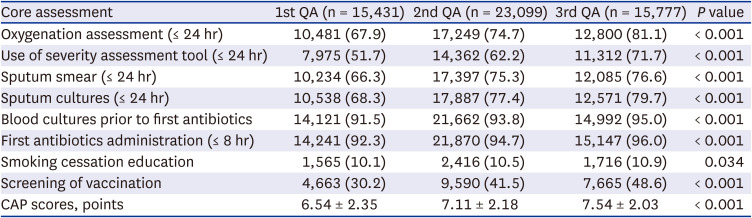
Table 2
Core measures of QA of hospitalized CAP in South Korea
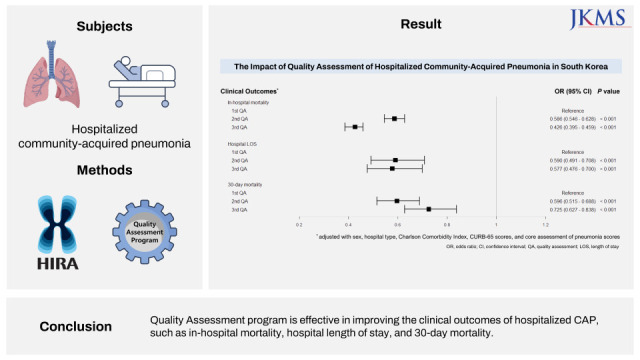
Change of in-hospital mortality
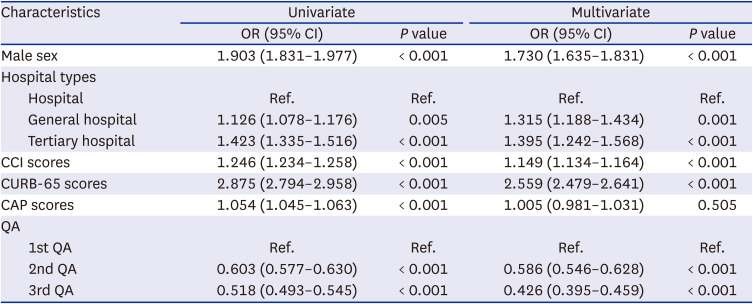
Table 3
Univariate and multivariate logistic analyses of in-hospital mortality of hospitalized CAP in Korea
Change in hospital stays
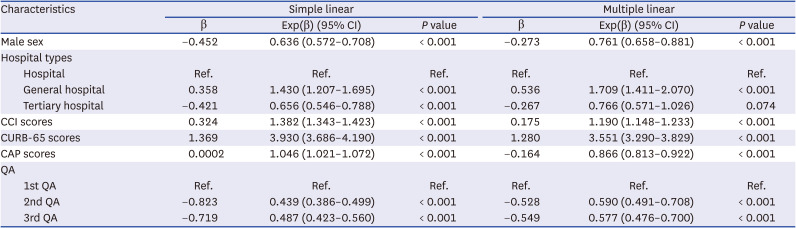
Table 4
Simple and multiple linear regression analyses for the hospital length of stay in hospitalized CAP in Korea
The 30-day mortality improvement
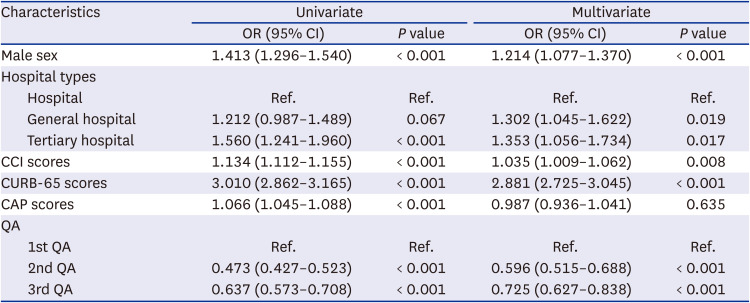
Table 5
Univariate and multivariate logistic analyses of 30-day mortality of hospitalized CAP in Korea
 XML Download
XML Download