

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since late 2019, coronavirus disease 2019 (COVID-19) infection has continued to spread worldwide, rendering an ongoing pandemic. Until May of 2022, more than 500 million have been infected worldwide, and more than 18 million have been infected in South Korea. Compared to previous variants, the omicron variant has evaded and transmitted the human immune system, thereby infecting many populations within South Korea.123
It is known that these persistent symptoms could remain as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection through the COVID-19 pandemic over the past two years.4567 Previous studies on long-term sequelae after illness by other coronavirus type infections—SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV)—have been reported in the literature.89 However, the consensus on the definition and criteria for these sequelae has not been established. The World Health Organization (WHO) defines “Long COVID” as the case in which symptoms persist for greater than two months; the Centers for Disease Control and Prevention (CDC) defines it as symptoms even after four weeks following acute disease, whilst the European Society of Clinical Microbiology and Infectious Disease (ESCMID) indicates symptoms even after 12 weeks post-infection.41011 The ESCMID established a working definition for the purpose of categorization as follows: 1) symptoms persisting for 12 weeks after COVID-19 diagnosis were defined as “Long COVID”, whereas 2) those persisting between 4 to 12 weeks were defined as “Post-acute COVID”.2
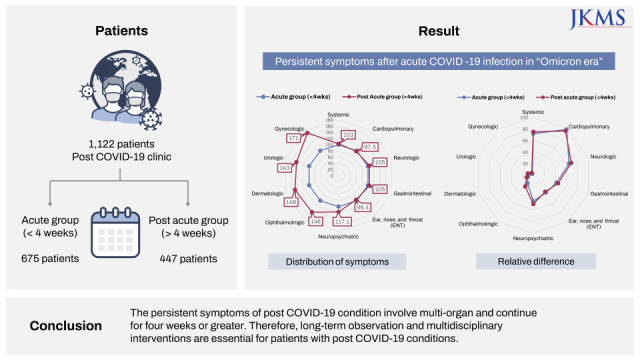
The persistent symptoms after COVID-19 infection have also been reported in the literature.121314 The clinical manifestation differs according to corresponding variants, and therefore the sequelae are also expected to be different.1 There are few reports on “Post COVID-19 Conditions” of the omicron variant. The prevalence of the omicron variant in South Korea dates back to its onset in November of 2021. Thereafter it was considered the most dominant species in February of 2022, prolonging and contributing to the unprecedented magnitude of the current pandemic. Myongji Hospital first opened the “Post COVID-19 Clinic” in South Korea. The center treated 1,122 patients presenting with post COVID-19 conditions from March 21 through April 22. Based on the data from our “Post COVID-19 Clinic”, we aim to compare the clinical characteristics and presenting symptoms of the acute COVID phase (< 4 weeks since the onset of COVID-19 infection) and that of the post-acute COVID phase (> 4 weeks since the onset of COVID-19 condition) in order to examine which factors may have plausible effects on the number of persistent symptoms and their respective categories.
METHODS
Study participants and stratified groups
We retrospectively collected data from 1,164 patients registered at the “Post COVID-19 Clinic” of Myongji Hospital in Goyang, Republic of Korea, from March 21, 2022, to April 22, 2022. All participants provided detailed medical history, including the date of diagnosis of the COVID-19 infection, physical examination, and a questionnaire assessing their symptoms. The hospital anxiety and depression scale (HADS) were used to assess levels of anxiety and depression. Fatigue severity scale (FSS) was used to assess fatigue. We excluded 42 participants due to the following reasons: 1) uncertainty regarding the date of their diagnosis, and 2) refusal to answer the questionnaire.
We classified the remaining 1,122 participants into two groups according to duration of symptoms from the time of diagnosis of COVID-19 up until the date of their clinic visit. In accordance with the ESCMID guidelines, we classified the participants by dividing 4 weeks into two periods. If the clinic visit was within 4 weeks since diagnosis the participant was classified into “acute group,” while those who visited the clinic following a period greater than 4 weeks were classified into “post-acute group.”
Questionnaire regarding symptoms after COVID-19 infection
We acquired the data on persistent symptomatology after COVID-19 infection using a questionnaire. Participants who visited “Post COVID-19 Clinic” answered the questionnaire which was provided via an SNS messenger system. Our questionnaire includes 33 detailed inquiries pertaining to 10 categories of symptoms. Multiple responses were allowed per question. Cardiopulmonary symptoms category included coughing, productive sputum, shortness of breath, palpitation, chest pain, and edema. Neurologic symptoms category included headache, dizziness, sleep disturbance, memory impairment, and tingling. General symptoms category included fatigue, generalized weakness, and weight loss. Gastrointestinal symptoms category included abdominal discomfort, heartburn, abdominal pain, diarrhea, and nausea or vomiting. Neuropsychiatric symptoms category included decreased attention, depression, and anxiety. Ear, nose, and throat symptoms category included hyposmia and hypogeusia. Ophthalmologic symptoms category included blurred vision and eye irritation. Dermatologic symptoms category included hair loss and skin rash. Gynecologic symptoms category included dysmenorrhea and vaginal bleeding. Urologic symptoms category included bladder-related symptoms, foamy urine, and sexual dysfunction.
Assessment of depression and anxiety
Anxiety and depression symptoms were assessed using the seven-item sub-scales of the hospital anxiety and depression scale (HADS-anxiety, HADS-depression).15 The HADS is designed to minimize reporting of somatic symptoms of anxiety and depression in medically ill people and is considered to have both sensitivity and specificity for the HADS-anxiety and HADS-depression of approximately 0.80 when using a cut-off score of > 7 from a total possible score of 21.16 Each item of the HADS has a minimum score of 0 and a maximum score of 3. The seven-item scores are summed to the final HADS-anxiety and HADS-depression scores.
Assessment of fatigue
Fatigue is defined as a sense of physical tiredness and lack of energy which are distinguished from sadness or weakness.17 The FSS, developed by Krupp et al.,17 is the most commonly used self-report questionnaire to measure fatigue.18 It consists of 9 items scored on a Likert scale from 1 to 7. The mean of all scores is considered to be the final score, and a higher score denotes a higher level of fatigue.
Statistical analysis
To evaluate the differences in demographics, we performed an analysis of variance for continuous variables and a χ2 test for categorical variables. The prevalence of symptoms of post COVID-19 conditions was compared by χ2 test. Linear regression analysis was performed to predict the number of symptoms and categories. A P value ≤ 0.05 indicates a statistical significance. All analyses were performed using SPSS software (SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Myongji Hospital and the study was performed in accordance with the approved protocols and guidelines (MJH-2022-05-009). The requirement for participants’ informed consent was waived by the IRB of Myongji Hospital since we used retrospective de-identified data collected during health exam visits.
RESULTS
Baseline characteristics of participants
Among 1,122 patients, 675 were classified into the acute group and 447 were classified into the post-acute group (Table 1). Overall, the post-acute group was older than the acute group (51.4 ± 15.3 vs. 50.9 ± 15.9, P = 0.001) and the duration from the diagnosis of COVID-19 to the clinic visit was 26.4 ± 45.2 days. Overall, the number of symptom categories was 4.0 ± 2.1, and the number of symptoms was 7.7 ± 4.9. The number of symptom categories was higher in the post-acute group than in the acute group (4.2 ± 2.2 vs. 3.9 ± 2.0, P = 0.001). The number of symptoms was higher in the post-acute group than in the acute group (8.1 ± 5.2 vs.7.6 ± 4.6, P = 0.007). The rate of hospitalization (P = 0.292) and the prevalence of pneumonia (P = 0.382) was not significantly different between the two groups. The mean score of FSS was 4.1 ± 1.8, the mean score of HADS-Anxiety was 6.2 ± 4.8, and HADS-Depression was 4.1 ± 1.8. The two groups were not different in terms of HADS and FSS.
Table 1
Demographic data
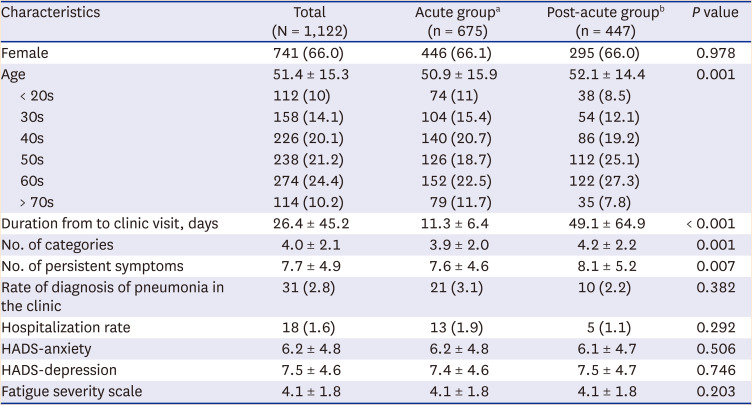
Values are presented as number (%) or mean ± standard deviation.
HADS = hospital anxiety and depression scale, COVID-19 = coronavirus disease 2019.
aAcute group: presented to the clinic within 4 weeks since COVID-19 diagnosis.
bPost-acute group: presented to the clinic at greater than 4 weeks since COVID-19 diagnosis.
Persistent symptoms after COVID infection
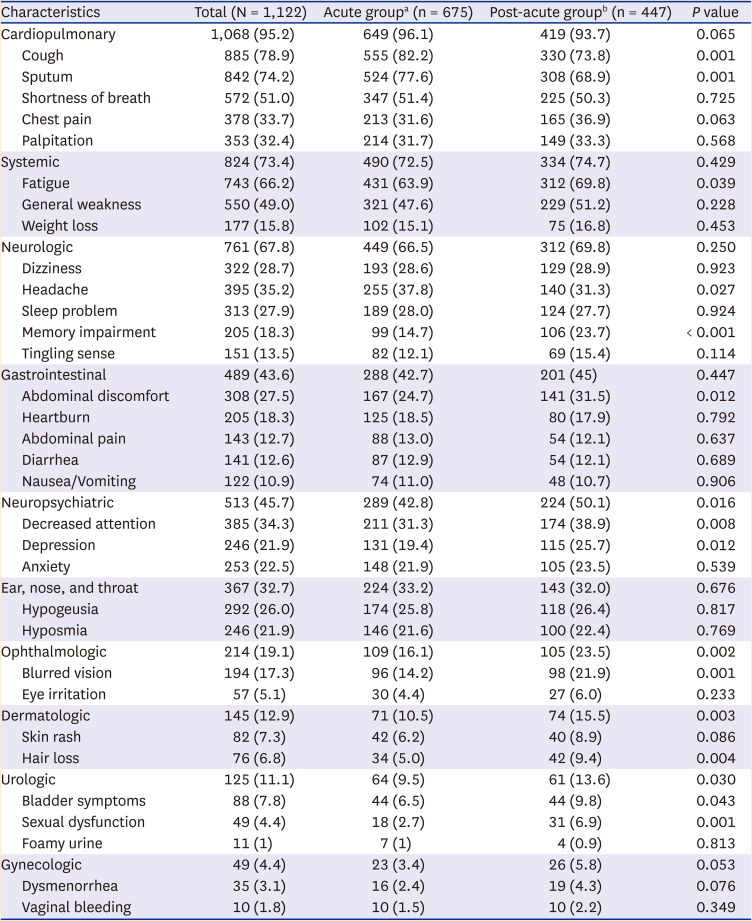
We investigated overall 24 symptoms across 10 symptom categories (Fig. 1 and Table 2). Among all symptom categories, the most common was cardiopulmonary (95.2%), followed by general (73.4%), neurologic (67.8%), and psychiatric (45.7%). Among presenting symptoms cough (78.9%) was the most common, followed by productive sputum (74.2%), fatigue (66.2%), and headache (35.2%).
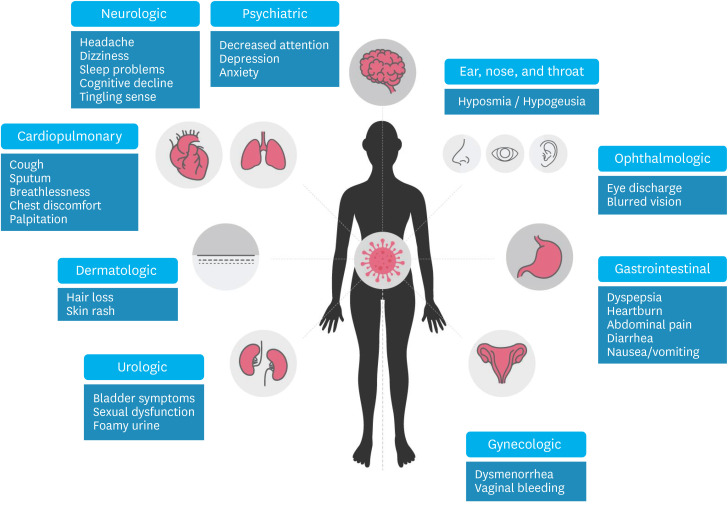
Table 2
Persistent symptoms of post COVID-19 condition
Persistent symptoms after COVID-19 infection compared between two groups
The number of symptom categories was higher in the post-acute group than in the acute group (4.2 ± 2.2 vs. 3.9 ± 2.0, P = 0.001). The number of symptoms also was higher in the post-acute group than in the acute group (8.1 ± 5.2 vs.7.6 ± 4.6, P = 0.007).
Participants in the post-acute group showed higher rate of symptoms in psychiatric (42.8% vs. 50.1%, P = 0.016), ophthalmologic (16.1% vs. 23.5%, P = 0.002), dermatologic (10.5% vs. 15.5%, P = 0.003), and urologic (11.1% vs. 13.6%, P = 0.03) categories than those in the acute group.
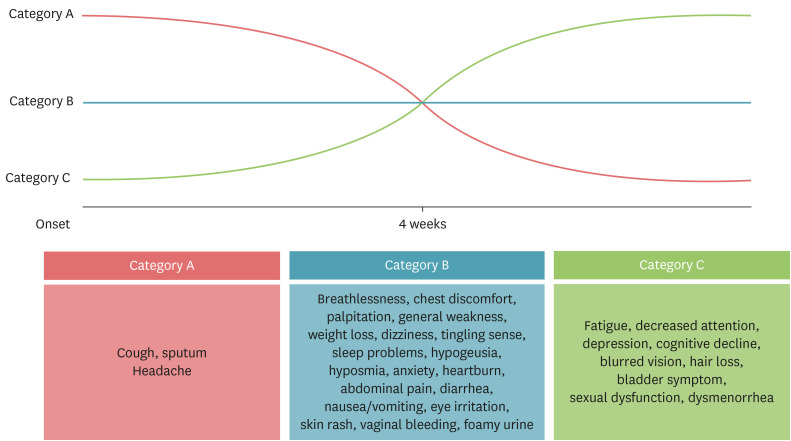
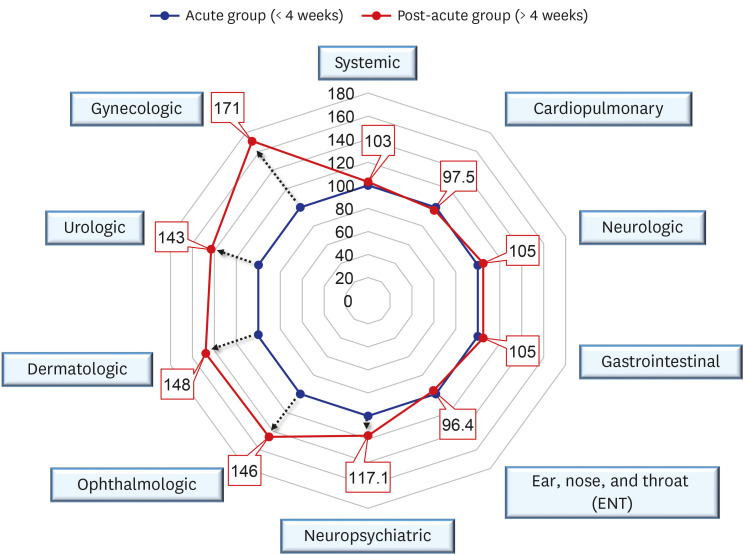
Among 32 symptoms, symptoms were classified into three categories as follows (Fig. 2): Category A (the prevalence of symptoms is higher in the acute group than in the post-acute group), Category B (the prevalence of symptoms is not different between two groups) and Category C (the prevalence of symptoms is higher in the post-acute group than in the acute group). Category A included cough, headache, and sputum. Category B included breathlessness, general weakness, chest discomfort, palpitation, dizziness, hypogeusia, hyposmia, anxiety, heartburn, weight loss, abdominal pain, diarrhea, tingling sense, nausea or vomiting, eye irritations, dysmenorrhea. Category C included fatigue, decreased attention or brain fog, depression, blurred vision, hair loss, and sexual dysfunction. When the acute group was standardized to 100 and compared with the post-acute group, the symptom category corresponding to Category C was significantly higher (Fig. 3).
Fig. 2
Three categories of persistent symptoms after acute COVID-19 infection. Category A: symptoms in which the prevalence is higher in the acute group than in the post-acute group; Category B: symptoms in which the prevalence is not significantly different between the two groups; Category C: symptoms in which the prevalence is higher in the post-acute group than in the acute group.
Multiple regression in the number of symptoms
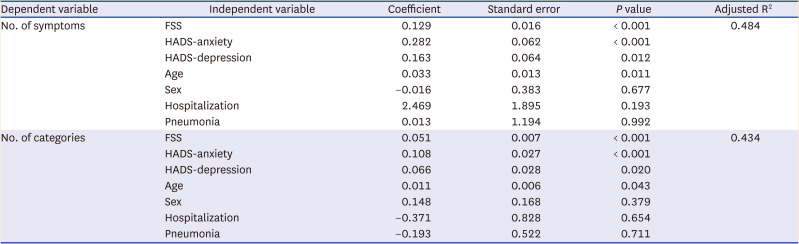
As shown in the regression model (Table 3), HADS-anxiety (B = 0.282, P < 0 .001), HADS-depression (B = 0.163, P < 0.064), FSS (B = 0.129, P < 0.001), and age (B = 0.033, P = 0.011) were all associated with the number of symptoms (R2 = 0.484). In addition, HADS-anxiety (B = 0.108, P < 0.001), FSS (B = 0.051, P < 0.001), HADS-depression (B = 0.066, P = 0.020), and age (B = 0.011, P = 0.043) were all associated with the number of symptom categories (R2 = 0.434).
Table 3
Multiple regression using number of symptoms and their categories as the dependent variable for participants in the post-acute group
DISCUSSION
In this study, we examined whether the number and categories of persistent symptoms were different according to their duration following an acute infection among 1,122 patients who responded to a questionnaire pertaining to persistent symptoms after COVID-19 infection, HADS and FSS. We observed that the number of symptoms and their categories were higher in the post-acute group than in the acute group. The prevalence of some symptoms such as fatigue, decreased attention, depression, blurred vision, hair loss, and sexual dysfunction were higher in the post-acute group than in the acute group. HADS-Anxiety, HADS-Depression, FSS and age were associated with the number of symptoms and their categories and anxiety was the most correlated factor. Our findings suggest that the persistent symptoms of post COVID-19 condition involved multi-organ systems with a duration of four weeks or greater which required long-term observation and multidisciplinary intervention.
Our results are not different from previous studies on the long-term effects of COVID-19 infection before the emergence of the omicron variant. In 2020, the CDC COVID-19 response team reported 270 infected patients after two to three weeks from the time of diagnosis.19 Herein, 175 patients (65%) fully recovered to baseline health status and the median value of the recovery period was 7 days; however, 95 patients (35%) had subjective complaints of persistent symptoms. Persistent symptoms were reported as follows: cough (43%), fatigue (35%), and dyspnea (29%).19 Goërtz et al.12 followed 2,113 patients for three months during which time 85.3% of women reported symptoms of fatigue, shortness of breath, and headache. A study by Jennings et al.,13 assessed patients during the acute period after infection, similar to our study, and reported fatigue (43%), shortness of breath (31%), cough (26%), insomnia (36%), and anosmia (11%) as persistent symptoms. The most common symptoms reported in another study were fatigue, shortness of breath, and myalgia.14 Similar to previous studies, the high incidence in women is likely to be associated with a higher incidence of autoimmune diseases among women.1214
In this study, the rate of pneumonia diagnosis rate was 2.8%, which was lower than in previous studies.1314 This is likely attributable to the fact that the omicron variant primarily causes upper respiratory tract infection, and the disease severity has decreased compared to previous variants due to the widespread implementation of COVID-19 vaccinations and spike protein mutation. Furthermore, the majority of our observed results in this study are thought to be due to the participation of home-based treatment patients with no hospitalization history.
The mechanism of persistent symptoms long after COVID-19 infection is currently not well understood. It is presumably caused by tissue damage from the SARS-CoV-2 virus binding action to human angiotensin-converting enzyme 2 which is expressed in multiple organs including lungs, brain, heart, gastrointestinal tract, liver, pancreas, kidneys, and blood vessels. Viral infection can bind to various organs and cause direct damage which can lead to persistent symptoms.2021 An immune response like an autoimmune response caused by a viral infection can also cause persistent symptoms. Although the role and immune mechanism of T cells in SARS-CoV-2 infection are not fully known, it is known that immune system dysregulation may occur, such as an autoimmune response.2223 Moreover, there are hypotheses on the underlying culprits for persistent symptoms including pathophysiologic manifestations such as hidden viral reservoirs and non-infectious viral fragments, COVID-19 associated immune exhaustion, abnormal immunometabolism, mitochondrial dysfunction, altered microbiome, and imbalance in the renin-angiotensin system.24
The symptom patterns were different across the two groups. In acute group, respiratory symptoms associated with viral infections were dominant, and this may be associated with an inflammatory response caused by residual levels of the virus or their fragments. As the virus level subsides respiratory symptoms improve. Other symptoms are thought to be potentially related to immune response without any significant difference as it relates to time. In the post-acute group, common symptoms were fatigue, psychiatric symptoms such as anxiety, depression, and decreased attention. Persistent symptoms after infection are affected by some psychological factors contributing to rates of infection as was the case with persistent symptoms after SARS-CoV and MERS-CoV infection.89 However, although anxiety belonged to Category B, depression and fatigue fell under Category C. Therefore, unlike anxiety, the prevalence of depression and fatigue appears to have increased as persistent symptoms continued. In the post-acute group, the prevalence of blurred vision, hair loss, and urologic and gynecologic symptoms were higher than that of the acute group. The pathogenesis of these symptoms with low prevalence involving multiple systems is unclear and thus future studies on the underlying mechanism are warranted.
WHO International Classification of Disease-10 system has approved “Post COVID-19 Condition (U-09)” for post-acute sequelae of COVID-19 since September of 2020. However, the definition of the “Post COVID-19 Condition” has not been substantiated. The sequelae are also on a continuum from the onset of the disease thereby adding to the challenge of clearly elucidating the course of ongoing disease. Based on our experience from the designated clinic for “Post COVID-19 Condition,” the demand for medical treatment arises immediately following the completion of an isolation period. It is necessary to delineate and characterize the long-term effects of COVID-19 infection that is different from the ongoing symptoms of COVID-19.
This is the first study on “Post COVID-19 Conditions” after the omicron variant breakthrough infection in South Korea, and we believe that it provides new insight into its underlying clinical manifestations during the transition period from acute infection to long COVID syndrome. Our study also presented some limitations. A prospective longitudinal cohort study design may serve to be more advantageous than the retrospective cross-sectional design. Subjective complaints of symptoms were acquired using a questionnaire with limited objective test results to support our hypothesis. Since there is a lack of consensus in defining post COVID-19 condition, all patients who presented to the clinic with varying subjective symptoms were included for data acquisition whereas patients with severe omicron variant infections were selectively excluded. Future studies are warranted to substantiate criteria and analysis of associated symptoms in depth by stratification of severity or underlying comorbidity. Although several studies have reported associations between COVID-19 vaccinations and post COVID-19 conditions, our data did not include the vaccination status.2526
In conclusion, there are varying symptoms which persist following a COVID-19 infection. As reported in our study, we observed many subjective complaints of post COVID symptoms after an omicron variant infection. In the protracted acute phase of COVID-19 infection (< 4 weeks from the infection of COVID-19), it is essential for medical management to primarily target respiratory-related symptoms whereas a multidisciplinary systems approach to clinical care is advantageous during the post-acute phase (> 4 weeks from the infection of COVID-19).
 XML Download
XML Download