

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients with a good response to concurrent chemoradiotherapy (CCRT) may have good oncological outcomes [123]. This can potentially allow for long-term conservative approaches, such as local excision or watchful waiting, which avoid the risks of surgical complications, including the need for a stoma [4]. In treating patients with low rectal cancer, preserving the anal sphincter and improving the quality of life via neoadjuvant CCRT are critical goals. However, the current standard treatment for locally advanced rectal cancer is neoadjuvant CCRT, followed by total mesorectal excision [5].
Several researchers have investigated the association between clinical parameters and pathological tumor response in patients with locally advanced rectal cancer. Tumor size [67], movability [6], and circumferential extent [8] as well as T stage, N stage, and histological grade [9] have been found to be predictive factors of responses to preoperative CCRT in these patients. Other studies have also found that a low CEA level, high hemoglobin level, and low neutrophil-to-lymphocyte ratio are predictors of good tumor response to CCRT [10111213].
The European Society for Medical Oncology and National Comprehensive Cancer Network guidelines, which were based on multidisciplinary expert opinions, suggested that fragile patients who are at high risk of adverse events following surgery may instead suffice with the watch and wait method if clinical complete response is achieved as determined by digital rectal examination (DRE), rectoscopic biopsy, and/or MRI [1415]. There have been numerous efforts to identify predictive factors for good responses to CCRT; however, the use of these variables, which involve maintaining certain blood cell counts or serum marker levels during treatment, has been difficult to apply clinically [1617181920]. Therefore, there remains a need to identify factors that can be easily evaluated in clinical practice. In particular, predictors of achieving ypT0–1 stage, which is suitable for local excision or “watch and wait,” would help in supporting the current clinical trend of preserving the sphincter and avoiding over-treatment in rectal cancer.
This study aimed to identify and clinically assess factors that are predictive of achieving stage ypT0–1N0 after neoadjuvant CCRT in patients with middle or low rectal cancer, while focusing on information that clinicians are most familiar with, especially MRIs.
METHODS
The study protocol was approved by the Institutional Review Board of Seoul National University Bundang Hospital (No. B-2108/702-103). Owing to the study’s retrospective nature, the requirement for informed consent was waived.
Study population
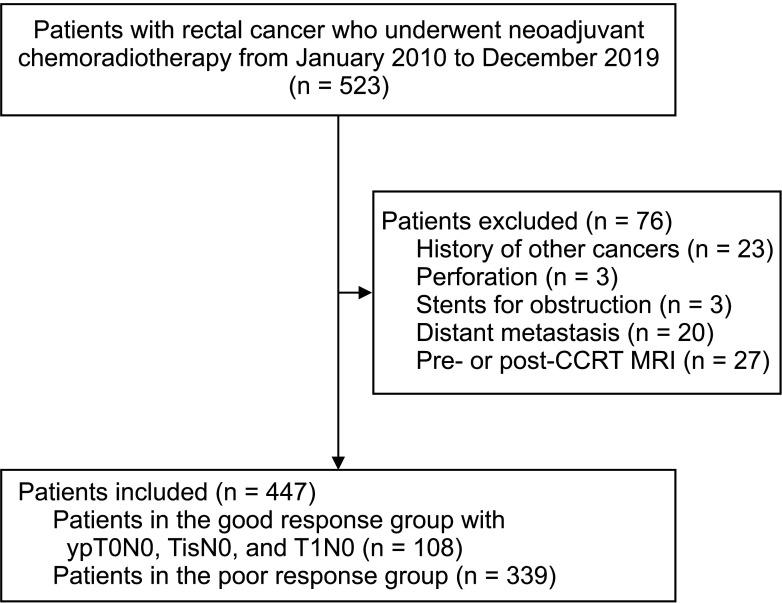
Between January 2010 and December 2019, 523 patients with mid to low rectal cancer, characterized by an inferior margin located at a distance below 10 cm from the anal verge, underwent surgery followed by neoadjuvant CCRT at a single center [1421]. Among these patients, we excluded 23 with a history of another cancer to avoid potential interference [2223], 3 with perforation, 3 with stents inserted for obstruction, 20 with distant metastases, and 27 lacking MRIs pre- or post-CCRT. Patients who underwent curative-intent surgery 6–8 weeks following completion of neoadjuvant CCRT at our hospital were included. Ultimately, a total of 447 patients with pathologically confirmed middle or low rectal cancer who received neoadjuvant CCRT were identified and retrospectively analyzed (Fig. 1).
Patients with stage ypTisN0 or T1N0 as well as those who achieved a pathological complete response (pCR) after neoadjuvant CCRT and surgical resection (108 patients) were classified under the good response group, whereas the remaining patients (339 patients) were included in the poor response group (Fig. 1).
Data collection
All data were retrospectively analyzed using a prospectively collected database that contained patient demographics, including age, sex, height, weight, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status (PS) classification, past medical history (including endoscopic procedures), CEA level, endoscopic information (anal verge height and gross type of tumor), pathological findings, and radiological findings. The normal range of CEA was defined as ≤5 ng/mL.
All surgical procedures were performed by surgeons who were well-experienced in both open and laparoscopic total mesorectal excision for low rectal cancer. The decision to administer neoadjuvant treatment was based on the tumor stage. Patients with T3, T4, or positive nodes without distant metastases received neoadjuvant CCRT [23]. Those with T2 low rectal cancer for whom sphincter preservation was planned also received neoadjuvant CCRT [2425].
Patients were injected with antispasmodics (hyoscine butylbromide) intravenously prior to MRI. Each patient was placed in the recumbent position, and 2 syringes, each filled with 50 mL of ultrasonic jelly, were injected into the anus using a catheter, while removing air as much as possible. Next, the patient was placed in the supine position, and the image was acquired using a Philips INGENIA 3.0T (Philips Medical System, Eindhoven, Netherlands). Dedicated abdominal radiologists interpreted the pre- and post-CCRT MRIs and graded the distance between the tumor and mesorectal fascia (MRF), tumor height from the anorectal junction, tumor size, clinical TNM stage, and tumor direction. A threatened MRF was defined as the presence of a tumor within 1 mm from the MRF [5]. If a DRE result was available in the medical record, the morphology was determined by supplementing it with the endoscopic result.
All resected specimens were examined by experienced gastrointestinal pathologists. Pathological TNM stage, resection margins (such as circumferential, distal, and proximal), gross type, and lymphovascular invasion were assessed.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation, whereas categorical variables are expressed as numbers (percentages). Univariable analyses using the Student t-test or the chi-square test were performed to identify the clinical variables associated with favorable tumor response to CCRT. Multivariable analysis was performed for variables that could be examined at bedside by the clinicians before the treatment and that showed significant differences in the Student t-test and chi-square test. A correlation matrix (Spearman rho) was constructed to evaluate concordance. Multivariable analysis was then performed using a logistic regression model. Two-tailed P-values of <0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics ver. 26 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
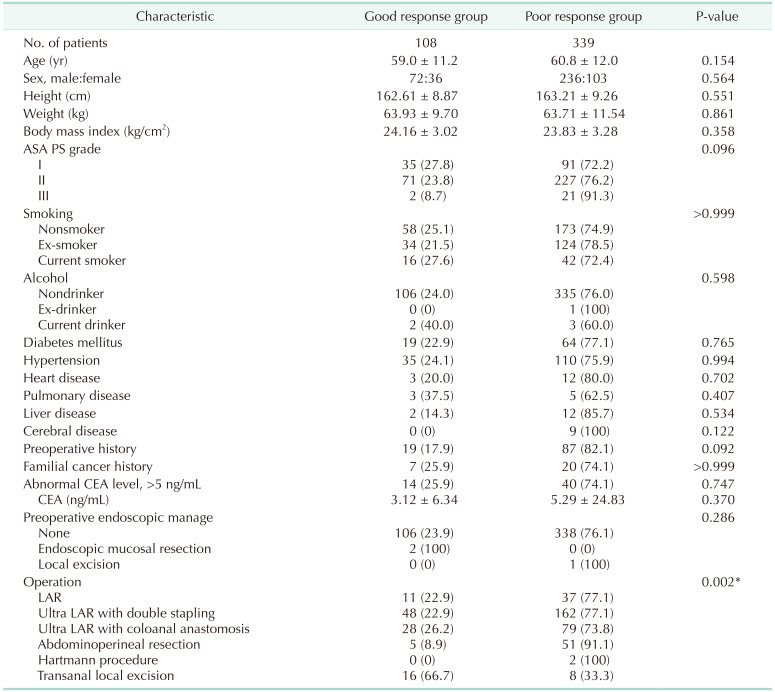
Of the 447 patients (mean age, 60.37 ± 11.85 years), 108 (24.2%) achieved ypT0-1N0 post-CCRT: 77 (71.3%) with ypT0N0, 5 (4.6%) with ypTisN0, and 26 (24.1%) with ypT1N0. The patients’ baseline characteristics are shown in Table 1. There were no significant differences in age, sex, height, weight, BMI, initial CEA level, and past medical history (including ASA PS grade, preoperative history, familial cancer history, or endoscopic procedures before treatment) between the good and poor response groups. However, transanal local excision was significantly more frequent in the good response group (66.7% vs. 33.3%, P = 0.002) (Table 1).
Predictive factors of response to neoadjuvant concurrent chemoradiotherapy
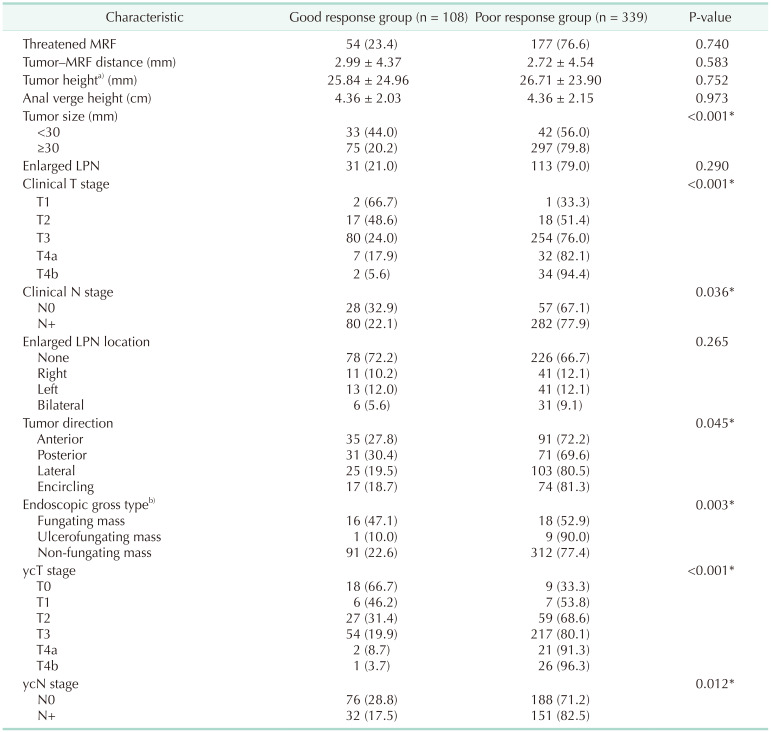
There were 3 patients with cT1 who received preoperative chemoradiotherapy; the clinical nodal status of all the patients before treatment was positive. Regarding cT2 disease, 16 patients with cT2N0 (8 in the good response group, 8 in the poor response group) and 19 patients with cT2N+ (9 in the good response group, 10 in the poor response group) were identified. In terms of radiological and endoscopic findings, the tumor distance to the MRF and the tumor height above the anorectal ring were not significantly associated with stage ypT0–1N0. Consequently, the proportions of patients with threatened MRF were not significantly different between the good and poor response groups. The factors associated with a good response to neoadjuvant CCRT included tumor size of <30 mm, lower clinical T and N stages before neoadjuvant CCRT, fungating tumor morphology on endoscopy, small primary tumor diameter on pretreatment MRI images, anterior/posterior directionality of the circumference, and lower ycT and ycN stages (Table 2).
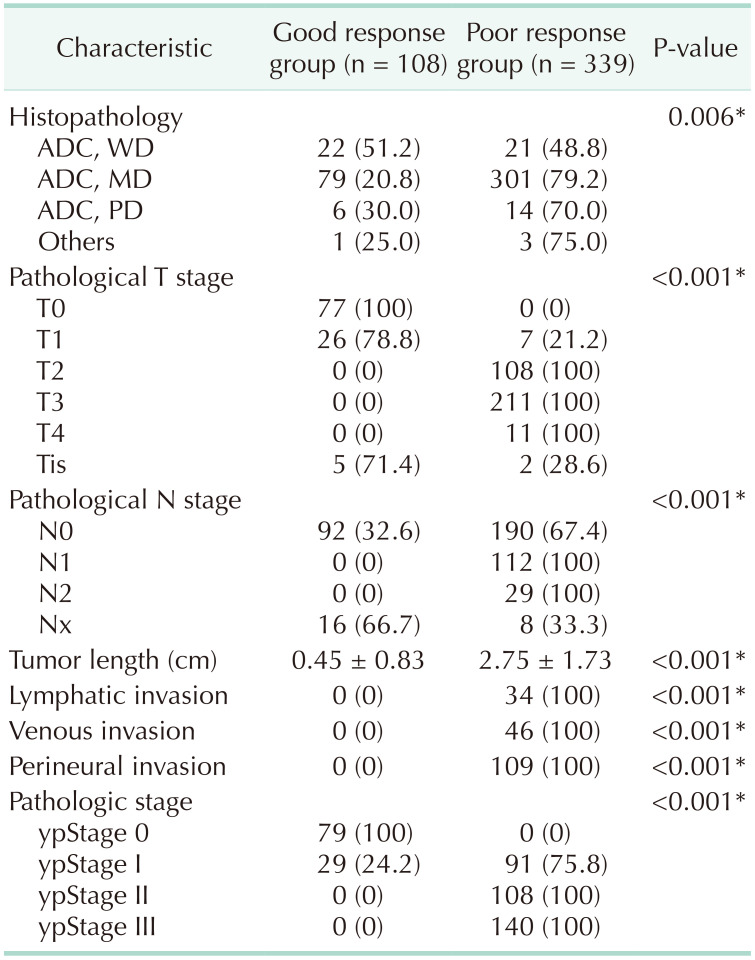
Pathologically, well-differentiated tumors were also significantly associated with stage ypT0–1N0 (51.2% [22 of 43] vs. 21.3% [85 of 400] in moderately or poorly differentiated tumors, P < 0.001) (Table 3).
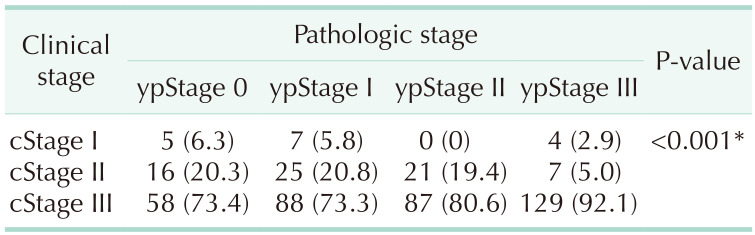
Table 4 describes the distribution of clinical stages before neoadjuvant CCRT and postoperative pathologic stages.
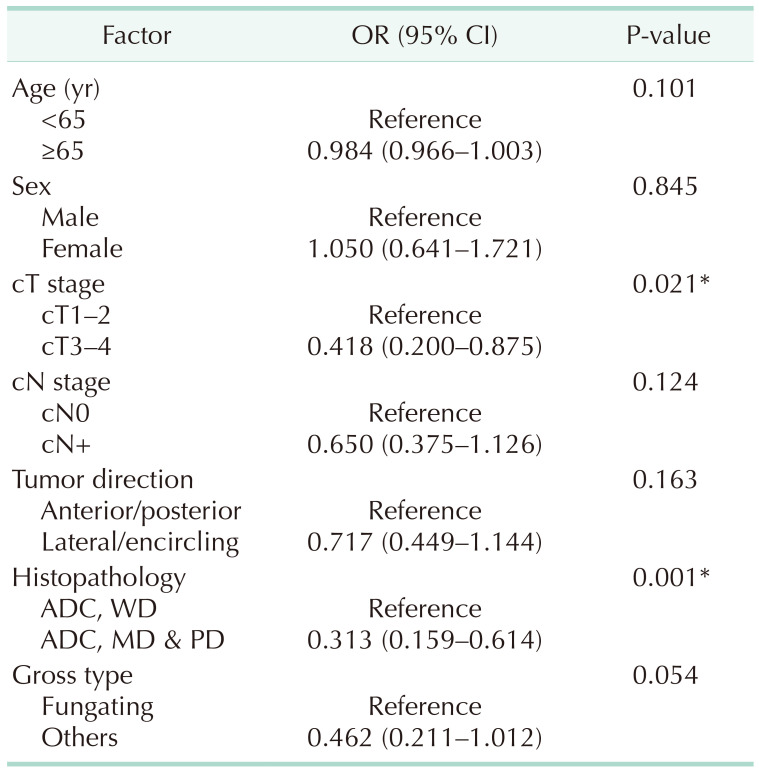
Table 5 presents the results of the multivariable logistic regression analyses. Clinical T1–2 stage (odds ratio [OR], 0.418; 95% confidence interval [CI], 0.200–0.875; P = 0.021) and well-differentiated tumors (OR, 0.313; 95% CI, 0.159–0.614; P = 0.001) were identified as independent factors associated with good response. A grossly fungating mass (OR, 0.462; 95% CI, 0.211–1.012; P = 0.054) was not significantly associated with good response on multivariable analysis.
The combined predictive value of clinical T stage (cT1–2) and tumor grade (well-differentiated type) was 50%. Thus, the combined use of these 2 factors provides information regarding tumor response to neoadjuvant CCRT in patients with rectal cancer.
DISCUSSION
In this study, we have identified stage cT1–2 and well differentiation of tumors as independent predictors of achieving stage ypT0–1N0 after CCRT. This finding could allow for the nonradical management of patients with middle or low rectal cancer, thus avoiding over-treatment after neoadjuvant CCRT. A fungating tumor type was just above the cutoff for significance on multivariate analysis.
To the best of our knowledge, no previous studies have been performed to predict tumor response based on achieving the ypT0–1N0 stage, which affords eligibility for transanal local excision [5]. Most previous studies have only focused on achieving a complete response [678910111213]. The ability to predict stage ypT1 and pCR is important in increasing the proportion of candidates who are eligible for minimally invasive and organ-preserving surgery through local excision, which was the ultimate objective of our study.
We found that cT classification before and after CCRT, ycN classification, and tumor size on pretreatment MRI were associated with good tumor response to neoadjuvant CCRT. Moreover, cT classification was an independent predictor of stage ypT0–1N0 on multivariable analysis. A retrospective study of 23,747 patients demonstrated that cT and N classifications were correlated with pathological response after neoadjuvant CCRT [9]. Smaller tumor size has also been reported as predictor of pCR in other retrospective studies [726]. In our study, tumor size and clinical T stage before CCRT showed the highest degree of correlation with good outcomes. Given that tumor size and tumor stage appear to influence each other, we selected only 7 factors other than tumor size as covariates in our multivariable logistic regression model. In general, our results are consistent with those of previous studies. Data regarding tumor movability was scarce owing to the retrospective nature of our study, although tumor movability may be a surrogate for T stage [6].
The relationship between histological grade and tumor response has been evaluated in several retrospective studies involving large cohort sizes (over 20,000 participants). These studies have reported that a lower histological grade was associated with pCR [927]. In our study, well-differentiated tumor was associated with good tumor response and was also an independent predictor of stage ypT0–1N0 on multivariable analysis. This finding is consistent with data from previous studies [69].
On univariable analysis, fungating tumor morphology and an anterior/posterior direction for the circumference were associated with good tumor response; however, fungating tumor was not significantly associated with stage ypT0–1N0 on multivariable analysis. To the best of our knowledge, no previous study provides a clear explanation for the varying responses to CCRT according to a tumor’s direction or morphology. Presumably, the radiation dose may be greater in a fungating mass with a larger surface area than in a flatter mass. Studies on the characteristics of tumors, as identified by endoscopy or DRE, are few. Park et al. [6] assessed tumor movability and morphology via DRE and reported that DRE was an accurate method for predicting pCR after CCRT. They suggested that a combination of clinical, laboratory, and metabolic data would best predict pCR. However, other studies reported DRE and endoscopy as poor methods for distinguishing between postradiation fibrosis and residual cancer [282930]. Notably, all these studies assessed tumors after CCRT to determine whether pCR was achieved but did not attempt to predict tumor response based on pretreatment gross morphology. In contrast, our study demonstrated some value for endoscopy, which was used to assess the primary tumor morphology, and reported that endoscopy is clinically important in planning treatment based on a good response to CCRT to ensure organ preservation. A prospective study is needed to verify the value of pretreatment gross morphology.
Our study has some limitations. First, the data were derived from a single institution. A multicenter study with a prospective design may provide additional reliable predictors of response to CCRT. Second, owing to the study’s retrospective nature, the data were extracted from medical charts; therefore, selection bias is inevitable. Given the finite extent of the available data, only a limited number of variables were analyzed. Although a large number of patients received neoadjuvant CCRT for rectal cancer at our center during the study period, those who did not undergo subsequent surgery were excluded. Moreover, clinical decisions were often made according to the physicians’ discretions. A prospective study may be able to evaluate additional variables that have recently received attention in the field. Even with these limitations, this is the first study evaluating the predictive factors of good response to achieve stage ypT0–1N0 which affords eligibility for transanal local excision that allows for nonradical treatment after neoadjuvant CCRT in patients with middle or low rectal cancer.
In conclusion, our study revealed that stage cT1–2 and well differentiation are predictors of stage ypT0–1N0, which in turn may provide an important and consistent indication for nonradical treatment after CCRT. Fungating tumors could be considered clinically meaningful, which may help in identifying candidates for nonradical treatment post-CCRT. These variables may also be used to stratify patients who participate in prospective studies aimed at developing new strategies for the treatment of rectal cancer.
 XML Download
XML Download