

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The management of rectal cancer has advanced with multimodal approaches in recent decades. With the introduction of total mesorectal excision (TME) by Heald et al. [1] and preoperative chemoradiotherapy (PCRT), local control has been greatly improved [2345]. Undoubtedly, radical resection based on the TME principle is the most important standard in treatment of rectal cancer in terms of curative resection, staging, prognosis, and subsequent therapeutic decisions. The core of the TME technique is a sharp dissection based on pelvic anatomy that subsequently results in en bloc removal of rectal tumor and surrounding mesorectum containing lymph nodes with pelvic nerve preservation [5]. The accuracy of TME has become an indicator for the quality of oncologic surgery. It can predict the likelihood of local recurrence [67]. However, a TME procedure for lower rectal cancer is challenging because many important structures are crowded in the narrow pelvis, making it difficult to reach the target anatomy and surgical plane, especially for patients with bulky tumors. The major difficulty for a low rectal cancer surgery is the poor visualization of the deep pelvis. Due to such difficulties, there have been demands for securing visibility and instruments suitable for working in a limited space. This need has led to advances in surgical technologies with an interest in minimally invasive surgery. High-resolution images by laparoscopy and robotic surgery provide a better view, allowing more anatomical dissection and function preserving techniques [8].
Laparoscopic surgery (LS) in colorectal cancer has progressively replaced open surgery in recent decades due to its advantage of less pain, reduced blood loss, faster recovery time, and better cosmesis [9]. Several landmark trials comparing open surgery and LS for rectal cancer have reported no difference in survival outcomes when they are performed by well-qualified surgeons [101112]. However, laparoscopic rectal surgery is a technically demanding procedure that requires intensive training. It also has visual/instrumental limitations in selected cases. Early clinical studies have shown a high open conversion rate and a high proportion of circumferential resection margin (CRM) positive rate for laparoscopic rectal surgery with concerns about its oncologic safety [1314]. These results might be attributed to the initial learning curve and inherent limitations of LS, such as an unstable assistant-controlled camera, poor ergonomics, straight instruments, fulcrum, and tremor effect.
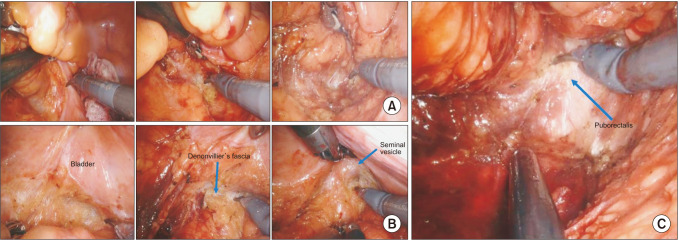
A robotic surgery (RS) system has been envisioned to be able to overcome limitations of laparoscopy. The da Vinci robotic system (Intuitive Surgical Inc., Sunnyvale, CA, USA) is a prevailing robotic platform that can provide enhanced operator-controlled 3 dimensional (3D) high-definition vision and an endo-wrist technology allowing 7° of freedom intraabdominally with tremor elimination and improved dexterity [15] (Fig. 1). These features of RS might be more suitable for rectal cancer surgery in a narrow pelvic cavity with confined field of view. The oncological safety and functional safety of RS are expected to be potentially improved by improving the TME quality. However, RS has disadvantages such as the lack of a haptic sense and longer operation time with additional time consumed for docking procedure [16]. The main issue of RS is its higher cost compared to conventional LS [1718]. Although global utilization of RS is increasing, the cost-effectiveness in terms of oncological and functional safety of RS for low rectal cancer has not been evaluated sufficiently. Therefore, the objective of this review is to provide recent updates on the current evidence regarding oncologic and functional outcomes of RS for low rectal cancers. Its real benefits are also discussed.

Go to : 
METHODS
Identification
PubMed, Embase, and Cochrane Library databases were searched. PubMed was searched using keywords and mesh terms of rectal neoplasms, colorectal surgery, robot surgery, and robot-assisted surgery in combination with Boolean operators AND or OR. The same strategy was adopted for searching other databases. Restriction was applied to include only human studies published up to March 25, 2022. After the initial electronic search, articles were further hand-searched. Articles identified were assessed individually for inclusion. Titles and abstracts of studies were then screened to exclude those not pertinent to the study subject.
Study selection
A full-text assessment was performed. Relevant reports that compared robotic techniques to laparoscopic or open technique for rectal cancer surgery were retrieved. Studies were excluded if: (1) the study design was editorial, commentaries, technical notes, or letters to the editor; (2) the type of publication was a conference proceeding or abstract; and (3) full text was written in a language other than English. In the case of duplicate publication, the latest study with the most adequate design and extended patient series was considered for the review.
Go to :
INTRAOPERATIVE AND PERIOPERATIVE OUTCOMES
Many previous studies have demonstrated that RS for rectal cancer is a safe and feasible surgical approach in terms of intraoperative complication, conversion rate, and short-term surgical outcomes [19202122232425]. Intraoperative and perioperative outcomes after rectal cancer surgery are presented in Table 1. Crippa et al. [25] have reported that RS shows better short-term outcome with a significantly lower conversion rate (5.1% vs. 13.8%, P < 0.001), shorter length of hospital stays (3 days [range, 3–5 days] vs. 5 days [range, 4–7 days], P < 0.001) and lower overall morbidity rate (37.2% vs. 51.2%, P < 0.001) than LS in a relatively large cohort. A meta-analysis of randomized controlled trials has found that the conversion rate of RS is significantly lower than that of LS [26]. Although the ROLARR (RObotic Versus LAparoscopic Resection for Rectal Cancer) trial failed to show statistical significance in overall conversion rate comparing RS and LS, it revealed difference in RS conversion rate between men and women, with RS appearing to offer more benefit for men than for women in a subgroup analysis (odds ratio, 0.46; 95% confidence interval, 0.21–0.99; P = 0.043) [27]. Considering that conversion to open surgery is associated with unfavorable short-term outcomes, lowering the conversion rate has clinical benefit [2829]. The low conversion rate to open surgery of RS, especially in male patients, suggests the potential benefit from RS of facilitating dissections in a narrower space with more operator-controlled retraction and better optics for technically challenging patients.
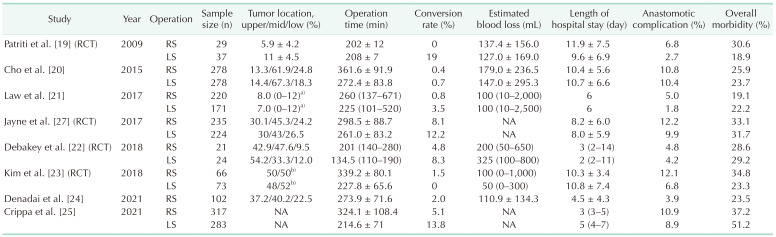
Most studies comparing RS and LS for rectal cancer have consistently reported significantly longer operation time for RS [202122232526]. The longer operation time of RS is due to docking and placement of the instrument with manipulation via camera and instrument sequentially by the operator alone; whereas the camera and the instrument can be moved simultaneously with a camera assistant and first assistant in LS. Although the operation time can be shortened with experience, the longer operation time of RS compared to LS might be a drawback of RS for a subgroup of patients.
For other intraoperative and perioperative outcomes such as estimated blood loss, length of hospital stays, and postoperative morbidity including anastomotic leakage, the results of RS were comparable to those of LS without showing notable advantages, although RS was suggested to have difficulty in bleeding control [22232427].
Go to :
PATHOLOGIC AND LONG-TERM ONCOLOGIC OUTCOMES
TME completeness and CRM involvement are recognized as parameters that can indicate the quality of surgery for rectal cancer and predict local recurrence and poor disease-free survival (DFS) [6]. Compared to conventional approaches (open surgery, LS), RS is expected to contribute to better TME quality and survival outcomes as it has a technical advantage in that it enables surgery with an accurate surgical plane (Fig. 2). However, RS did not show better results than LS in TME completeness or CRM positivity rate for cases involving experienced surgeons [23262730]. In addition, studies published to date have not demonstrated improvement in oncologic outcomes after RS for low rectal cancer patients compared to conventional approaches (open, LS) [18203132].
There was no significant difference in terms of local control between RS and LS. Compared to LS with a 5-year local recurrence rate of 2%–6%, groups that included patients who received PCRT showed similar local recurrence rates [1833]. However, in more challenging situations, RS has the potential to be more advantageous than LS. Yamaoka et al. [34] have reported a favorable local recurrence rate of 4% in patients with 122 clinical T4 stage cases after RS, despite 28% of them having undergone a combined resection of adjacent organs.
Currently, evidence from a prospective randomized trial comparing RS and other surgical approaches regarding long-term oncologic outcomes is not available. Several retrospective studies have compared survival outcomes of RS and LS and found that DFS and overall survival (OS) after RS are similar to those of LS [1820213233]. In a case-matched study, Kim et al. [33] showed that patients who underwent RS had higher 5-year OS (RS, 90.5% vs. LS, 78.0%), cancer-specific survival (RS, 90.5% vs. LS, 79.5%), and DFS (RS, 72.6% vs. LS, 68.0%) than those who underwent LS. However, differences between the 2 groups were not statistically significant. Park et al. [35] have reported no significant difference in 5-year DFS between RS and LS in matched patients with mid to low-lying rectal cancer. However, in a subgroup analysis of patients with ypT3/4 tumors who received PCRT, they found that the RS group had lower 5-year distant recurrence (RS, 9.8% vs. LS, 44.8%; P = 0.014) and higher 5-year DFS (RS, 81.3% vs. LS, 55.2%; P = 0.076), although the difference in 5-year DFS was not statistically significant. Based on these results described above, RS did not show better long-term oncologic outcomes than LS. The role of RS in advanced disease needs further evaluation. Long-term oncologic data of 2 currently ongoing randomized controlled trials [2327] have not been reported yet. Long-term oncologic outcomes after RS for rectal cancer patients are summarized in Table 2.
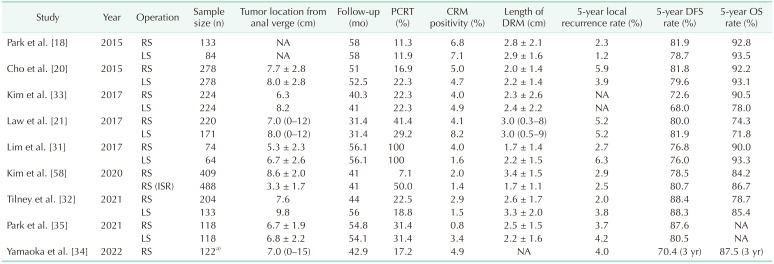
Table 2
Oncological outcomes after laparoscopic and robotic surgery for rectal cancer patients
PCRT, preoperative chemoradiotherapy; CRM, circumferential resection margin; DRM, distal resection margin; DFS, disease-free survival; OS, overall survival; RS, robotic surgery; LS, laparoscopic surgery; NA, not applicable; ISR, intersphincteric resection.
a)Only patients with cT4 stage based on pretreatment MRI were included.
![]()
Go to :
FUNCTIONAL OUTCOMES
In rectal cancer surgery, quality of life regarding urinary and sexual function is another major concern. Urogenital dysfunction is a well-known common complication after rectal cancer surgery, especially in men. It is caused by direct or indirect injury to the pelvic autonomic nerve during pelvic dissection. RS with a 3D magnified view and an endo-wrist has the advantage of easier nerve identification, thus reducing nerve damage. It might have the potential to improve urinary and sexual function outcomes.
Results of comparing functional outcomes after RS and LS for rectal cancer are summarized in Table 3. In previous studies evaluating functional outcomes after rectal cancer surgery, International Prostate Symptom Score (IPSS), a subjective scoring system measuring voiding function in 7 categories, has been mainly used to evaluate urinary function [36]. Several studies have reported that patients who have undergone RS have a significantly lower IPSS score or greater improvement of IPSS score postoperatively than those who have undergone LS [37383940]; whereas there is no significant difference in urinary function between RS and LS for female patients [3841].
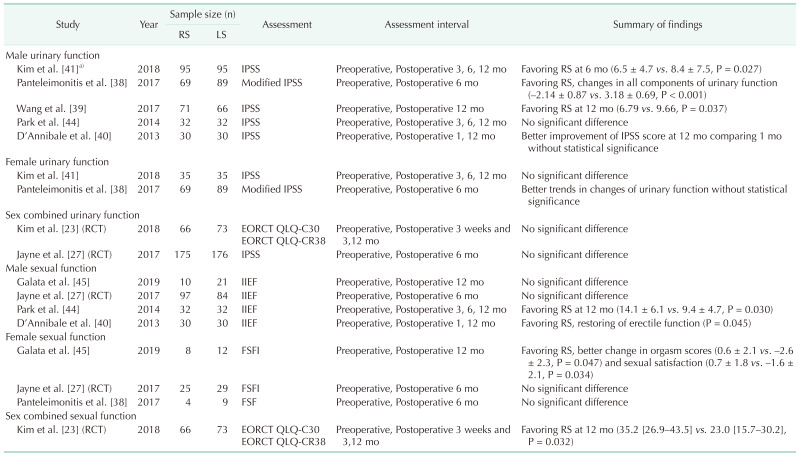
Table 3
Urinary and sexual functional outcomes after LS and RS for rectal cancer patients
RS, robotic surgery; LS, laparoscopic surgery; IPSS, International Prostate Symptom Score; RCT, randomized controlled trial; EORTC QLQ, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; FSFI, Female Sexual Function Index; IIEF, International Index of Erectile Function.
a)Case-matched study.
![]()
The 5-item version of the International Index of Erectile Function (IIEF) is used most commonly to evaluate male sexual function, with a lower score representing poorer sexual function [42]. In the case of women, the Female Sexual Function Index consisting of 19-item self-report measures such as sexual desire, libido, and confidence [43] is most commonly used. Reported results regarding sexual function are inconsistent. Park et al. [44] have reported that IIEF score is better for male patients who have undergone RS than for those who have undergone LS. D’Annibale et al. [40] have shown that erectile function in the RS group is restored completely at postoperative month 12. Other studies have reported no difference in IIEF between RS and LS [2745]. Regarding female sexual function, Galata et al. [45] have reported that the female patients who have undergone RS show better changes in orgasm score and sexual satisfaction. However, another study has reported that there is no significant difference in female sexual function between RS and LS groups [38].
The ROLARR trial, a randomized controlled study that compares RS and LS for rectal cancer, has shown no difference in urinary function or sexual function between RS and LS groups [27]. In another randomized controlled trial comparing outcomes of RS with LS, functional outcome was evaluated using the European Organization for Research and Treatment of Cancer Quality of Life (EORTC QLQ) C30 and EORTC QLQ CR-38 [23]. There was no difference in urinary function in gender combined analysis. However, sexual function was better in the RS group than in the LS group at 12 months after surgery [23]. Sex differences in pelvic anatomy exist between male and female patients, which can greatly increase the difficulty of rectal surgery in men. Such anatomical variations may explain differences in functional outcomes according to surgical approach in men, but not in women. However, results on the number and quality of functional outcomes after rectal cancer surgery are limited. In addition, evaluation tools for functional outcomes are not standardized. Thus, there are limitations when interpreting results. Even if there is a statistical difference in the score, it is difficult to correlate statistical findings to a consistent clinical outcome. The difference in score may result in a change in category from severe to moderate or mild dysfunction, or it might have no effect on the category. The quality of life and functional data in rectal cancer surgery have such a significant weakness. Therefore, current evidences in terms of urinary and sexual function after RS are not conclusive, although some studies have reported better urinary and erectile function in male patients who have undergone RS [46].
Go to :
EXTENDED TECHNIQUES IN ROBOTIC SURGERY
Lateral pelvic lymph node dissection
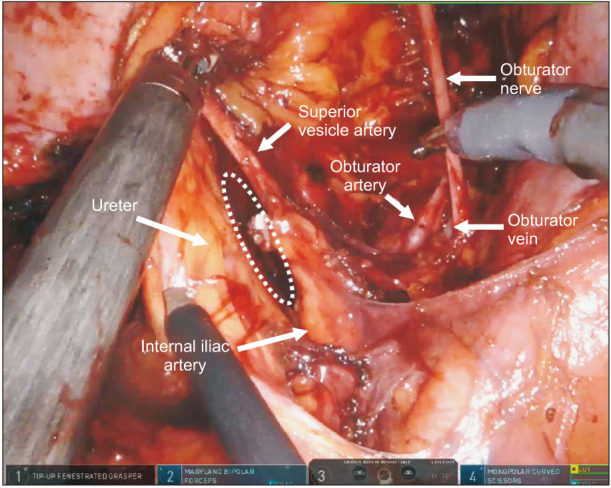
Although the prognostic significance of lateral pelvic lymph node dissection (LPLND) is still controversial, recent data suggest that clinically positive lateral pelvic lymph nodes (LPLNs) might have a high risk of treatment failure irrespective of PCRT or LPLND [474849]. LPLND is a technically demanding procedure owing to its technical difficulty, risk of incomplete dissection, and higher incidence of intraoperative bleeding and surgical morbidity including urinary and sexual dysfunction [48]. However, technical advantages of RS may facilitate more precise dissection of lymph nodes from the complicated neurovascular anatomy with the lateral wall of the pelvis (Fig. 3). Especially, RS is easily accessible from both sides when performing bilateral LPLND. Therefore, the difficulty of both approaches is similar, while LS is relatively easy on one side and inaccessible on the other side depending on the operator’s position. Some studies have shown that the robotic approach of performing LPLND is safe and feasible with acceptable postoperative morbidity [505152]. In addition, indocyanine green could be used to guide the detection of LPLNs to improve accuracy and completeness of LPLND by visualization with a near-infrared camera system in robotic platforms [5354].
Intersphincteric resection
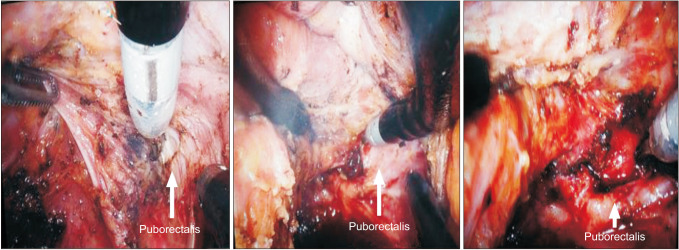
With a better understanding of pelvic anatomy and advances in surgical technologies, sphincter-saving resection for low-lying rectal cancer patients has largely replaced abdominoperineal resection (APR). Intersphincteric resection (ISR) is a safe procedure that ultimately preserves the anus without permanent stoma. It has acceptable oncological and functional outcomes [5556]. ISR requires deep and complex pelvic dissection. The application of the robotic approach for ISR might be technically more efficient than open surgery or LS. RS could provide stable visualization of the pelvic floor muscle complex with proper stable traction and angulation of instrument targeting the surgical plane, thus allowing precise dissection (Fig. 4). Several studies have described technical issues of robotic ISR and shown acceptable perioperative, oncological, and functional outcomes of robotic ISR for low-lying rectal cancer patients [5758]. However, there is a risk of worse anorectal functional outcomes, which can threaten the quality of life in some patients including those with very-low rectal cancer and those who have received radiotherapy. Thus, it is important to select the appropriate patients to achieve an optimal functional outcome [8].
Partial excision of levator ani muscle
Partial excision of the levator ani muscle is a recently proposed new surgical alternative to APR for very-low rectal cancer invading the ipsilateral levator ani muscle [8]. This procedure can be maximized when combined with RS, which enables more precise surgery [59]. However, this technique needs validation for its oncological and functional safety.
Go to :
LEARNING CURVE
Superior ergonomics and instrumentation of RS might have a positive effect on the learning curve to acquire adequate surgical competence. Although many surgeons have already experienced LS and quickly adapted to RS, previous analyses support a short learning curve for RS [606162]. According to previous reports, the learning curve of RS for rectal cancer surgery requires 25–65 cases [6061626364]. For the conventional laparoscopic approach, approximately 40–90 cases are required for the learning curve [656667]. Several studies showed a short learning curve for a novice surgeon comparable to those who had already mastered the technique with laparoscopic or open approach [6268]. The faster acquisition of surgical techniques in robotic platforms may contribute to the adoption of new technologies in rectal cancer surgery. Future surgeons can also be trained to perform robotic rectal cancer surgery with fewer difficulties. This could allow more patients access to the benefits of RS.
Go to :
CONCLUSION
RS for low rectal cancer patients has several technical advantages for surgeons. However, for patients, the evidence so far does not show any superiority of RS over LS regarding perioperative, oncological, and functional outcomes. Operative time and the high cost of RS remain as challenges. Further studies are needed to prove the potential benefit of RS over LS in technically challenging patients such as men with very narrow pelvic anatomy, obese patients, and those with bulky or fixed tumors. The application of robotic systems to technically demanding procedures and novel surgical strategies will contribute to favorable outcomes of rectal cancer surgery in the future. Since the surgical principle for treating rectal cancer is well established, comparable oncological and functional outcomes should be obtained regardless of the surgical approach as long as the surgical principle is observed. Advanced technology using RS should be developed in a way that allows established surgical principles to be adhered to, even when operating on patients with anatomical and pathological obstacles. Outcomes of rectal cancer surgery are expected to be leveled upward using the advantages of RS.
Go to :
 XML Download
XML Download