

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Adrenal insufficiency (AI) is a life-threatening condition that increases the risk of readmission and mortality.12 AI is caused by an insufficient production of steroid hormones in the adrenal glands, among which glucocorticoids are related to the regulation of blood glucose metabolism, calcium metabolism, growth and development, immune system, cardiovascular system, and central nervous system.3 Patients with malignancy are at a particularly high risk of AI because many cancer patients have a history of steroid use, which is a known risk factor for AI.456 The development of AI is also associated with metastatic lesions in the adrenal glands, resection of the adrenal glands, and the use of immune checkpoint inhibitors.78910 Supplement of glucocorticoids could alleviate AI-related symptoms, but can also lead to adverse effects such as osteoporosis, muscle atrophy, hyperglycemia, dyslipidemia, and heart failure.11 Therefore, it is important to appropriately diagnose and treat AI in patients with malignancy.
AI is diagnosed by performing a rapid adrenocorticotrophic hormone (ACTH) stimulation test, which involves the measurement of blood cortisol levels in serial blood samples.12 However, it is difficult to measure serial blood cortisol levels in the outpatient setting. Moreover, the common presenting symptoms of AI—general weakness, fatigue, weight loss, loss of appetite, nausea, vomiting, myalgia, hypoglycemia, hypotension, and fever13—are also often caused by advanced cancer or chemotherapy, thereby hindering the discerning of the cause of these symptoms and making a timely diagnosis of AI in cancer patients.
Hospitalist units were introduced to Korea in the late 2010s in order to reduce the workload of clinicians and improve the safety and in-hospital management of patients.14 Importantly, hospitalist units may have a unique advantage in examining the prevalence and clinical features of AI in cancer patients because patients hospitalized in these units have ample time for rapid ACTH tests and their symptoms are closely and continuously observed by dedicated hospitalists. Therefore, in this study, we aimed to analyze the prevalence and risk factors of AI in cancer patients being treated at a medical hospitalist unit, and tried to determine the values of a single cortisol level that can predict the occurrence of AI in cancer patients.
METHODS
Patients and study design
This retrospective study was conducted in patients with malignancy who were suspected of AI and underwent a rapid ACTH stimulation test during admission at the medical hospitalist unit at Asan Medical Center (Seoul, Korea) between January 2020 and June 2021. The medical hospitalist team at our institution is operated in two wards and is composed of 11 internal medicine specialists (hospitalists) who provide medical care 24 hours a day, 365 days a year.
Rapid ACTH stimulation tests were performed when the hospitalists decided to determine if symptoms such as general weakness, weight loss, loss of appetite, nausea, vomiting, and abdominal pain were associated with AI and not advanced cancer or chemotherapy, or if the reason for the signs such as hyponatremia, fever, and hypotension were not clear and AI should be ruled out. Baseline characteristics, laboratory findings, and clinical outcomes of the study patients were reviewed through electronic medical records.
ACTH stimulation test
Rapid ACTH stimulation tests with 250 μg of synthetic ACTH (Tetracosactrin, Synacthen® DALIM BIOTECH, Wonju, Korea) were used for the diagnosis of AI. The tests were started in the morning at 8 AM; after collecting baseline serum cortisol and plasma ACTH by blood sampling, synthetic ACTH was administered intravenously. Additional serum cortisol levels were collected twice at 30 and 60 minutes after synthetic ACTH injection. AI was defined when the peak cortisol level after synthetic ACTH administration was less than 18 μg/dL (500 nmol/L).12
Definitions
Eosinophilia was defined as an eosinophil count of more than 500 cells/μL.15 Chronic kidney disease was defined as a glomerular filtration rate of less than 30 or the requirement of renal replacement therapy such as dialysis. Corticosteroid and megestrol acetate usage were classified into using any duration, more than 7 days, and more than 30 days according to the cumulative period. Corticosteroid doses were classified according to the prednisone equivalent dose as low dose (≤ 7.5 mg/day), medium dose (7.5–30 mg/day), and high dose (> 30 mg/day). Immune checkpoint inhibitors included PD-1 inhibitors (i.e., pembrolizumab, nivolumab) and PD-L1 inhibitors (i.e., atezolizumab, avelumab).161718 The primary outcome was independent risk factors for AI, and the secondary outcome was the ideal baseline cortisol cutoff for predicting AI.
Statistical analysis
Categorical variables were compared using the χ2 test or Fisher’s exact test, as appropriate, and continuous variables were compared using Student’s t-test or Mann-Whitney U test, as appropriate. All tests of significance were two-tailed, and P values < 0.05 were considered statistically significant. Risk factors for the occurrence of AI in patients with malignancy were analyzed using logistic regression analysis. We fitted multiple logistic regression model with variables that were included by backward elimination with P value threshold < 0.2. Variables with clinical importance, such as sex and immune checkpoint inhibitors, were included additionally. The diagnostic accuracy of the baseline cortisol level was assessed using receiver operating characteristic (ROC) curves, and the Youden index was used to select the optimum cutoff points on the ROC curves (optimal balance between sensitivity and specificity). Statistical analyses were performed using SPSS for Windows software package, version 24 (SPSS Inc., Chicago, IL, USA), and ROC curves were drawn using the R Studio (version 1.4.1717; R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org).
Ethics statement
This observational study was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2021-1185). To protect personal privacy, identifying information in the electronic database was encrypted. Informed consent was waived by the IRB because no intervention was involved and no patient-identifying information was included.
RESULTS
Clinical features of hospitalized patients with malignancy
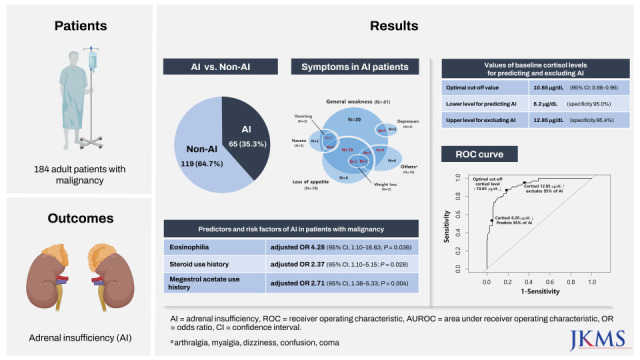
During the study period, 3,201 patients with malignancy were hospitalized, of whom 184 (5.7%) patients underwent a rapid ACTH stimulation test. Of them, 65 (35%) patients were diagnosed with AI. Table 1 shows the baseline characteristics of patients with AI (n = 65) and those without (n = 119). The median age of the AI group and the non-AI group was 69 years and 66 years, respectively (P = 0.130), and the proportion of male sex was not significantly different between the two groups (60% vs. 58%; P = 0.791). Except for chronic kidney disease (11% vs. 3%; P = 0.043), the distribution of underlying diseases was not significantly different between the two groups. General weakness (63% vs. 52%) and loss of appetite (28% vs. 33%) were the most common symptoms in both groups. In the AI group and the non-AI group, 15 (23.1%) and 39 (32.8%) patients did not have overt symptoms, respectively. The total sum of symptomatic cases was 126% when considering overlapping symptoms.
Table 1
Baseline characteristics of hospitalized patients with malignancy

Data are presented as median (interquartile range), number (%), or mean ± standard deviation.
AI = adrenal insufficiency, COPD = chronic obstructive pulmonary disease, ACTH = adrenocorticotropic hormone, WBC = white blood cell, Hb = hemoglobin, qSOFA = quick Sepsis Related Organ Failure Assessment, PD-1 = programmed cell death protein 1, PD-L1 = programmed cell death-ligand 1.
aArthralgia, myalgia, dizziness, confusion, coma.
b≤ 7.5 mg/day of prednisone equivalent.
c> 7.5 mg/day and ≤ 30 mg/day of prednisone equivalent.
d> 30 mg/day of prednisone equivalent.
*P < 0.05, **P < 0.01, ***P < 0.001.
In terms of laboratory findings, the AI group and the non-AI group did not show significant differences except for cortisol levels (all P < 0.001) and the proportion of those with eosinophilia (12% vs. 3%; P = 0.019). In the AI group, the mean levels of ACTH and cortisol at 60 minutes were 47.5 ± 100.5 pg/mL and 12.6 ± 4.2 μg/dL, respectively.
In terms of medication history, the AI group had higher proportions of patients who used corticosteroids for more than 7 days (49% vs. 32%; P = 0.021) or 30 days (34% vs. 17%; P = 0.008) than the non-AI group. Megestrol acetate use of any duration was significantly more common in the AI group (60% vs. 33%; P < 0.001), but the use of immune checkpoint inhibitors was not significantly different between the two groups (14% vs. 10%; P = 0.443).
In the AI group, the rates of readmission and in-hospital mortality were 34% and 29%, which were not significantly different from those of the non-AI group (28%, P = 0.386; 42%, P = 0.087, respectively).
The distribution of the types of malignancy is shown in Table 2. The underlying malignancy in the AI group and the non-AI group was solid cancer in 80% and 85% (P = 0.523), respectively. Of the 8 patients with multiple myeloma who were suspected of having AI, 7 (87.5%) were diagnosed with AI (P = 0.003). No statistically significant difference between the AI group and the non-AI group was observed in other malignancies.
Table 2
Types of malignancy in hospitalized patients
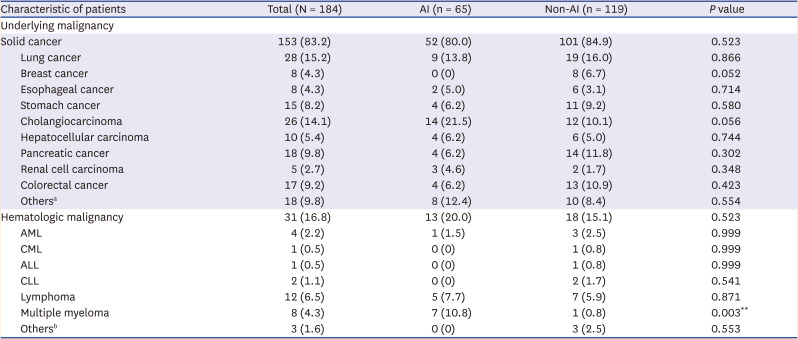
Data are presented as number (%).
AI = adrenal insufficiency, AML = acute myeloid leukemia, CML = chronic myeloid leukemia, ALL = acute lymphoblastic leukemia, CLL = chronic lymphocytic leukemia.
aFive gallbladder cancer, three prostate cancer, three bladder cancer, two tongue cancer, one duodenal cancer, one ovarian cancer, one small bowel gastrointestinal stromal tumor, one neuroendocrine tumor, and one angiosarcoma were included.
bThree myelodysplastic syndrome were included.
**P < 0.01.
Predictors and risk factors for AI in hospitalized patients with malignancy
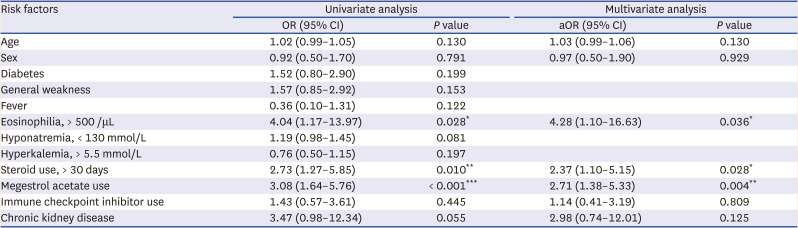
Multivariate analysis showed that eosinophilia (> 500/μL) (adjusted odds ratio [aOR], 4.28; 95% confidence interval [CI], 1.10–16.63; P = 0.036), steroid use for more than 30 days (aOR, 2.37; 95% CI, 1.10–5.15; P = 0.028), and megestrol acetate use of any duration (aOR, 2.71; 95% CI, 1.38–5.33; P = 0.004) were significantly associated with the occurrence of AI in hospitalized patients with malignancy (Table 3).
Table 3
Univariate and multivariate analysis of predictors and risk factors for adrenal insufficiency in hospitalized patients with malignancy
Predicting and excluding values of baseline cortisol level for AI in hospitalized patients with malignancy
Fig. 1. shows the ROC curve of baseline cortisol for predicting AI. The area under ROC was 0.92 (95% CI, 0.88–0.96). The optimal cutoff value as determined by the Youden index was 10.65 μg/dL, at which the sensitivity and specificity were 87.7% and 80.7%, respectively. At 6.2 μg/dL and 12.85 μg/dL, the sensitivities of baseline cortisol were 53.9% and 65.6%, respectively, and the specificities were 95.0% and 95.4%, respectively (Table 4).
Fig. 1
Receiver operating characteristic curve of baseline cortisol for predicting adrenal insufficiency in hospitalized patients with malignancy.
AI = adrenal insufficiency, AUROC = area under receiver operating characteristic, CI = confidence interval.
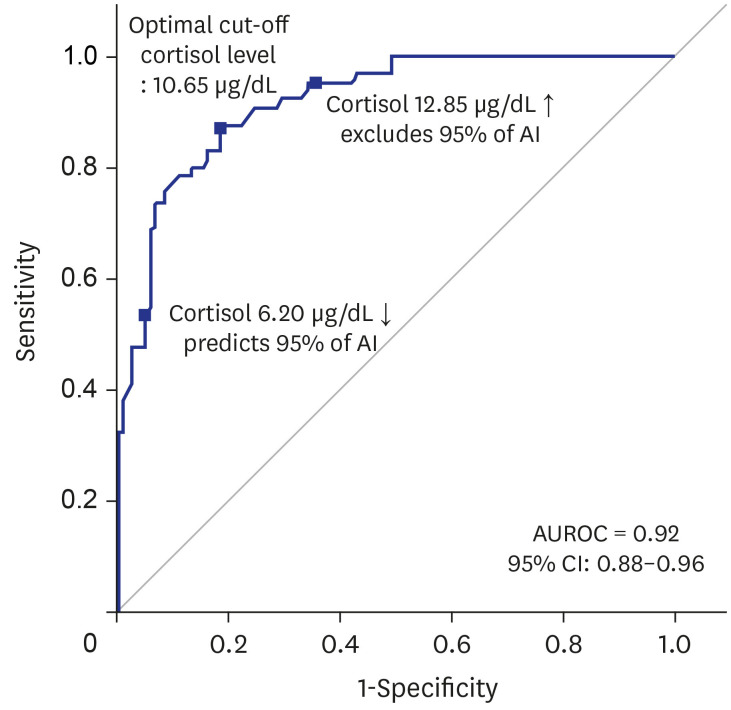
Table 4
Baseline cortisol levels for predicting and excluding adrenal insufficiency in hospitalized patients with malignancy

DISCUSSION
Patients with malignancy have multiple risk factors for the development of AI, and steroid replacement offers significant benefits in cancer patients with AI; however, studies on the risk factors of AI in cancer patients are lacking. To our knowledge, this is the first study to evaluate clinical features of cancer patients with AI, identify the risk factors thereof, and determine the optimal baseline cortisol levels for predicting AI in such patients. By analyzing a cohort of cancer patients admitted to our hospitalist unit, we found that AI was quite common (35%) among cancer patients who showed relevant symptoms and signs such as general weakness and loss of appetite, which are prevalent among cancer patients receiving chemotherapy. Corticosteroid use and megestrol acetate use were independent risk factors for AI, and eosinophilia was an independent pre-test predictor of AI. Importantly, a baseline cortisol level of 10.65 μg/dL was determined as the optimal cutoff for predicting the development of AI (sensitivity, 87.7%; specificity, 80.7%), which may be useful in situations such as outpatient clinics in which serial testing for cortisol levels cannot be performed.
Of the 184 patients with malignancy who underwent a rapid ACTH stimulation test, 65 (35.3%) were confirmed with AI, suggesting that as much as one-third of patients with ongoing advanced cancer or chemotherapy may have AI if they complain of symptoms such as general weakness, loss of appetite, and nausea. Therefore, clinicians and hospitalists should be aware of the possibility of accompanying AI when patients with malignancy persistently complain of the abovementioned symptoms despite symptomatic treatment. Interestingly, although the overall incidence of multiple myeloma was small (8/184 [4.3%]), we found that the proportion of patients with multiple myeloma was significantly higher in the AI group than in the non-AI group (11% vs. 1%; P = 0.003). We assume that this was because patients with multiple myeloma tend to receive repeated treatments with salvage regimens including high-dose glucocorticoids.1920
In our results, eosinophilia was a significant pre-test predictor for the occurrence of AI. It is not clear why eosinophilia was associated with AI, but the modulation of the expression of adhesion and migration factors by corticosteroids may result in a higher transition rate of eosinophils out of the bloodstream to tissues and confer an eosinopenic effect by stimulating eosinophil apoptosis.212223 Therefore, it is plausible that eosinophilia may be a direct effect of the corticosteroid deficiency caused by AI, and eosinophilia can be utilized as a marker of the possible existence of AI. Other laboratory findings that were known to be related to AI, such as hypoalbuminemia or hyponatremia, had no statistical significance in the prediction of AI; this is presumably because cancer patients often have decreased oral intake due to chemotherapy and cachexia.
We also found that history of steroid and megestrol acetate use were significant risk factors for increasing the incidence of AI. The mechanism by which steroids cause AI is relatively well-known: when corticosteroids are administered, cortisol regulation and releasing system functions are suppressed due to the hormone feedback system.242526 Accordingly, previous studies have reported that the use of dexamethasone for anti-emesis in cancer patients receiving chemotherapy could cause AI.42526 Our finding is consistent with these previous findings. In terms of megestrol acetate, only a few case reports272829 and one recent retrospective study20 reported the history of megestrol acetate use as a risk factor for AI. Through multivariable analysis that adjusted for confounding variables, our study provides further evidence that megestrol acetate could cause AI in patients with malignancy.
A total of 21 (11.4%) patients received immune checkpoint inhibitors, of whom 9 (42.9%) were diagnosed with AI. The development of AI-related to immune checkpoint inhibitors is a critically important issue, as the use of immune checkpoint inhibitors is increasing in cancer patients and their effects are irreversible.161718 Although more than 40% of the suspected patients treated with immune checkpoint inhibitors were diagnosed with AI, the proportion of patients treated with immune checkpoint inhibitors did not significantly differ between the AI group and the non-AI group. Further studies with larger cohorts are needed to clarify this issue.
Our study provides valuable information on predicting AI based on baseline cortisol level in patients with malignancy. A previous study also evaluated the predictive value of baseline cortisol on the development of AI,30 but none has focused on patients with malignancy. We therefore determined the diagnostic performance and usefulness of baseline cortisol levels in a specific population with malignancy. Our results showed that AI can be predicted with a 95% probability if the baseline cortisol level is less than 6.2 μg/dL, and AI can be excluded with a 95% probability if the baseline cortisol level is over 12.85 μg/dL. These cortisol level values were similar to those reported in other studies; one study suggested that AI could be excluded with a 95% probability when the baseline cortisol level was higher than 12.7 μg/dL,30 and suggested that the optimal baseline cortisol level for predicting AI with a 95% probability was 4.5 μg/dL.30 Our findings on the value of baseline cortisol would be useful for clinicians seeking to predict the risk of outpatients with malignancy or those with poor vessel conditions, in whom measuring serial blood cortisol levels after injection of cortisol stimulating hormone is difficult.
Hospital medicine aims to improve the quality and efficiency of generalized care for hospitalized patients.31 Because medical hospitalist units in Korea are mainly operated in tertiary hospitals, the proportion of cancer patients in those units is high. In this study, the presence of AI was not significantly associated with the reduction of mortality rate and readmission rate. Yet, the prediction of AI in cancer patients will be of great help in improving the quality of life in patients and the quality of inpatient care in hospitalist units.
This study had a few limitations. First, selection bias might be present because it is a retrospective study conducted at a single center and ACTH stimulation tests were only conducted on patients who were clinically suspected of AI. This selection bias hinders the generalization of the high incidence rate of AI (up to 35%) in patients with malignancy. Therefore, further studies are needed by securing participation from multiple centers, and well-designed studies are also needed to define the criteria for performing ACTH stimulation tests in cancer patients. Second, AI might have been over-diagnosed because of the inherent limitations of rapid ACTH stimulation tests. The rapid ACTH stimulation test measures cortisol levels in the blood, which are mostly bound with proteins such as corticosteroid-binding globulin or albumin. This could be affected by the fact that patients with malignancy often have hypoalbuminemia due to chronic inflammation, decreased systemic protein synthesis, decreased liver function, malnutrition, and changes in the normal distribution of albumin.32 However, within our limited data, albumin levels were not significantly associated with the occurrence of AI. Further studies are needed to evaluate the occurrence of AI in patients with hypoalbuminemia. Despite these limitations, our study is meaningful in that it examined the incidences and risk factors of AI in patients with malignancy.
In conclusion, AI was diagnosed in more than one-third of cancer patients at a medical hospitalist unit who complained of common symptoms such as general weakness and loss of appetite. Patients with eosinophilia and history of corticosteroids or megestrol acetate use should be closely monitored for the development of AI. Baseline cortisol level may be a useful adjunct marker for AI.
 XML Download
XML Download