

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
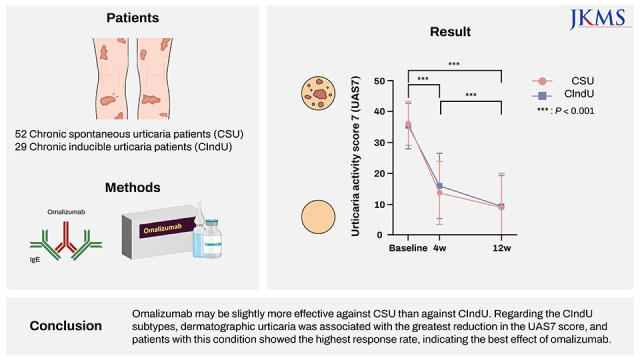
Omalizumab is a major drug for treating chronic urticaria that is not well controlled with antihistamines or cyclosporine. Extensive real-world data are available on the efficacy and safety of omalizumab in patients with chronic spontaneous urticaria (CSU).123 However, data for the drug when used for the management of chronic inducible urticaria (CIndU) are relatively insufficient.4567 Furthermore, few studies have compared the efficacy of omalizumab between CSU and CIndU.89 Therefore, this study was aimed at evaluating omalizumab’s efficacy in patients with CSU and CIndU and determining in which patients the treatment is more effective.
Go to : 
METHODS
Study participants
This study was conducted in 81 patients (age ≥ 19 years) including 52 and 29 with isolated CSU and CIndU, respectively, who were treated with 150 mg of omalizumab at least thrice every 4 weeks from January 2017 to January 2022. Patients who had both CSU and CIndU were excluded. Among the patients with CIndU, cholinergic urticaria was the most common condition (n = 13, 44.8%), followed by dermatographic urticaria (n = 9, 31.0%), cold urticaria (n = 6, 20.69%), and delayed pressure urticaria (n = 1, 3.5%).
Treatment response
Complete blood count and total immunoglobulin E (IgE) level were evaluated in all patients before the first omalizumab was administered, and Urticaria Activity Score 7 (UAS7) at baseline, week 4, and week 12 was assessed. The daily cyclosporine dose (converted to the number of 25 mg capsules) and number of antihistamine tablets administered daily (both first and second-generation antihistamines) at baseline, week 4, and week 12, were also investigated to indirectly evaluate the degree of disease control. All related data were analyzed retrospectively. Based on the UAS7 at week 12, the scores were defined as follows: 0, complete response; ≤ 6, partial response; and ≥ 7, minimal response.10 Both partial and complete responders were classified as responders.
Statistical analysis
Changes in UAS7 following omalizumab administration were examined using repeated-measure analysis of variance. In comparisons between responder and non-responder, correlations between continuous variables and relationships between categorical variables were examined using the Student’s t-test and χ2 test, respectively. Statistical significance was analyzed using SPSS software (version 26.0); P values of < 0.05 were considered significant.
Ethics statement
This study was reviewed and approved by the Institutional Review Board (IRB) of Hallym University Sacred Heart Hospital (IRB number 2022-01-001), and Seoul Asan Medical Center (IRB number 2019-0996). Informed consent was waived because of the retrospective nature of the study.
Go to :
RESULTS
Treatment response in CSU and CIndU
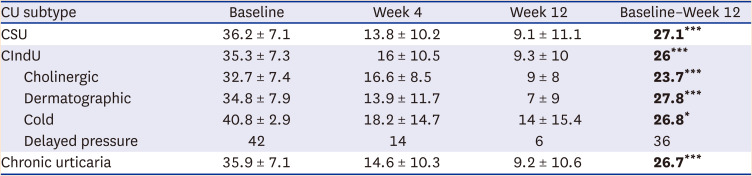
Fig. 1 and Table 1 summarize the changes in UAS7 over time in both patient groups. The baseline UAS7 was 36.2 ± 7.1 and 35.3 ± 7.3 in the CSU and CIndU groups, respectively. In the former, UAS7 decreased to 13.8 ± 10.2 and 9.1 ± 11.1 in weeks 4 and 12, respectively. The corresponding values in the CIndU group were 16 ± 10.5 and 9.3 ± 10. Therefore, the mean differences in UAS7 between baseline and week 12 in the CSU and CIndU groups were 27.2 (95% confidence interval [CI], 23.6–30.7; P < 0.0001) and 26.03 (95% CI, 21.1–31; P < 0.0001), respectively.
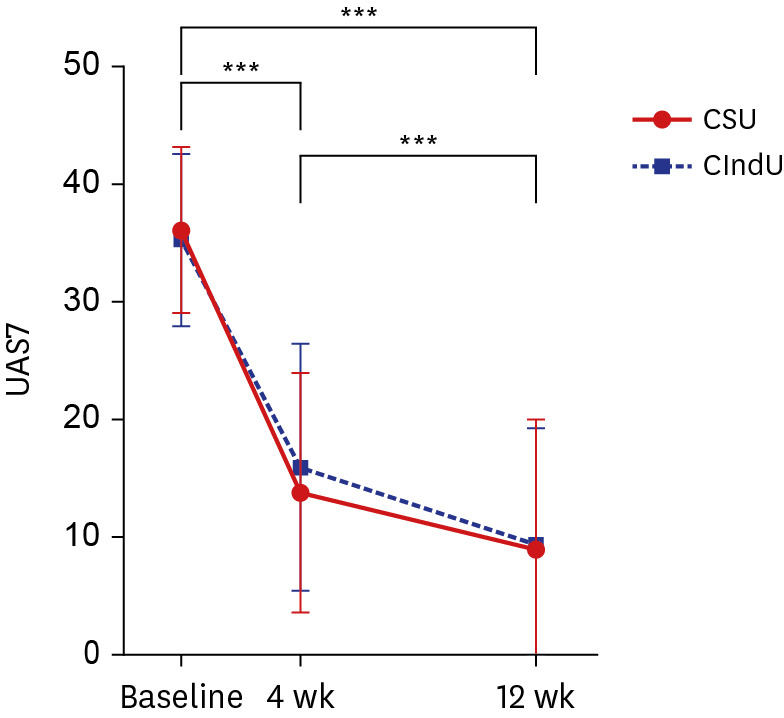 | Fig. 1Changes in UAS7 over time in patients with CSU and CIndU.UAS7 = Urticaria Activity Score 7, CSU = chronic spontaneous urticaria, CIndU = chronic inducible urticaria.
***P < 0.001.
|
Table 1
UAS7 at baseline, week 4, and week 12 in chronic urticaria (CU)
Values are presented as number (%) or mean ± standard deviation.
Statistically significant values are shown in bold.
UAS7 = Urticaria Activity Score 7, CSU = chronic spontaneous urticaria, CIndU = chronic inducible urticaria.
*P < 0.05, ***P < 0.001.
![]()
UAS7 significantly decreased over time in both groups, with a significant decrease after 4 weeks with the administration of only one omalizumab dose (P < 0.0001). This significant change continued until week 12 after two additional doses, indicating a significant decrease in UAS7 in both groups (CSU: P < 0.0001; CIndU: P < 0.001) at week 12 compared to that at week 4. Intergroup differences in UAS7 at baseline, week 4, and week 12 were not significant.
According to the definition of response, complete and partial responses were noted in 19 (36.5%) and 14 (26.9%) patients with CSU, respectively, with an overall response found in 33 patients (63.5%) (Table 2). The corresponding numbers in the CIndU group were 4 (13.8%), 14 (48.3%), and 18 (62.1%).
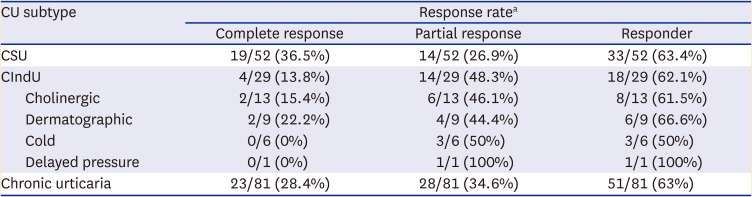
Table 2
Response rates in the CSU and CIndU groups
CSU = chronic spontaneous urticaria, CIndU = chronic inducible urticaria.
aBased on the UAS7 at week 12, the scores were defined as follows: 0, Complete response; ≤ 6, Partial response; and ≥ 7, Minimal response.
UAS7 = Urticaria Activity Score 7.
![]()
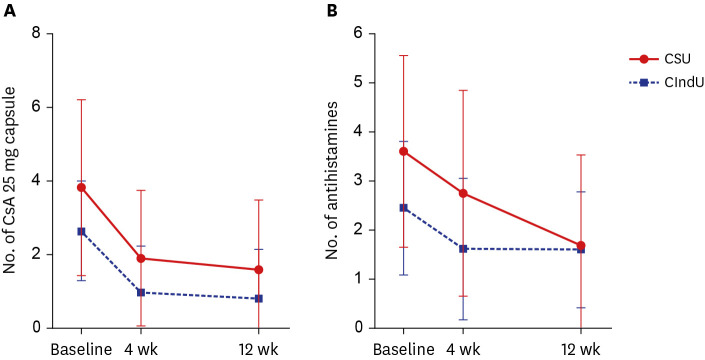
Of the 52 CSU patients, 13 were prescribed cyclosporine at baseline and 48 were prescribed antihistamine with initial omalizumab. Of the 29 CIndU patients, 6 were prescribed cyclosporine and 24 were prescribed antihistamines on the first day of omalizumab administration. In CSU patients who were prescribed cyclosporine, the number of prescribed baseline cyclosporine 25 mg capsules were 3.9 ± 5.6 and the number of prescribed baseline antihistamine tablets were 3.6 ± 3.8. In these patients, mean number of prescribed cyclosporine capsules at week 4 and week 12 was reduced to 1.9 and 1.6, respectively. Mean number of prescribed antihistamine tablets at week 4 and week 12 was reduced to 2.8 and 1.7, respectively. In CIndU patients who were prescribed cyclosporine, the number of prescribed baseline cyclosporine 25 mg capsules were 2.7 ± 1.9 and the number of prescribed baseline antihistamine tablets were 2.5 ± 1.7. In these patients, mean number of prescribed cyclosporine capsules at week 4 and week 12 was reduced to 1 and 0.8, respectively. Mean number of prescribed antihistamine tablets at week 4 and week 12 was reduced to 1.7 and 1.6, respectively.
The number of cyclosporine 25 mg capsules administered daily decreased significantly in both groups, and there was no significant intergroup difference (P = 0.898) (Fig. 2A). The number of antihistamine tablets administered daily significantly decreased in both groups, with the CSU group showing a more significant decrease (P = 0.047) (Fig. 2B).
Treatment response per CIndU subtypes
Fig. 3 summarizes the changes in the UAS7 over time for each CIndU subtype. Except for delayed pressure urticaria, which could not be statistically analyzed because only one patient with the condition was included, all subtypes were associated with a significant decrease in UAS7. Especially, cholinergic urticaria and dermatographic urticaria showed a significant decrease in UAS7 with only one omalizumab dose (P < 0.001); after 12 weeks, a more significant decrease in UAS7 was observed compared with baseline (the significance of differences in UAS7 in those with cholinergic urticaria and dermatographic urticaria is shown as a black line in Fig. 3). Cold urticaria was also associated with a significant decrease in UAS7 at both 4 (P = 0.036) and 12 weeks (P = 0.017) compared to baseline.
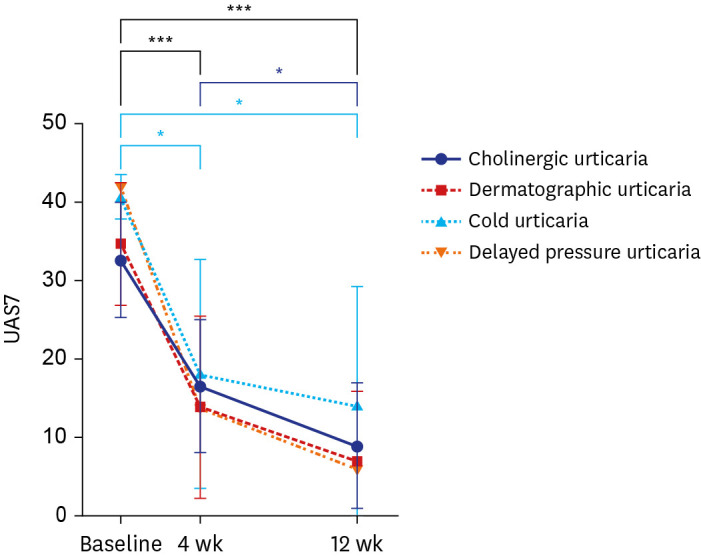
Regarding the response rates of the CIndU subtypes (Table 2), the overall response rate, the sum of complete and partial response rates, was the highest for dermatographic urticaria (66.7%), followed by cholinergic urticaria (61.5%) and cold urticaria (50%). One patient with delayed pressure urticaria showed a partial response.
Comparison between responders and non-responders
Twenty-three (28.4%) and 28 (34.6%) showed complete and partial responses, respectively; thus, 51 patients (63%) were classified as responders (Table 2) and the rest as non-responders. A comparison of the baseline characteristics between the two groups is summarized in Table 3. The duration of chronic urticaria was longer among the non-responders (142.3 ± 257.6 weeks) than responders (53.2 ± 36.7 weeks) (P = 0.025). The baseline total IgE level was significantly higher among the responders (322.7 ± 285.1 IU/mL) than non-responders (172.7 ± 204.7 IU/mL) (P = 0.039). Further, there was no intergroup difference in baseline characteristics between the CSU and CIndU groups.
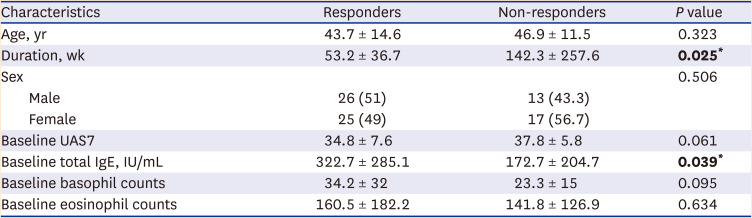
Table 3
Comparison of baseline characteristics between responders and non-responders
Values are presented as number (%) or mean ± standard deviation.
Statistically significant values are shown in bold.
UAS7 = Urticaria Activity Score 7, IgE = immunoglobulin E.
*P < 0.05.
![]()
Go to :
DISCUSSION
In this study, omalizumab treatment significantly decreased UAS7 in both the CSU and CIndU groups and reduced the numbers of cyclosporine and antihistamine tablets administered. Therefore, we reconfirmed that it was effective against both CSU and CIndU. Improved UAS7 in patients with CSU in this study corresponded to the levels in a meta-analysis of real-world data for CSU, which showed mean 25.6 points of decrease in UAS7.1 Concerning improvement in CIndU, there have not yet been any studies reporting the difference between baseline and post-treatment UAS7 in patients with CIndU.
There was no significant difference in UAS7 between the two groups; therefore, it is difficult to say that either is more responsive to treatment. However, the rate of decrease in UAS7 from baseline to week 4 and from baseline to week 12 was larger in the CSU group, indicating a faster decrease in UAS7 in the group (Fig. 1). Furthermore, the number of antihistamine tablets administered every day decreased more significantly in the CSU group, indirectly indicating that CSU symptoms could be controlled better with omalizumab.
The complete response rate was higher in the CSU group than in the CIndU group (36.5% vs. 13.8%); however, the partial response rate was higher in the latter (48.3% vs. 26.9%). Therefore, the overall response rate was only slightly higher in the CSU group (63.5% vs. 62.1%). The response rates were similar to those in a previous study (week 12: 64.7% [CIndU] and 66.7% [CSU] and increased to 78.6% (CIndU) and 84.6% (CSU) at week 24.6 These results show that response to omalizumab was slightly better in patients with CSU and continuing omalizumab treatment for 24 weeks may increase response rates in patients who were unresponsive at week 12.8
When CIndU subtypes were classified and the response rates were compared, dermatographic urticaria had the highest response (66.7%), and the greatest result for a decrease in UAS7 score from baseline to week 12 was 27.8 (P < 0.0001). Therefore, dermatographic urticaria showed the best response to omalizumab among the CIndU subtypes. In a randomized placebo-controlled trial of omalizumab in dermatographic urticaria,11 the response rate in the omalizumab 150 mg administration group was 66%. Hence, our study result was almost consistent with that of the randomized controlled study.11 Notably, there was no significant difference in efficacy between the 150 and 300 mg treatment groups, which showed a 58% response rate. Therefore, only administration of 150 mg of omalizumab can effectively treat dermatographic urticaria, which was also confirmed in our study.
Cholinergic urticaria also showed a response in 61.5% of patients, and a reduction in UAS7 score from baseline to week 12 showed a good result of 23.7 (P < 0.0001). Furthermore, when comparing the changes from week 4 to week 12, dermatographic urticaria did not show a significant difference in UAS7, while the UAS7 for cholinergic urticaria significantly decreased (P = 0.037). Regarding cold urticaria, 50% of patients showed a response, and the associated UAS7 decreased significantly at weeks 4 (P = 0.036) and 12 (P = 0.017) compared to baseline. In a patient with delayed pressure urticaria, baseline UAS7 of 42 points decreased to 6 points at week 12, confirming omalizumab’s effect.
To date, three studies have compared the effects of omalizumab per CIndU subtypes. The complete response rate was the highest for delayed pressure urticaria in one study.12 In a retrospective, real-life study,13 delayed pressure urticaria showed the highest response rate, followed by cold urticaria and cholinergic urticaria. In a study of 80 patients with CIndU,3 the best response to omalizumab was shown by solar urticaria and a relatively poor response was shown by dermatographic urticaria compared to other subtypes. Since the definitions of response were different in each study and the omalizumab dose administered was differed, it seems difficult to clearly determine which CIndU subtype is the most responsive based on the results obtained hitherto.
In comparison between responders and non-responders, the duration of chronic urticaria was longer in the non-responders (P = 0.025). Approximate mean duration of responders was 53.2 weeks, and that of non-responders was 142.3 weeks. Therefore, the duration of chronic urticaria of non-responders was approximately three times longer than that of responders. In contrast, baseline total IgE levels were significantly higher in responders (P = 0.039); therefore, patients with higher baseline total IgE levels responded better to omalizumab. This finding was consistent with those of previous studies.1415 Therefore, baseline total IgE levels should be checked in all patients with chronic urticaria in whom omalizumab administration is considered because it can be used to predict treatment response. Additionally, omalizumab can be actively recommended if total IgE levels are high in patients who do not respond well to other treatments.
This study is meaningful in that it offers the largest scale real-world data on omalizumab treatment in Korean patients with chronic urticaria, especially in that it included many patients with CIndU. Especially, it is meaningful in that it confirmed significant improvements in urticaria symptoms among Korean patients administered 150 mg omalizumab rather than 300 mg. In clinical settings, it is often difficult to prescribe 300 mg of omalizumab due to the burden of price. Therefore, it would be appropriate to prescribe 150 mg first and increase the dose to 300 mg if the response is insufficient.
This study has several limitations. First, this was a retrospective study. Secondly, when we count the number of antihistamine tablets administered daily, we did not distinguish antihistamine types. Furthermore, it did not include patients with chronic urticaria who received omalizumab 300 mg. Additionally, a relatively small number of patients with CIndU were included compared to the number of CSU patients. Other CIndU subtypes, such as solar urticaria, heat urticaria, and aquagenic urticaria, were not included. Therefore, a larger-scale prospective study with more patients and various subtypes of CIndU is required.
In summary, omalizumab 150 mg was effective against both CSU and CIndU and showed significantly improved symptoms. Although there was no significant difference in efficacy between the two groups, CSU symptoms tended to improve faster, and the number of antihistamine tablets administered daily decreased more significantly. Further, the reduction in the UAS7 between baseline and week 12 was larger in the CSU group, and the responder rate was slightly higher among CSU patients. Therefore, omalizumab may be slightly more effective against CSU. Among the CIndU subtypes, dermatographic urticaria was associated with the greatest decrease in UAS7, and showed the highest response rate, showing the best effect on omalizumab. In patients with chronic urticaria, the longer the morbidity of the disease, the less likely it would respond to omalizumab. Conversely, the higher the baseline total IgE level, the better the response to omalizumab.
Go to :
 XML Download
XML Download