

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Historically low incidence rates of viral respiratory tract infections were observed worldwide following the coronavirus disease 2019 (COVID-19) pandemic.12 South Korea also experienced minimal viral respiratory tract infections after the introduction of nonpharmaceutical interventions (NPIs) to mitigate the COVID-19 pandemic.345 Two years into the COVID-19 pandemic, public health measures were eased as mass COVID-19 vaccination has been implemented in South Korea since late 2021. Although restrictions on gathering sizes and mandated mask use were maintained, the number of COVID-19 cases increased sharply due to the emergence of the omicron variant as well as general fatigue regarding prevention strategies.67
Following a relaxation of NPIs, human parainfluenza virus type 3 (PIV3) circulation increased in July 2021, and a respiratory syncytial virus (RSV) B outbreak followed in November. There are increasing concerns that COVID-19 may modify the epidemiological and clinical features of common respiratory viruses.8 The decreased prevalence of respiratory viral infections in the past two years may have affected virus–virus interactions regarding airway niches and may have led to the loss of natural immunity in children.9 Investigations of COVID-19-related changes in the characteristics of respiratory viral infections would help understand the nature and pathogenesis of such viruses. These investigations may also play a role in reducing the respiratory viral infection disease burden in children and guide clinical and public health decision-making in future outbreaks.
Herein, we investigated the epidemiologic and clinical features of PIV3 and RSV B infections in Korean children and compared them before and during the COVID-19 pandemic.
METHODS
Study design
This multicenter retrospective study was performed in four hospitals in South Korea between January 2018 and January 2022. The hospitals are located in four different regions: Seoul National University Children’s Hospital in Seoul (SNUCH), Chungbuk National University Hospital (CNUH) in Cheongju, Pusan National University Hospital (PNUH) in Busan, and Jeju National University Hospital (JNUH) in Jeju.
Subjects
Eligible children were 18 years of age or younger and infected with PIV3 or RSV from January 2018 to January 2022. Nasopharyngeal swab or aspiration samples were obtained for viral detection from those who visited the hospital with fever or acute respiratory symptoms as a component of standard patient care. Respiratory viruses, including PIV3, RSV A, and RSV B, were detected with commercial multiplex reverse transcriptase polymerase chain reaction (RT-PCR) kits: Anyplex™ II RV16 Detection (Seegene Inc., Seoul, Korea) in SNUCH and CNUH, Real-Q RV Detection Kit (BioSewoom Inc., Seoul, Korea) in JNUH, and AdvanSure™ RV-plus real-time (LG Life Science, Seoul, Korea) in PNUH. During the COVID-19 period, febrile patients with respiratory symptoms needed to be tested for COVID-19 prior to seeing a doctor and hospital admission. The monthly numbers of samples positive for PIV3, RSV A, and RSV B were collected from each hospital. When samples from a single person were repeatedly positive for the same virus within three months, only the initial episode was included in the analysis. As the first COVID-19 case was detected in South Korea in January 2020, the two-year period prior to January 2020 was considered ‘before the COVID-19 pandemic,’ and the subsequent two-year period was considered ‘during the COVID-19 pandemic.’
Clinical analysis
Electronic medical record reviews were performed for patients that tested positive for PIV3 and RSV B. Age, sex, date of sample collection, clinical diagnosis, hospitalization, and need for respiratory support were retrospectively collected. Cases were classified as either upper respiratory tract infection (URTI) or lower respiratory tract infection (LRTI). URTI included rhinitis, pharyngitis, tonsillitis, acute otitis media, or croup. Pneumonia, bronchiolitis, and bronchitis were defined as LRTIs. Patients with any of the following underlying medical conditions upon clinical analysis were excluded: primary immune deficiency disease, immunocompromised condition, chronic respiratory disease, chronic cardiac disease, chronic kidney disease, neuromuscular disease, solid organ transplantation, or hematopoietic stem cell transplantation. Since respiratory samples were obtained from only hospitalized children in JNUH, they were excluded when calculating the hospitalization rate.
Statistical analysis
We compared changes in the demographic and clinical characteristics of PIV3 and RSV B infection patients before and during the COVID-19 pandemic. We defined the onset of an epidemic as the time when the viruses first appeared and the end of an epidemic as the time when no case had occurred for a month at each hospital. For RSV B cases, comparisons were performed among the 2017/2018, 2019/2020, and 2021/2022 seasons when RSV B predominated. Of note, RSV B cases in 2017 were not included in the 2017/2018 season because the start of the study period was January 2018, and there were sufficient cases of RSV B in 2018 for analysis. Patients were divided into four age groups: < 3 months of age, 3 to 23 months of age, 24 to 59 months of age, and ≥ 5 years of age. Pearson’s χ2 test and Fisher’s exact test were used to compare categorical variables. The Kruskal-Wallis test was used for nonparametric analysis. Post hoc pairwise comparisons were performed with Bonferroni’s method. All tests were two-sided, and a P value of < 0.05 was considered statistically significant. We performed statistical analyses using R version 4.1.3 (R Foundation, Vienna, Austria).
RESULTS
A total of 652 patients tested positive for PIV3: 216 in 2018, 260 in 2019, 3 in 2020, 167 in 2021, and 6 in January 2022. For RSV B, 169 children were infected in 2017/2018, 69 in 2018/2019, 274 in 2019/2020, zero in 2020/2021, and 115 in 2021/2022. RSV A mainly circulated in the 2018/2019 and 2019/2020 seasons (453 and 195 cases, respectively). The median age of PIV3 cases was 15.0 (interquartile range [IQR], 8.0–25.0) months and that of RSV B cases was 4.0 (IQR, 1.0–19.0) months during the study period.
Seasonality of PIV3 and RSV B
PIV3 mostly circulated from late spring until early autumn, with peaks in May during the pre-COVID-19 period (2018–2019) (Fig. 1). Ninety-three percent of PIV3 cases were detected from April to August in 2018, and 92.3% were detected in 2019. Only two PIV3 cases were detected from December 2019 to June 2021, during the COVID-19 pandemic. PIV3 returned in July 2021, and the case number peaked in November 2021 and dropped in January 2022. Ninety-one percent of the 2021 epidemic cases were detected from September to December; however, 5.2% were detected from April to August.
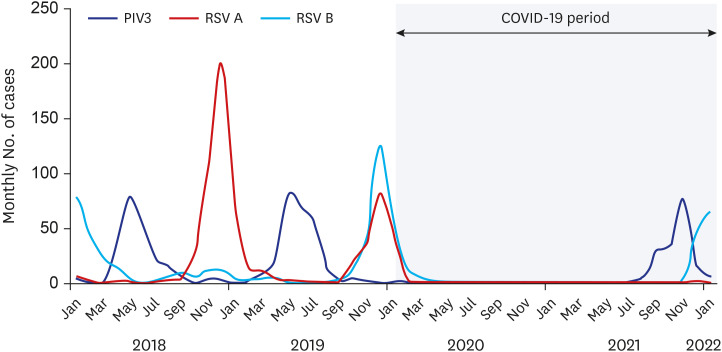
Fig. 1
Monthly number of children with human PIV3 and RSV infection before and during the COVID-19 pandemic (January 2018–January 2022). The light blue shaded area indicates COVID-19 period in South Korea.
PIV3 = parainfluenza virus type 3, RSV = respiratory syncytial virus, COVID-19 = coronavirus disease 2019.
![]()
For RSV infection, the predominant strains shifted yearly before the COVID-19 pandemic, with RSV A predominating in 2018/2019, and RSV B predominating in 2017/2018 and 2021/2022 (Fig. 1). In 2019/2020, the two strains were prevalent in similar numbers, but RSV B was relatively dominant. No RSV cases were reported in 2020/2021. An RSV B epidemic occurred from September to April, and the circulation peaked in December in 2017/2018 and 2019/2020. In 2021/2022, RSV B re-emerged in late November, with the number of cases continuing through February 2022. RSV A has rarely been detected since March 2020.
Epidemic patterns by geographic area
Epidemic patterns of PIV3 infection differed slightly by region (Supplementary Fig. 1). In 2018 and 2019, PIV3 started to circulate among the regions simultaneously and gradually ended at a similar time in all four regions. In 2021, the first PIV3 activity was captured in Busan in July, with subsequent spread across the country. The peak case number in Busan occurred in September, and that in Seoul followed in November, with a relatively high number. For RSV A and RSV B, there were minimal differences in the onset times and peaks of the epidemics among the four regions.
Demographics
The demographics of children with PIV3 infection by year and the changes before and during the COVID-19 pandemic are presented in Table 1. The median age of PIV3 patients in 2021 was 21.5 months, which was markedly older than those in 2018 (13.0 months) and 2019 (14.0 months) (P < 0.001). There was also a significant difference in the age group distributions before and during the COVID-19 pandemic (P < 0.001). Prior to the emergence of COVID-19, children aged 3–23 months were predominantly affected by PIV3 (63.9% in 2018 and 67.3% in 2019), while only 16.0–16.7% of cases occurred in those aged 24–59 months. In 2021, children aged 24–59 months accounted for 43.9% of PIV3 infections; nonetheless, children 3–23 months were most commonly affected (45.9%).
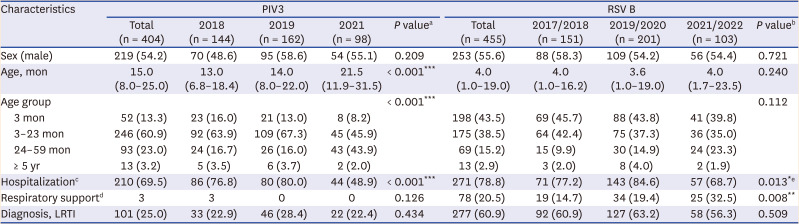
Table 1
Demographics and clinical characteristics in children with PIV3 and RSV B infection (January 2018–January 2022)
Values are presented as number (%) or median (interquartile range).
PIV3 = parainfluenza virus type 3, RSV = respiratory syncytial virus, LRTI = lower respiratory tract infection, COVID-19 = coronavirus disease 2019.
a
P value indicates the comparison among 2018, 2019, and 2021.
b
P value indicates the comparison among 2017/2018, 2019/2020, 2021/2022 season when RSV subtype B was dominant.
cHospitalization rates were analyzed among the patients in Chungbuk National University Hospital, Pusan National University Hospita, Seoul National University Children’s Hospital. A test for COVID-19 was mandated prior to hospital admission during the COVID-19 pandemic.
dA requirement of respiratory support was analyzed among children admitted to hospital.
ePost hoc analysis revealed a significant difference between 2019/2020 and 2021/2022 season.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
For RSV B infection, the median ages of patients infected with RSV B were 4.0 months in 2017/2018, 3.6 months in 2019/2020, and 4.0 months in 2021/2022 (Table 1). There were no significant differences in the median ages or age group distributions among the three seasons. The male to female ratios were 1.12:1 for PIV3 and 1.17:1 for RSV B patients, which were comparable throughout the study period for both viral infections.
Clinical characteristics
The clinical features of PIV3 and RSV B infections are shown in Table 1. Before the COVID-19 pandemic, approximately 80% of children with PIV3 were hospitalized; however, less than half were admitted to the hospital in 2021 (P < 0.001). Among 314 hospitalized children infected with PIV3, only three in 2018 needed respiratory support. Twenty-five percent of PIV3 cases were diagnosed with LRTI during the study period. The proportion of LRTI as a clinical diagnosis was not significantly different among the three epidemics (P = 0.434).
There was no significant difference in the proportion of LRTI among the three RSV B seasons (P = 0.509). Children with RSV B infection had lower hospitalization rates in 2021/2022 (68.7%) than in 2019/2020 (84.6%, P = 0.006), but the rate was not substantially different from that in 2017/2018 (77.2%, P = 0.273). Among hospitalized children with RSV B infection, 32.5% required respiratory support in the 2021/2022 season, while 14.7% in 2017/2018 and 19.4% in 2019/2022 required respiratory support (P = 0.008). When the proportion of patients requiring respiratory support was analyzed by age group, infants aged 3 to 24 months had a higher rate of respiratory assistance in 2021/2022 (19.2%) than in previous seasons (1.8% in 2017/2018 and 6.0% in 2019/2020, P = 0.012; Supplementary Table 1).
DISCUSSION
Resurgences of PIV3 and RSV B infections in Korean children were observed after an absence of these viruses for more than one year. Peak PIV3 circulation was delayed by six months, and the RSV epidemic was delayed by two months compared to those in the recent pre-COVID-19 period. This study also demonstrated a modified age distribution in PIV3 patients and reduced hospitalization rates for both PIV3 and RSV B infections during the COVID-19 period.
Following the initiation of mass COVID-19 vaccination in March 2021, COVID-19 mitigation practices such as physical distancing, home isolation, and cessation of global travel have become less stringent in South Korea. Changes in public perceptions and fatigue regarding the response to the ongoing COVID-19 pandemic may have accelerated the relaxation of public health measures as well. In particular, the operations of daycare centers and schools fully resumed in South Korea in April 2021.10
Considering the usual epidemic pattern of PIV3, which is predominant from late spring to summer,1112 the 2021 PIV3 outbreak was unusual and unpredictable. While there has been an increasing number of studies on RSV resurgence,1314 little has been reported about the epidemiologic changes in PIV during the COVID-19 pandemic.15 There could be several plausible explanations for this interseasonal rebound. First, a relaxation of NPIs starting in mid-2021 coincided with the resurgences of pediatric PIV3 and RSV infections as well as COVID-19 infection. Multiple factors, including lifted travel restrictions, reopening of educational institutions, and the resumption of socioeconomic activities, may have triggered this unusual epidemic. Large outbreaks of seasonal viruses, such as RSV and influenza, after the COVID-19 pandemic were predicted in a modeling study in 2020.8 Indeed, a rebound of common respiratory viruses, including RSV and rhinovirus, was reported as sanitary restrictions were lifted.1617 Second, seasonal respiratory viruses were suppressed by COVID-19 containment measures starting in March 2020. Children who were not exposed to RSV and PIV3 infection in 2020–2021, making them more susceptible to viruses from internal or external sources, could have rapidly transmitted the viruses to each other, playing a role in large outbreaks. Last, this interseasonal rebound could be attributed to the emergence of new viral genetic lineage strains. A preliminary report recently revealed that the PIV3 strain detected in 2021 was genetically distant from previously detected strains within subcluster C.18
Another noteworthy finding is that the median age of PIV3 patients increased, and more children aged 24–59 months were responsible for the 2021 PIV3 epidemic. PIV3 and RSV are leading causes of hospitalization for respiratory tract infections in healthy infants and young children.19 Most children become infected with PIV by the age of two years. However, infants born after the emergence of COVID-19 have unexperienced many respiratory viruses since birth, and preschoolers may not have substantial immunity against PIV or RSV due to a lack of previous exposure. These virus-naïve children who started attending daycare likely became the main contributors to the marked resurgences. A recent study also showed that the age of children with community-acquired pneumonia was higher during the NPI period than before.20 Considering that the clinical severity of PIV infection did not vary with age,19 it is understandable that the proportion of LRTIs and the need for respiratory support did not significantly change in 2021. However, the hospitalization rate decreased in the 2021 PIV3 epidemic. After the emergence of COVID-19, patients with fever or respiratory symptoms were screened for COVID-19 before entering the hospital, and children and caregivers needed COVID-19 testing for hospital admission during the COVID-19 period. Taking these factors into account, physicians and parents may have decided to minimize the hospitalization of children to reduce exposure to COVID-19 and the healthcare burden. It is also possible that increased patient age may have weakened the overall severity of PIV3 infection irrespective of the diagnosis or respiratory compromise, given the lower severity of respiratory viral infections in older children.21
RSV also showed a temporal shift. This is in accordance with previous findings17222324 that described shifts in RSV epidemics after COVID-19 in many countries. Of note, RSV A was rarely detected after January 2020 in this study. In light of the annual differences in circulating RSV strains in Korea, RSV A may return in the 2022/2023 season. Earlier studies on pediatric RSV infection in the COVID-19 era showed that the median age increased to 17–18.4 months, which was higher than the median age of 6–8.1 months in the pre-COVID-19 era.16192225 However, the median age of RSV B patients in our study was approximately four months and did not differ during the study period. Because of the nature of RSV, manifesting as acute bronchiolitis in young infants, younger children with respiratory difficulties were more likely to visit a hospital and undergo testing than older children. The need for respiratory support significantly increased during the 2021/2022 RSV outbreak, despite an unchanged age distribution and diagnosis. This finding reflects similar results reported elsewhere.1622 Expanded cohort of children having incomplete immunity against RSV may have resulted in a high proportion of primary infections, leading to a more severe disease course than reinfection. This is supported by the findings that children aged 3–24 months had slightly different characteristics than those in previous seasons, as shown in Supplementary Table 1. The relative severity appears to have increased during the COVID-19 period because children with mild cases did not visit a hospital after testing negative for COVID-19 by PCR.
In the present study, PIV3 showed different epidemiologic patterns by region, whereas RSV did not. These results are in contrast with previous findings of other studies that showed that RSV peaked later with increasing latitude.1226 Possible mechanisms include geographic and meteorological conditions, virus-specific factors, host immunity, and population movement during the NPI period. Further work is required to confirm our results and understand the epidemic dynamics of PIV resulting from interactions between virus survival, transmissibility, latitudinal differences, and climate factors.
This study has several limitations. First, due to the retrospective study design, clinical information, such as diagnosis, could be misclassified. Some cases may have been missing because each hospital implemented various testing policies and management practices for febrile patients, particularly during the COVID-19 period. Second, we limited the inclusion of patients to those with infections detected by PCR. Moderate-to-critically ill patients requiring respiratory assistance who were more likely to receive PCR testing may have accounted for a relatively high proportion. It is also possible that cases diagnosed with only the RSV antigen test without PCR testing were missed. There might be slight differences in the sensitivity and specificity because three different PCR kits were used. Third, information for patients coinfected with COVID-19 was not available since uncomplicated patients who tested positive for COVID-19 were treated at home or in a residential treatment center without further viral examination.27 Additionally, we did not collect information about other viral coinfections. However, the chance of coinfection with a virus other than COVID-19 seemed to be minimal since a markedly low incidence of respiratory viral infection was observed during the COVID-19 period. Despite these limitations, this is the first in-depth study of the epidemiological and clinical profiles of PIV3 and RSV B infection in children from four medical institutions distributed nationwide during the COVID-19 period.
In conclusion, in this multicenter study, we found that the epidemiologic characteristics of PIV3 and RSV B changed during the COVID-19 period. COVID-19 infection itself and NPIs may have directly or indirectly affected the nature of non-COVID-19 respiratory virus infections. Once sanitary restrictions are fully lifted, a return of seasonal respiratory viruses, including influenza virus, is expected. Clinicians should prepare for altered epidemiologic and/or clinical features among respiratory pathogens, and healthcare practices and policies, such as the timing of passive RSV immunization, need to be re-evaluated.
 XML Download
XML Download