

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The emergence of the coronavirus disease 2019 (COVID-19) has evoked an interest in research concerning its psychological impact in addition to it being a global health crisis.1234 Following the outbreak of the COVID-19 pandemic, many countries implemented social distancing measures such as stay-at-home orders, which in turn affected the daily lives of people worldwide. According to a UNESCO report in March 2020,5 more than 90% of the world’s schools have been temporarily closed to mitigate the spread of COVID-19. In South Korea, the government implemented social distancing measures from March 2020. Part of these measures involved elementary school classes being offered online as a form of home-based learning. With growing concern about the interrupted learning and students’ opportunities for growth and developmental loss due to the lack of teacher-child, inter-colleagues interaction, and reduced role tasks, a hybrid model was started in June 2020.67 A hybrid model was school modification which combined online and full in-person class because the number of students attending school had to be adjusted according to the density. After it changed, children were required to physically attend school one to three days a week, depending on school size and their school year, and engage in home-based learning for the remaining weekdays. At school, children were seated separately and asked to keep their masks on and minimize their conversations with classmates.
The children who are going through developmental milestones (physical, language, social and moral) would experience the effects of physical and social isolation on an even greater scale.8 Failure to go to school, social isolation, increased screen time, and parental stress are likely to negatively affect children’s mental health.8910 Interaction with peers and support from families are powerful aids for children, but the COVID-19 pandemic has also hindered them. Impoverished children, who may rely heavily on school-based services were disproportionately impacted.1112 Thus, specific studies are needed to determine which groups are more vulnerable to specific elements of the crises and to determine how they may respond to those long-term changes.
Recently, many studies have been conducted on the effects of these social changes on adult mental health, such as a lockdown or longitudinal changes that compared pre- and post-pandemic mental health statuses.1314151617 Although the pandemic has lasted for more than two years, the long-term impact of COVID-19 is still unclear. A longitudinal study of 7,319 Americans reported that psychological distress rose sharply during the early days of COVID-19 and returned to its original baseline after 3 months,18 however, another study argued the population in vulnerable groups were more susceptible to mental health issues during the pandemic.19 In contrast, there are few studies of the impact on children. Therefore, it became necessary to study how the children’s mental health changed from the initial stage to the current stage of the pandemic.20
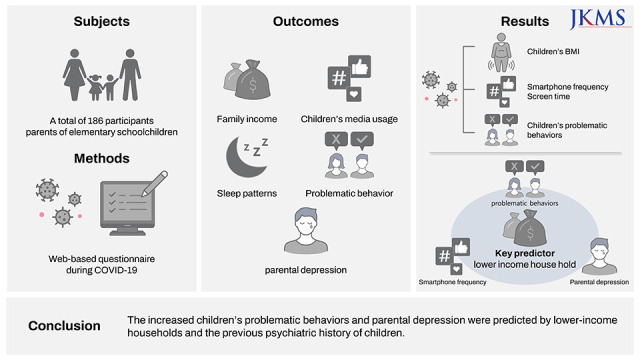
In this study, the primary purpose was to elucidate if there had been any change in children’s and parental mental health problems during the various stages of COVID-19. This was done by comparing their mental health levels or statuses at the time of the initial school closures and 14 months after the hybrid school modification was implemented. In terms of the children’s screen time, behavior problems, sleep problems, and parental depression. The secondary purpose was to identify the various predictors of those potential changes in a longitudinal setting among Korean elementary students during the COVID-19 related school curriculum modifications.
Go to : 
METHODS
Study design and participants
This study was conducted online and completed by the randomly recruited children’s caregivers via emailed link in South Korea. They accessed the web page through an e-mailed link and provided informed consent, reviewed the research guide, and completed the questionnaire.
Using a longitudinal study, surveys were disseminated to a caregiver at two-time points during COVID-19: once at the end of school closures and at the beginning of the hybrid school model (June 2020) and 14 months later during the hybrid or full in-person classes model (September 2021). Earlier data was collected from June 1st to June 30th, 2020, approximately three months after the online-only curriculum (school closure) was implemented in South Korea. The baseline investigations were published that parental subjective stress and depression were strongly and positively associated with children’s sleep problems, media exposure, and problem behaviors.13 The second survey was conducted from September 17th to October 31st, 2021. It was one year after the announcement of a full in-person class was decided. From March 2021, in-person classes were strongly implemented in many elementary schools for grades 1 and 2 children. The combination of online and offline classes was implemented for children in grades 3 and above. For an accurate analysis, there is a strong need for timely longitudinal research that allows a direct comparison of mental health during the school curriculum modifications due to COVID-19 using validated mental health scales to avoid potential errors.21222324
A total of 186 caregivers of elementary school children from community mental health centers in Suwon City, South Korea were randomly recruited. Among participants, the 84 children who had already participated in the Kids Cohort for Understanding of Internet Addiction Risk Factors in Early Childhood (K-CURE) study. Except for 18 people from 9 households, independent families participated. Participants who met inclusion criteria and completed the survey got compensation ($5 worth of hygiene products such as masks). The inclusion criteria were: 1) parents who completed both surveys, 2) parents of primary school children, 3) parents who were able to read and write in Korean.
Measures
Screen time variables
Screen time was investigated by asking primary daytime caregivers to report the frequency per week and time per day of their children’s screen time including television (TV), tablet personal computer (PC), and smartphone in line with the recommendations of previous studies.1325 According to the frequency of use, a request was made to select the number of days each device was used for 1 week. The response options for the mean length of time per day the media were accessed, and the corresponding coded scores were as follows: none (score: 0; less than 1 hour (score: 1); more than 1 hour and less than 2 hours (score: 2); more than 2 hours and less than 3 hours (score: 3); more than 3 hours and less than 4 hours (score: 4); and more than 4 hours (score: 5).
Children’s sleep and behavioral problems
Children's sleep problems were assessed through the parents completing a short version of the Children's Sleep Habits Questionnaire (CSHQ), proven useful in a previous study.13 Parents were asked to recall the sleeping behaviors of their children that occurred over a typical week. Item scores were summed to create a score that could range from 0–12, with higher scores representing greater sleep problems.
Behavioral problems were assessed with the Behavior Problem Index (BPI),26 developed by James L. Peterson, Nicholas Zill,27 and Thomas Achenbach.28 It consists of 27–28 items, 23 common questions and 5 additional questions for those under the age of 11, and 4 additional questions for those over 12. It composed with six domains: “Anxious/Depressed,” “Headstrong,” “Hyperactive,” “Immature Dependency,” “Anti-social,” and “Peer Conflict/Social Withdrawal.” The ratings relied on feedback by caregivers as they were asked to rate their children using a three-point Likert-type scale (0 = not true, 1 = sometimes true, 2 = often true). These questions assess specific behaviors that children may have exhibited in the previous three months. In the current study, Cronbach’s α was .090–.092 in BPI.
Parental mental health (depression)
The Patient Health Questionnaire (PHQ-9) was used similarly as it was in a previous study. Participants were asked to rate nine questions relating to depressive symptoms that they may have experienced in the past two weeks: 0 (not at all), 1 (several days), 2 (more than half the days), or 3 (nearly every day). In the current study, Cronbach's α was .0895–.0916 in PHQ-9.
Family income
Household income was assessed with the question “What is your current average monthly household income?” Caregivers chose from the following response options: “less than $1,700 (two million Korean won, 2M KRW),” “$1,700 (2M KRW) to $3,400 (4M KRW),” “$3,400 (4M KRW) to $5,000 (6M KRW),” and “over $5,000 (6M KRW).” The income level was divided based on 4 million won (approximately $3,400) by referring to the median national income.
Statistical analyses
Variables were summarized via descriptive statistics for demographic information, including frequencies, means, and standard deviations. To compare the differences of mean scores by year, paired t-tests were used. Regression analysis was used to test whether baseline demographic variables predict the variables for those in the year 2021. However, since the normality of the population could not be assumed, the generalized estimating equation (GEE) was applied. GEE was performed with all predictors when they were entered initially. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 25.0 (SPSS Inc., Chicago, IL, USA), and a P value of < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) at the Ajou University School of Medicine, Suwon City, South Korea (IRB No. AJIRB-SBR-SUR-21-345). Informed consent was obtained from all participants at two times of enrollment. Data were collected through a web-based questionnaire platform. Participants could withdraw from the survey at any time without justification.
Go to :
RESULTS
Descriptive statistics of participants
The characteristics of the participants in 2021 and 2020 are shown in Table 1. A total of 186 participants (85.7% response rate) were included in the data analysis. The participant’s mean age was 10.14 years old with a range of 8 to 13 years. Body mass index (BMI) increased significantly in 2021 (18.94 ± 3.75 vs. 18.14 ± 3.30, P < 0.001). However, there was no statistically significant difference in the monthly household income in 2021 and 2020 (P = 0.063). Previous mental health care services that the children were evaluated, and 26.3% of them had a history of psychiatric treatment at both survey time points. Fifteen of these students (8.1%) are in grades 1–2 of elementary school who had attended complete in-person classes without online classes in 2021.
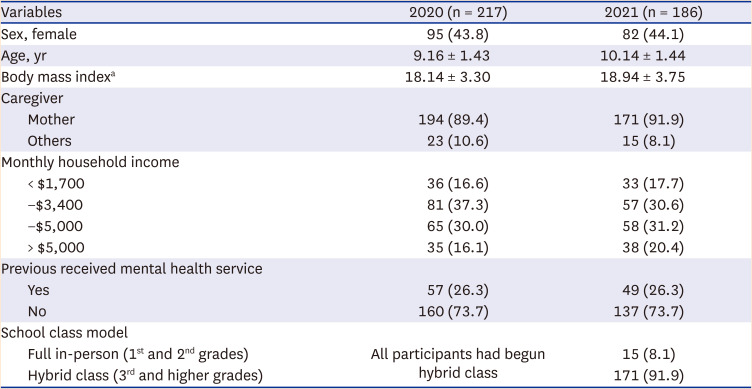
Table 1
Demographic characteristics of study participants in 2020 and 2021
Values are presented as number (%) or mean standard ± deviation.
aindicate statistically significant (P < 0.001).
![]()
Screen time, sleep and behavioral problems in 2021 and 2020
The changes in the children’s screen time, sleep behaviors, and behavioral problems from the longitudinal study are shown in Table 2. Compared to 2020, smartphone screen time, tablet PC screen time per day (respectively, P < 0.001), and smartphone usage frequency per week (P < 0.001) increased significantly in 2021. Contrastingly, the TV usage time and frequency showed a tendency to decline (P < 0.001).
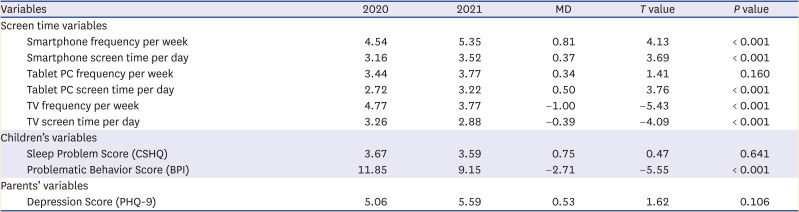
Table 2
Screen time and behavioral problems in 2020 and 2021 (n = 186)
CSHQ = Children’s Sleep Habits Questionnaire, BPI = Behavior Problem Index, PHQ-9 = Patient Health Questionnaire-9.
![]()
The children’s problematic behavior scores were significantly decreased (P < 0.001) from 11.85 to 9.15 between 2020 and 2021. There was no significant change in children’s sleep problems as reported by their parents, or in a parental depression between 2020 and 2021.
To understand the effect of in-person classes, the researchers divided the cross-sectional data for 2021 into two groups according to the grade the children are in (full in-person classes for grades 1–2 vs. hybrid classes for grades 3 and above) to see if there was a difference between them. Through a Mann-Whitney analysis, no difference was found between the children in these groups according to the school modification.
Predictors for screen time and subject’s variables by GEE analysis
This study examined which variables, if any, from the year 2020 could be used to predict screen time in 2021 (Table 3). To understand past predictors, a GEE analysis was performed.
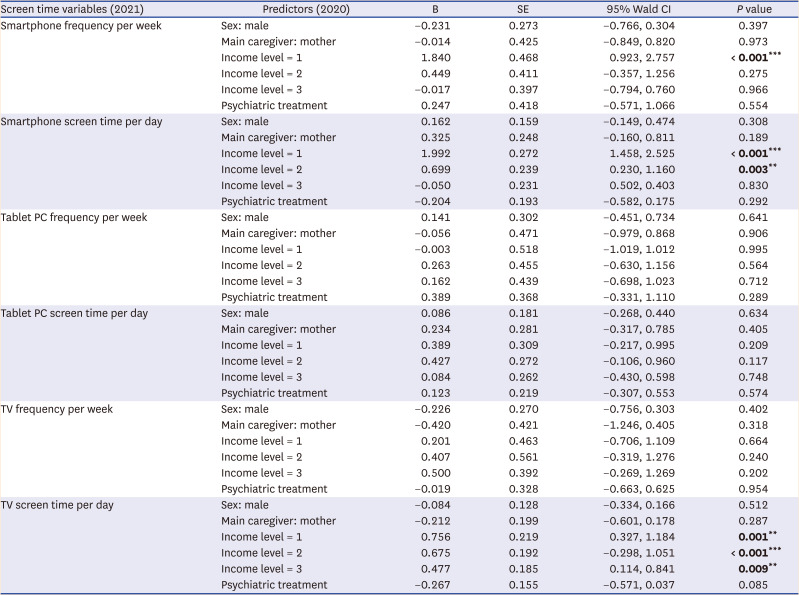
Table 3
Predictors for media usage by generalized estimating equation analysis
CI = confidence interval.
Income level: 1 = less than $1,700; 2 = between $1,700–$3,400; 3 = between $3,400–$5,000; 4 = more than $5,000 per month.
**Significant at P < 0.01, ***Significant at P < 0.001.
![]()
Lower-income (income level 1, less than $1,700 per month) was found to be a significant predictor in 2020, for both smartphone usage frequency per week (B = 1.840, 95% Wald confidence interval [CI], 0.923–2.757, P < 0.001) and smartphone screen time per day (B = 1.992, 95% Wald CI, 1.458–2.525, P < 0.001) in 2021. The income level 2 ($1,700–$3,400 per month) predicted the smartphone screen time per day (B = 0.699, 95% Wald CI, 0.230–1.16, P = 0.003). In terms of decreasing TV usage time, all income levels except the highest in 2020 significantly predicted the TV screen time in 2021.
Additionally, the researchers also examined which variables of 2020 potentially predicted children’s problematic behavior and parental depression in 2021 (Table 4). In children's problematic behavior, lower-income groups (income level 1, B = 5.624, 95% Wald CI, 2.927–8.320, P < 0.001; income level 2, B = 5.023, 95% Wald CI, 2.652–7.394, P < 0.001) and children’s previously received mental health care services in 2020 (B = 7.579, 95% Wald CI, 5.666–9.492, P < 0.001) were significant predictors. In parental depression, lower-income groups (income level 1, B = 3.476, 95% Wald CI, 1.628–5.325, P < 0.001; income level 2, B = 1.807, 95% Wald CI, 0.181–3.243, P = 0.029) and children’s previously received mental health care services were significant predictors (B = 3.138, 95% Wald CI, 1.827–4.450, P < 0.001).
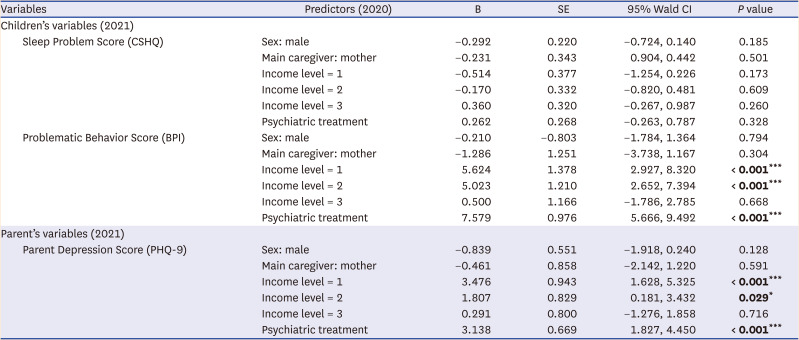
Table 4
Predictors for children’s problematic behavior and parent’s depression by Generalized Estimating Equation
CI = confidence interval, CSHQ = Children’s Sleep Habits Questionnaire, BPI = Behavior Problem Index, PHQ-9 = Patient Health Questionnaire-9.
*significant at P < 0.05, ***significant at P < 0.001.
Income level: 1 = less than $1,700; 2 = between $1,700–$3,400; 3 = between $3,400–$5,000; 4 = more than $5,000 per month.
![]()
Go to :
DISCUSSION
There was an increase in the children’s BMI in 2021. Insufficient outdoor physical activity has been suggested as a major risk factor for overweight pediatric or obesity development.29 It also provided that excessive weight gain in children mainly occurred during the summer, while they were not going to school.30
Previous Korean studies showed the COVD-19 pandemic influence on the increasing childhood obesity rates.31 Specifically, a hospital clinic sample found that being normal range weight was a significant risk factor for increased BMI during school closures, meaning that normal weighted children are more likely to gain weight because of being less alert compared to overweight and obese children about weight gain.31 The duration of school closures was a significant risk factor for increased BMI. They suggested that reopening schools as soon as possible should be a priority for policymakers and should circumstances following the COVID-19 pandemic make school closure indefinite, interventions should be a focused on ways to increase opportunities for physical activity. Unfortunately, this study showed that after reopening the school, within at least one school year was not quick enough and consequently did not prevent the children’s BMI increase. More quantitative and qualitative research on the effects of the changes in the school curriculums and limited outdoor activities has become more urgent than ever before.
Smartphone frequency of use and time spent on devices showed a significant increase in 2021. Despite the full-in person or hybrid classes being possible as compared to 2020 when only full-online classes took place. It reflected the increased use of technology in daily life for academic work, interpersonal meetings, and entertainment purposes.32 However, as the age of the children increases, the frequency and time of media use also increase, and the preferred media pattern changes.33 Additionally, this tendency has been confirmed to occur even if the closure is only for one school year, a long-term study is required.1020
Interestingly, the COVID-19 that lasted for a couple of years showed a relatively adaptive aspect unlike the initial period in terms of problem behaviors of children. Although the main caregiver’s level of depression did not change, the children’s problematic behaviors decreased significantly. According to earlier studies, screen time was closely related to children’s sleep and behavioral problem.34 However, this study showed that children’s sleep problems did not worsen in 2021; this might be due to the reopening of schools that allow them to relearn their previous regular morning routines and assisted in the prevention of the children’s sleep problems due to overnight smartphone use. This contradictory finding could be interpreted in a similar context as the results of previous studies that suggested the trajectory of recovery and adaptation.18
Contradicting other findings, the depression of the primary caregiver did not significantly increase during the survey period. Contrary to general expectations, reopening schools did not affect parental depression in this study. It is estimated that there were limitations and deterioration in the quality of the interaction in the class curriculum and extra-curricular activities.15
In the current study, there were no differences in sleep and behavioral problems between children who attended full in-person classes and hybrid classes according to the administration’s density restrictions. One explanation is that younger children might need more quality interpersonal interactions than older children to keep up to date with their developmental milestones and to maintain their mental health.
Since demographic factors such as gender, primary caregiver, income level, children’s screen time, along with the mental health of caregivers can all be important predictors for mental health, the researchers examined whether those variables from 2020 could predict changes in children’s screen time and behaviors in 2021. The results showed that when considered within the context of school closures, which was affected by the COVID-19 pandemic, the lower-income household groups were more useful predictors of smartphone usage and parental depression compared to the higher-income household groups during school curriculum modification periods. In addition to lower-income, children’s psychiatric treatment history predicted the increased children’s problematic behaviors and parental depression. However, the scores of sleep problems and TV usage did not increase.
In the study, the lower-income household groups in 2020 were more predictive of smartphone usage and parental depression in 2021 compared to the higher income household group. The detrimental effects of COVID-19 are more harmful to low-income families, particularly their children. Given that elementary schoolchildren are not mature enough to effectively moderate behavior on their own, they might be less able to control their smartphone usage.35 Additionally, due to the COVID-19-related online education requirements, their smartphone use may have increased. Many students may become overly reliant on smartphones, even if their parents supervised their usage.
For a low-income household, because the parent job could require them to work on-site, parents might have fewer opportunities to work from home and stay with their children. And the detrimental economic effect of COVID-19 has made it more challenging to earn a living.35 These all contribute to possibly an increase in the time they have to put in for work to maintain a similar level of income generated before the pandemic. That is, in low-income households, parents may not have enough time to manage their children’s smartphone use. It could lead to an increased risk of smartphone addiction among low-income children.
These results are consistent with the results of previous studies showing that the low-income class was vulnerable to media overuse, sleep problems, and problematic behavior.15253436 Family income, not only parental wellbeing, but access to an abundant resource of structured education and activity, is an important factor in establishing and maintaining a family's effective coping strategy.37 However, how income affects other variables during COVID-19 needs to be investigated in detail through additional research.
In addition to lower-income households, the study showed that children’s psychiatric treatment history predicted an increase in children’s problematic behaviors and parental depression. It was found that the children groups with a history of prior psychiatric treatment for problem behavioral problems had a greater vulnerability to problem behaviors and parental depression.38 Accordingly, investment of resources will be required not only in the low-income group but in the group of children who received previous psychiatric treatment. Researchers have also found that socioeconomic status may be associated with depression among children and adolescents, even during the COVID-19 pandemic.3940
Strengths of the present study include the repeated assessment measures on the same group in South Korea during COVID-19. It was possible to check which predictors influence media use and children’s behavior. Through this, it was possible to examine the difference in resilience levels in other population groups emerging from the sample group. Like how low-income or previous psychiatric treatment history groups have a greater vulnerability to negative influences. However, this study has the following limitations. First, although it is a longitudinal study, it could not be compared with the baseline of the sample before the pandemic. Second, selection bias could influence the results as the data consisted of voluntary participants who received incentives for their participation. Third, since the income range was divided into certain sections based on self-report measures, there may be a difference in whether or not they are eligible for basic benefits that require government subsidies. Fourth, there was no significant observation found between hybrid and full in-person classes using Mann-Whitney analysis in 2021. These results were thought to be due to the large difference in the number of subjects. The full in-person class has 15 students and the hybrid school group has 171 students.
In summary, this study provides evidence that the COVID-19 pandemic during a year’s review led to the increase in screen time but problem behaviors of children have decreased compared to the initial period generally. Income level was a significant predictor, and it was found that screen time and problem behavior increased specifically in the low-income group. Therefore, it is necessary to continue monitoring the mental health of vulnerable groups and ensure that social support is continuously provided, to assist the primary caregiver.
Go to :
 XML Download
XML Download