

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As serving the military is mandatory in Korea, establishing adequate environments to help enlisted personnel in adapting to the service is an essential national assignment.1 However, it is suggested that the hierarchical structure of military command and obligatory enlistment elevate the occurrence of depression and hinder adapting to the service.23 Furthermore, Navy recruits have several additional risk factors which hamper mental health: harsh climate, noise, deterioration of circadian rhythm, social isolation and less opportunity to get proper medical management.45 In regards to these circumstances, it is not surprising that depression is prevalent in the seafarers, reported up to 25%.67 Moreover, the seafarers have been ranked as one of the occupation with the highest suicide rate.8 Psychologic stress and mental health in the seafarers have become important issues that occupational efficacy and long-term health outcomes are readily affected.910
Almost all ship travelers could have seasickness according to the roughness of waves.11 Motion sickness in the sea could be induced by passive locomotion of the ship inducing intersensory conflict between vestibular and visual pathways.1213 Although seasickness is a physiologic response to the sensory conflict, seasickness substantially affects occupational role and adjustment to seafaring and is thus needed to be managed properly. Considering the importance of depression and seasickness in seafarers; however, the relationship between depression and seasickness has not yet been elucidated. As a depression screening tool is feasible and has been widely applied to assess depression and its relationship with other medical conditions,141516 in this study, we aimed to evaluate the association between depression scale and seasickness in Navy recruits.
METHODS
Study population
The retrospective cohort study included recruits who were firstly designated to a naval ship and never sailed before from July 2017 to March 2019. Among the newcomers, the participants who served less than 5 distant seafaring days were excluded. The ship was 1st class naval ship that sails distant seas. As this study included only those subject to mandatory service, and all participants were male.
Data collection and outcome assessment
On the day of ship boarding, all recruits underwent routine physical examinations for newcomers including diastolic and systolic blood pressure measurement and individual interviews performed by a physician served in the ship’s infirmary. The Beck Depression Inventory (BDI)17 was mandatorily conducted for screening participants with depression before starting the military service. Recruits with BDI score of 10 or more were consulted and referred to a proper psychological management. Information on age and the workplace was obtained. The workplace in the ship was classified into where external visual input is perceptible including deck and bridge of the ship and imperceptible including occupations inside the ship.
The occurrence of seasickness requiring treatment was retrospectively collected. In this study, we collected the medication prescription records for the first 30 distant seafaring days. All members who needed medical consultation or prescription were referred to the physician on board. For patients with seasickness requiring treatment, antihistamine agent (a single dose of dimenhydrinate 50 mg) was prescribed and intermittent resting was guaranteed in the infirmary or individual’s bedroom. When the patient’s symptoms and signs correlated with seasickness, the medication was prescribed if contraindications of antihistamine drug were absent. All patients considered on prescription had no contraindication.
According to the previous literature that adjustment period about several days13 might be needed for seasickness in seafarers, we separately collected the outcome in the first 5 distant seafaring days (early period) and thereafter (6–30th seafaring days, late period). We established two different outcomes to distinguish the initial susceptibility (in the early period) and the adaptation ability to seasickness (in the late period). During the early period, the susceptibility to seasickness was evaluated as whether the participant had at least one prescription. For the late period, we calculated the adaptation ability as the ratio of medication prescription days/seafaring days. We defined poorly adapted individuals as the above-mentioned ratio of more than 10% and well-adapted individuals ≤ 10%. This ratio may be a factor that could significantly hinder occupational performance.
Statistical analysis
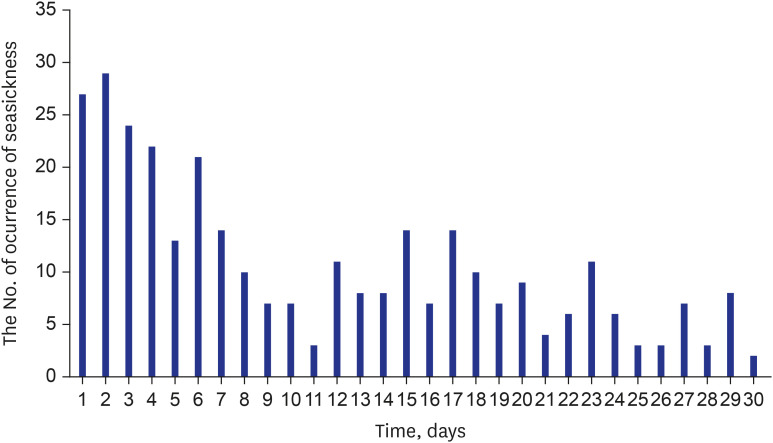
The temporal trend of seasickness was plotted with time (day) as a X-axis and the proportion of patients with treatment required seasickness as a Y-axis. The analyzable population was divided into 3 groups according to BDI scores: BDI score of 0 as no depression, BDI score of 1–9 as minimal depression, and BDI score of 10–29 as mild-to-moderate depression.18 Recruit with severe depression (BDI score ≥ 30) was absent amongst included participants. Comparisons of baseline routine examination and outcomes were made using the χ2 test for categorical and analysis of variance for continuous variables. Binary logistic regression models were used for two outcomes. Unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for the initial susceptibility of the minimal and mild-to-moderate depression groups with no depression group as a reference (Model 1) and BDI score as a continuous variable (Model 2) were estimated. Furthermore, ORs and 95% CIs were estimated for the adaptation ability. Covariates were predetermined: age and the workplace with external visual perception or not.11 Data were analyzed using R 4.1.3 and a P value < 0.05 was defined statistically significant.
RESULTS
Baseline characteristics and outcomes
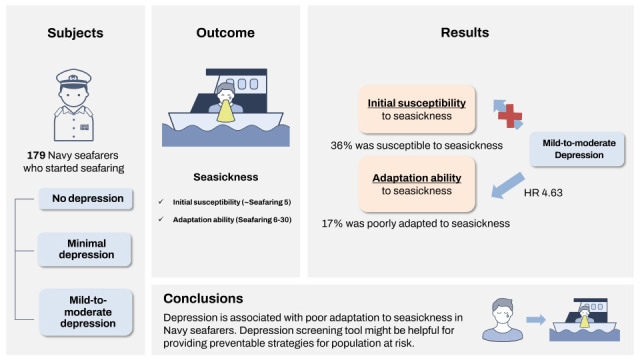
Out of a total 185 newcomers, BDI was assessed in all participants. A total of 179 participants (97%) who served for more than 5 distant seafaring days were analyzed. Median follow-up days of seafaring were 30 days (interquartile range [IQR] 29–30). Among the analyzable population, a total of 318 days of seasickness requiring treatment were observed during the 5,044 seafaring days. The ratio of the seasickness days to seafaring days in the early and late period were on average 13.3% and 6.1%, respectively. The occurrence of treatment requiring seasickness according to seafaring days was described in Fig. 1. Seventy-one participants (39%) were never treated with seasickness. A total of 64 patients (36%) was susceptible to seasickness in the early period. Thirty-one patients (17%) were poorly adapted to seasickness in the late period.
Depression scale and outcomes
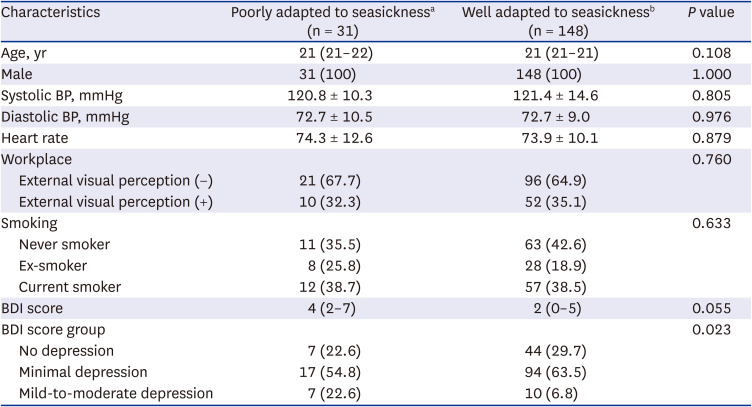
Amongst the population, participants with mild-to-moderate depression were 17 (9.4%) and minimal depression were 112 (61.7%) while no depression were 51 (28.3%). Median of BDI score in the analyzable population was 2 (IQR 0–6). Baseline characteristics according to the BDI score groups were demonstrated in Table 1. Among three groups, the proportions of poor adaptation in the late period were different (41% vs. 15% vs. 14%) that patients with mild-to-moderate depression had the highest rates of poor adaptation. There was no significant difference in the susceptibility in the early period among the groups. Ratio of suffered/seafaring days during the overall period were different that mild-to-moderate depression showed around 14% of days suffered from seasickness.
Table 1
Baseline characteristics according to the depression scale
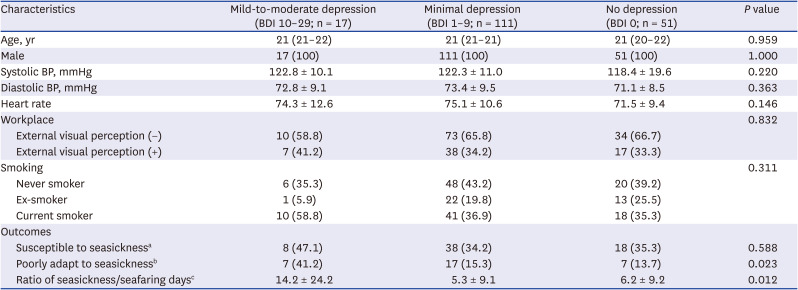
Values are presented as median (interquartile range), number (%) or mean ± standard deviation.
BDI = Beck Depression Inventory, BP = blood pressure.
aThe presence of at least one seasickness requiring treatment during the first 5 distant seafaring.
bThe ratio of seasickness days requiring treatment/seafaring days > 10% during the 6–30 distant seafaring.
cThe ratio of seasickness days requiring treatment/seafaring days during the overall period.
Comparing participants regarding susceptibility to seasickness in the early period, BDI score as a continuous variable and BDI sub-groups were not significantly different (Table 2). However, poorly adapted participants in the late period had a trend of higher BDI score although not statistically significant (median 4, IQR [2–7]) compared to those who are well-adapted (2 [0–5]) (P = 0.055) (Table 3). Proportions of mild-to-moderate depression (22.6%) were higher in the poorly adapted group compared to the well adapted group (6.8%, P = 0.023).
Table 2
Comparing characteristics and BDI depression scores regarding sea-sickness susceptibility in the early period
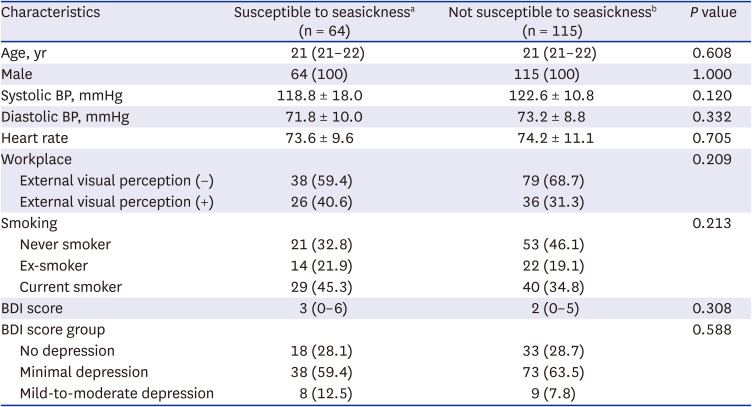
Values are presented as median (interquartile range), number (%) or mean ± standard deviation.
BDI = Beck Depression Inventory, BP = blood pressure.
aThe presence of at least one seasickness requiring treatment during the first 5 distant seafaring.
bThe absence of at least one seasickness requiring treatment during the first 5 distant seafaring.
Table 3
Comparing characteristics and BDI depression scores regarding adaptation ability to sea sickness in the late period
Values are presented as median (interquartile range), number (%) or mean ± standard deviation.
BDI = Beck Depression Inventory, BP = blood pressure.
aThe ratio of seasickness days requiring treatment/seafaring days > 10% during the 6–30 distant seafaring.
bThe ratio of seasickness days requiring treatment/seafaring days ≤ 10% during the 6–30 distant seafaring.
Multivariable analysis
In binary logistic regression models, BDI groups and BDI score did not significantly elevate the odds for susceptibility to seasickness in the early period (Table 4). On the other hand, mild-to-moderate depression independently increased the odds for poor adaptation to seasickness in the late period by OR, 4.63 (95% CI, 1.31–16.98). Furthermore, every 1 increment in BDI score increased odds for poor adaptation to seasickness by 1.10.
Table 4
Unadjusted and adjusted odds of the depression scale for the susceptibility in the early period and adaptation ability in the late period
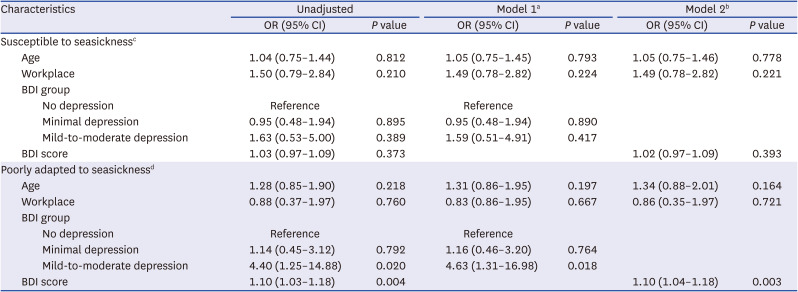
BDI = Beck Depression Inventory, OR = odds ratio, CI = confidence interval.
aBDI was assessed as a categorical variable (no depression, BDI 0; minimal depression, BDI 1–9; mild-to-moderate depression, BDI 10–29).
bBDI was assessed as a continuous variable.
cModel was evaluated for the early period outcome (the presence of at least one seasickness requiring treatment during the first 5 seafaring days).
dModel was evaluated for the late period outcome (the ratio of days of seasickness requiring treatment/days of seafaring > 10% during the 6–30 distant seafaring).
DISCUSSION
In the current study, mild-to-moderate depression was associated with poor adaptation ability to seasickness in the naval crew. On the other hand, depression scale was not significantly associated with the initial susceptibility to seasickness. The ratio of days suffered from seasickness requiring treatment was greater in the mild-to-moderate depression group compared to none or minimal.
As this study was conducted for Navy recruits who were naïve to seafaring, we could evaluate the early period for initial susceptibility to seasickness and the late period for adaptation to seasickness. The recent research including college students’ first experience sailing suggested gender, age, and birthplace were associated with motion sickness susceptibility but psychological factors were not evaluated in the study.19 The current study suggested depression could be associated with naïve seafarers’ adaptation ability to seasickness. The relationship between psychological status and motion sickness on the laboratory-based research has been explored.20 Psychological status and motion sickness evaluated by Hospital Anxiety and Depression Scale was associated with inability in updating orientation after a rotation test. Here, we stated the association between depression and seasickness in the real-world setting.
Among various possible explanations for motion sickness, the sensory conflict has been widely accepted in the literatures.21 According to this theory, if discrepancy in sensory signals from proprioception, visual, and vestibular system occur, the motion sickness is provocated.22 Seasickness and car-sickness could also be triggered by suppression of vestibule-ocular reflexes. In the current study, we included the workplace as a covariate that outside workers could have more chances to alleviate sensory conflict by looking sea which was associated in the previous literature.11 However, the workplace in the ship was not associated with seasickness requiring treatment. Not constricted to the spatial meaning, the workplace implies the different roles, stress, social, and environmental factors that could not be simply defined as a factor reflecting visual perception.
In regards to adaptation, if the conflict of sensory signals is estimated, neural mismatch does not always result in the development of motion sickness.23 It is presumed that discrepancy in sensory information is stored in the hippocampus and the vestibular cortex.24 Therefore, the motion sickness after exposure to conflict stimuli might be determined with the function of individual’s sensory center as well as a degree and types of sensory conflict. It is suggested that neural plasticity and neuronal adaptation are commonly disrupted in depression via N-methyl-D-aspartate receptor in the amygdala of hippocampus.25 Impairment in vestibular system was also associated with increased risk of depression and memory function.26 Therefore, this could also apply to the main finding of this study. Hindered adaptation to seasickness in depression patients could be partly explained by possible deterioration of hippocampal and vestibular system in depression.
Neural circuits including cholinergic, histaminergic, dopaminergic, and serotonergic system might be involved in the development of motion sickness.1323 In depressive patients, decreased serotonergic function has been suggested as a pathophysiologic mechanism and symptoms were associated with the decreased level of serotonin.27 Decreased activity in the dopaminergic pathway in the limbic system and the level of norepinephrine were also related to depression.2829 These neurotransmitters, thus, become major targets for pharmacological treatment in depression. Therefore, decreased activity in these neural circuits in the depressive patients could be associated with the occurrence of motion sickness. Furthermore, patients with migraine were susceptible to motion sickness that the authors suggested tryptophan depletion in these patients could result in decreased synthesis of serotonin and vestibular dysfunction.30 Further studies utilizing neuroimaging tools visualizing neural circuits such as functional magnetic resonance imaging could approach pathophysiologic evidence for relationship between depression and seasickness.
There are several recommendations for helping adaptation to seasickness in seafaring. Pharmacological option includes antihistamine agent which reduces the sensory conflict and enhances adaptation to seasickness.1331 Active body motion,1332 exposure to more gradual onset stimulus33 and accumulated experience of seafaring1334 could aid in adaptation. As a depression screening tool is feasible even in a large group of population,3353637 the tool could be used for military seafarers in screening those with depression as well as those at risk of poor adaptation to seasickness in advance. Careful support from superiors and colleagues might help seafarers to well adapt to seasickness and military service.38
This study has strengths in that the environments of the participants enrolled were relatively well controlled in this cohort. The participants were exposed to homogenous environmental stimuli such as similar locomotive force from the ship, food intake, and life cycles. As motion sickness could be largely affected by such environmental factors, the study design and population selection are often difficult. We could overcome this limitation by constructing a well-controlled homogenous cohort in a particular ship. Furthermore, the dropout rate (3.2%) was low that the result of this study could be less affected by potential selection bias.
This study has a few limitations. First, the result of the current study should be cautiously interpreted as it only included participants with first seafaring. The previous study compared motion sickness in seafarers and non-seafarers that reported veteran seafarers had lower susceptibility to seasickness compared to non-seafarers.39 Differential effects of depression on the seasickness for naïve and veteran seafarers are to be further investigated. Second, this study assessed seasickness requiring treatment and much milder seasickness was excluded. Only significant outcomes resulting in diminished standards of work performance due to seasickness in this population were evaluated. Furthermore, prescription-based assessment could be more objective than motion sickness questionnaires. Third, this study was conducted in a large-sized ship sailing distant seas and those of small-sized ships were not included. Fourth, the sample size was limited and further investigation with larger dataset would support the finding of this study.
In the current study, depression was associated with poor adaptation to seasickness in Navy recruits of first seafaring. Depression screening tool might be used to find seafarers with difficulties in adapting to seasickness in advance. Preventing strategies for these population at risk including pre-medication before seafaring could be considered.
 XML Download
XML Download