

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The 2017 American College of Cardiology (ACC)/American Heart Association (AHA) guideline is advocated that antihypertensive medications achieve a target blood pressure (BP) of <130/80 mm Hg in most adults.1) New guidelines on hypertension by the European Society of Hypertension (ESH)/European Society of Cardiology (ESC) recommend that the first objective of treatment should be to lower BP to <140/90 mmHg in all patients, and provided that the treatment is well tolerated, treated BP values should then be targeted at ≤130/80 mmHg in most patients. Moreover, the diastolic blood pressure (DBP) target range of 70–79 mmHg has been recommended for all hypertensive patients.2)
Although results from previous epidemiologic studies have revealed an increased risk of cardiovascular (CV) disease in people with a DBP >75 mm Hg,3)4)5)6) the DBP threshold and target have been fundamentally based on expert opinion,1) and the results of meta or pooled analyses.7)8) Furthermore, there is inadequate evidence supporting the use of DBP as a criterion for treatment goals.
Isolated diastolic hypertension (IDH) without elevation of systolic blood pressure (SBP) has been a distinct phenotype of hypertension in its early phase, or in young adults. Nonetheless, several studies9)10)11)12)13)14)15) have presented conflicting results. Moreover, elevated DBP between treated hypertensive patients and non-treated subjects need to be considered separately. It is unclear whether DBP, while receiving antihypertensive treatment, modulates CV risk in the presence of an achieved SBP target.
This nation-wide population-based study using the Korean National Health Insurance Service (NHIS) database, covered 97% of the Korean population and included 3.2 million adults with hypertension over a wide age-range. It aimed to investigate the association between the risk of cardiovascular events and two different levels of elevated on-treatment DBPs in the presence of achieved SBPs—in which they were lowered either by the 2017 ACC/AHA (SBP <130 mmHg, DBP ≥80 mmHg) or by the Seventh Report of Joint National Committee (JNC7; SBP <140 mmHg, DBP ≥90 mmHg) definitions.
METHODS
Ethical statement
This study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (IRB No. KBSMC 2019-12-020). Informed consent was waived because an anonymised dataset was provided to the researchers by the NHIS. Participants were not involved in the design, conduct, reporting, or dissemination of this research.
Data sources
The NHIS provides mandatory health insurance for all citizens in the Republic of Korea, covering 97% of the population in the Republic of Korea.16) Adults aged ≥19 years are legally required to undergo periodic health examinations biannually, as provided by the NHIS. All diagnoses are recorded in the NHIS database using the International Classification of Diseases, Tenth Revision (ICD-10) codes. Death records, including the cause of death and date of death, were obtained from the Statistics Korea database. The details of the database are described and validated elsewhere.17)
Study population
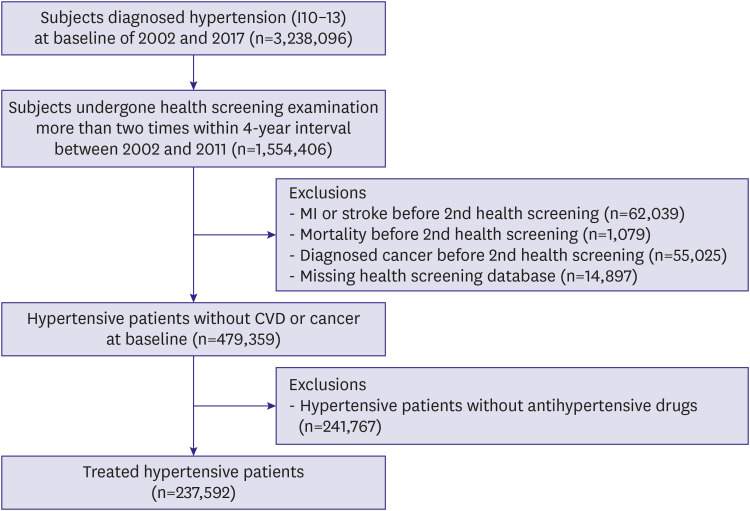
During the 2002–2011 period, 1,554,406 adults aged ≥19 years who underwent at least 2 separate health examinations within 4 years were identified. Of these, data from 612,399 individuals, who had already been diagnosed with hypertension (I10–I13) or were prescribed anti–hypertensive agents before their first health examination, were extracted. We excluded 62,039 individuals who had experienced myocardial infarction (MI) or stroke, 1,079 who had died, 55,025 diagnosed with malignancies between the first and last health examination, and 14,897 with missing relevant data in the health examination database. Of the 479,359 patients with hypertension, 241,767 patients who were not taking any antihypertensive medications were excluded. Finally, 237,592 patients treated for hypertension were included in the final analysis; these patients were prescribed antihypertensive medications between the first and second health examinations. Participants were followed up until death from any cause, major CV events, or the end of the study (December 31, 2017), whichever was earlier. Figure 1 shows the flow chart of the study population.
Blood pressure measurement and definition of elevated on-treatment diastolic blood pressures
BP was measured using either sphygmomanometers or oscillometric devices after at least 5 min of rest during a health examination. The staff who performed the measurements had been advised to select a cuff of an appropriate size, and to repeat the measurements ≥2 times at 1–2 min intervals. BP was defined as the mean value of BP measurements from two separate health examinations at 2-year intervals within 4 years. The BP measurement closest to January 1, 2002 was considered as the first BP measurement.
The elevated on-treatment DBP by the JNC7 definition was demarcated according to a BP target of <140/90 mmHg and we defined elevated on-treatment DBPs as an SBP <140 mmHg with a DBP ≥90 mmHg. The elevated on-treatment DBP by the 2017 ACC/AHA definition was demarcated according to a lowered BP target of <130/80 mmHg, and we defined elevated on-treatment DBPs as an SBP <130 mmHg with a DBP ≥80 mmHg.
Clinical variables
Age, sex, household income quartiles, smoking, physical activity, alcohol consumption, fasting plasma glucose, body mass index (BMI), fasting serum glucose, serum total cholesterol, diabetes mellitus, aspirin use, statin use, classes of antihypertensive medications, and the Charlson Comorbidity Index (CCI) were used as risk variables in each risk model used. Each participant’s medical history, family history, smoking and exercise habits were identified using a self-reported questionnaire. CCI was calculated according to Quan et al.18)
Clinical outcome events and assessment
The primary endpoint was the first occurrence of a major adverse cardiac event (MACE), defined as the composite of death from CV cause, non-fatal MI, or non-fatal stroke. Secondary endpoints included individual components of the primary composite outcome. All deaths and causes were retrieved from the mortality records of the National Statistical Office of the Republic of Korea. CV death was defined as death due to CV diseases (ICD-10 codes I00–I99) as mentioned on the certificate. MI was defined as hospitalisation with codes I21, I22, and I23 mentioned as the primary or secondary diagnosis. Stroke was defined based on the diagnosis delivered at discharge (I60–64).19)
Statistical analyses
Given the differences in the baseline characteristics between those with achieved target DBPs and elevated on-treatment DBPs, propensity-score matching was used to identify a cohort of patients with similar baseline characteristics.20) Multivariate cox proportional hazard models were used to evaluate the associations between baseline BP and the risk of CV events. The subgroup analyses were based on median age, aspirin or statin use, classes of antihypertensive medications, and CCI. We conducted several sensitivity analyses. Cofounders included in Model 1 were age and sex. Model 2 was adjusted for variables in Model 1 plus clinical variables. Model 3 was adjusted for variables in Model 2 plus time-varying SBP to perform an analysis including the follow-up BP data. Time-varying SBP were updated at each available study visit so that all longitudinal study visit SBP data were incorporated. Supremum test of the proportional hazards assumption was performed in Cox regression model to identify models satisfying assumptions required for proportional hazard analysis. Detailed statistical methods are described in the Supplementary Data 1.
RESULTS
Baseline characteristics of the study population
Of the 237,592 patients treated for hypertension, 157,971 patients achieved the target DBPs (66.5%) and 6,891 patients had elevated on-treatment DBPs (2.9%) by the JNC7 definition, whereas 57,859 patients achieved target DBPs (36.6%) and 23,437 patients had elevated DBPs (10.7%) by the 2017 ACC/AHA definition. The median duration of follow-up was 9 years (interquartile range: 7–11 years). During the follow-up period, the median of times that BP was measured was 6 occasions (interquartile range: 4–7 times). The descriptive characteristics of subjects who achieved target DBPs and had elevated on-treatment DBPs by the JNC7 and the 2017 ACC/AHA definitions are described in Tables 1 and 2, respectively. Before the propensity-score matching, there were differences in age, BPs, household income, smoking, physical activity, alcohol consumption, BMI, total cholesterol, diabetes mellitus, aspirin use, statin use, antihypertensive drug classes, and CCI between those who achieved target DBP and those had elevated on-treatment DBP by the JNC7 definition. There were differences between subjects who achieved target DBPs and had elevated on-treatment DBPs in age, BPs, household income, smoking, physical activity, alcohol consumption, BMI, total cholesterol, fasting glucose, diabetes mellitus, aspirin use, statin use, antihypertensive drug classes, and CCI by the 2017 ACC/AHA definition in overall study population. After matching, the standardised mean differences were <10.0% for all variables, indicating well-balanced covariate distributions between the groups (Tables 1 and 2).
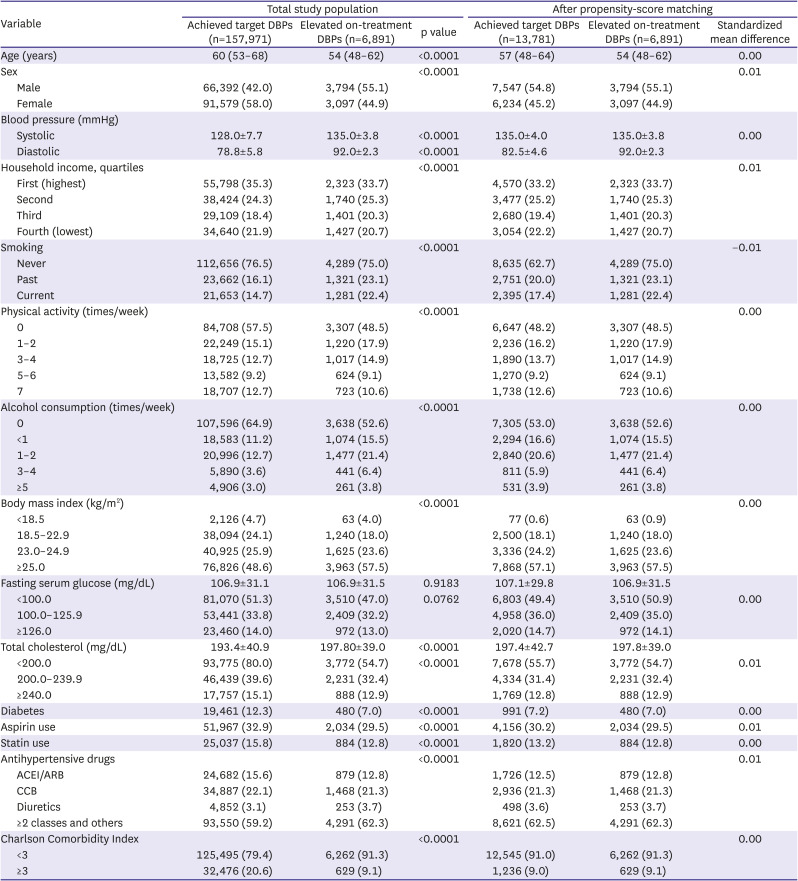
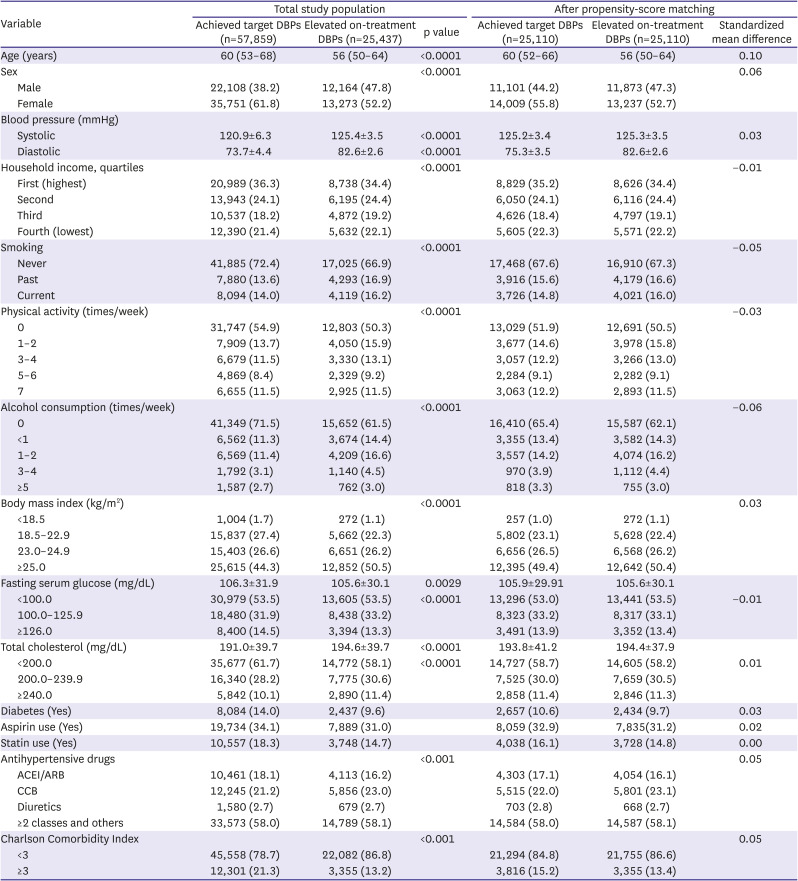
Table 1
Descriptive characteristic of subjects achieved target DBPs and elevated on-treatement DBPs by the JNC7 definition
Values are presented as median (interquartile range), mean ± standard deviation or number (%). Subjects achieved target DBPs were defined as systolic blood pressure <130 mmHg and diastolic blood pressure <80 mmHg by the JNC7 definition.
ACC = American College of Cardiology; AHA = American Heart Association; ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; CCB = calcium channel blocker; DBP = diastolic blood pressure; IQR = interquartile range; JNC7 = The Seventh Report of Joint National Committee.
![]()
Table 2
Descriptive characteristic of subjects achieved target DBPs and elevated on-treatement DBPs by the 2017 ACC/AHA definition
Values are presented as median (interquartile range), mean ± standard deviation or number (%). Subjects achieved target DBPs were defined as systolic blood pressure <130 mmHg and diastolic blood pressure <80 mmHg by the 2017 ACC/AHA definition.
ACC = American College of Cardiology; AHA = American Heart Association; ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; CCB = calcium channel blocker; DBP = diastolic blood pressure; JNC7, The Seventh Report of Joint National Committee.
![]()
Elevated on-treatment diastolic blood pressures and primary endpoint
The incidence of MACEs, which was the primary endpoint in individuals with elevated DBPs of both groups is shown in Supplementary Table 1 for the total study population and in Supplementary Table 2 for propensity-matched cohort.
Those by the JNC7 definition, there were a total of 621 MACEs in patients with elevated DBPs. They had a higher risk of MACE in the total study population (adjusted hazard ratio [aHR], 1.14; 95% confidence interval [CI], 1.05–1.24) and propensity-score matched cohort (aHR, 1.12; 95% CI, 1.01–1.23), as compared with individuals who achieved the target DBP.
In the analysis of elevated on-treatment DBPs by the 2017 ACC/AHA definition, a total of 2,333 MACEs occurred in the elevated DBP group. Compared with the group that achieved the target DBPs, the elevated DBP group was not associated with a higher risk of MACEs in the total study population (aHR, 1.04; 95% CI, 0.99–1.10), and propensity-score matched cohort (aHR, 1.03; 95% CI, 0.98–1.09) (Figure 2A and B).

Figure 2
Mortality and cardiovascular events in subjects with DBP target by either the JNC7 or the 2017 ACC/AHA definitions. (A) Total study population, (B) After propensity-score matching, and (C) Subgroup analysis for MACE in total study population.
ACC = American College of Cardiology; AHA = American Heart Association; CI = confidence interval; DBP = diastolic blood pressure; HR = hazard ratio; JNC7 = The Seventh Report of Joint National Committee; MACE = major adverse cardiac event; MI = myocardial infarction.
*The p value <0.05 for hazard ratio. Hazard ratio calculated by Cox proportional hazards regression analysis after adjustments for age, household income, smoking, physical activity, alcohol consumption, body mass index, fasting serum glucose and total cholesterol levels, diabetes mellitus, classes of antihypertensive medications, and Charlson Comorbidity Index.
![]()
Elevated on-treatment diastolic blood pressures and secondary outcomes
Elevated on-treatment DBPs by the JNC7 definition was associated with a higher risk of CV mortality in the total study population (aHR, 1.42; 95% CI, 1.18–1.70) and propensity-score matched cohort (aHR, 1.59; 95% CI, 1.26–2.00). In contrast, elevated DBPs by the 2017 ACC/AHA definition did not show this association in the total study population (aHR, 0.97; 95% CI, 0.87–1.08) and propensity-score matched cohort (aHR, 1.11; 95% CI, 0.98–1.27). Elevated on-treatment DBPs in both groups were not associated with the risk of non-fatal MIs in the total study population.
However, elevated on-treatment DBPs in both groups were associated with an increased risk of non-fatal stroke. In those by the JNC7 definition, the adjusted HRs were 1.19 (95% CI, 1.08–1.30) in the total study population and 1.12 (95% CI, 1.01–1.25) in the propensity-score matched cohort. Those by the 2017 ACC/AHA definition, the adjusted HRs were 1.10 (95% CI, 1.04–1.16) in the total study population and 1.07 (95% CI, 1.02–1.14) in the propensity-score matched cohort (Figure 2A and B).
Subgroup and sensitivity analyses
Figure 2C summarises results of subgroup analysis for MACEs in the total study population. In the analysis including those by the JNC7 definition, women with elevated DBPs had a significantly higher risk of MACEs (p for interaction=0.0392) and stroke (p for interaction=0.0347). In the analysis including those by the 2017 ACC/AHA definition, there were no statistically significant differences when the groups were stratified according to sex (all p for interaction>0.05). In the subgroup analyses based on sex, elevated on-treatment DBPs by the JNC7 definition did not show statistically significant differences in the CV mortality and non-fatal MI (p for interaction>0.05) between the groups (Supplementary Figure 1).
In the subgroup analyses based on median age (60 years), elevated on-treatment DBPs in both groups showed no differences between the subgroups for all endpoints except CV mortality. In the analysis including the 2017 ACC/AHA group, there was a significant difference in the risk of CV mortality according to age; subjects with elevated on-treatment DBPs who were aged <60 years were associated with a lower risk of mortality due to CV causes (p for interaction=0.0267). Subgroup analysis stratified according to concomitant medications is shown in Supplementary Figure 1. The subgroup analyses based on the use of aspirin or statin did not reveal any subgroup differences. Subgroup analysis stratified according to sex, age, and concomitant medications in propensity-matched cohort is presented in Supplementary Figure 2.
Figure 3 shows the results of sensitivity analysis for elevated on-treatment DBPs in both the groups. Elevated on-treatment DBPs by the JNC7 definition were associated with a higher risk for MACEs, CV mortality, and non-fatal stroke in all the three models. In contrast, elevated on-treatment DBPs by the 2017 ACC/AHA definition did not show increased risks for MACEs, except after adjusting for SBP as a time-varying covariate. Elevated on-treatment DBPs were not associated with increased CV mortality in all three models. In contrast to other events, non-fatal stroke was the only event that was significantly higher in those with elevated on-treatment DBPs by the 2017 ACC/AHA definition, in all the three models. Tests of the proportional hazards assumption in Cox regression models are shown in Supplementary Table 3.
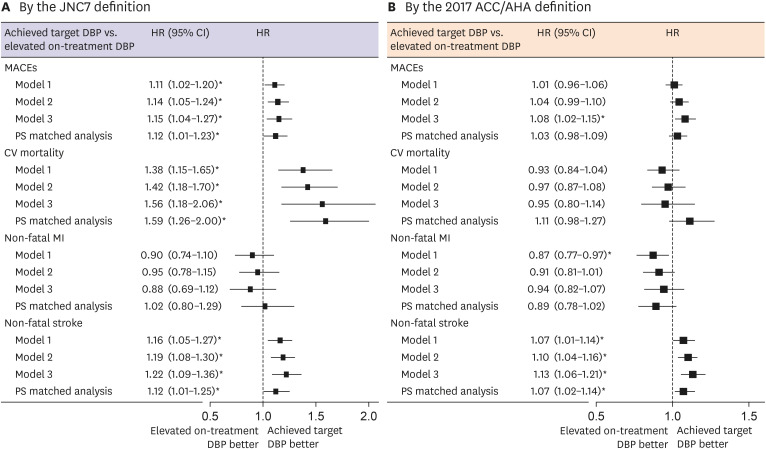
Figure 3
Associations between each endpoint and two different levels of elevated on-treatment DBPs in the presence of achieved SBPs, lowered by either the JNC7 or the 2017 ACC/AHA definition.
Model 1 is adjusted for age and sex. Model 2 is adjusted for model 1+ household income, smoking, physical activity, alcohol consumption, body mass index, fasting serum glucose and total cholesterol levels, diabetes mellitus, use of aspirin or statin, classes of antihypertensive medications, and Charlson Comorbidity Index. Model 3 is adjusted for model 2 + time-varying systolic blood pressure.
PS matched analysis is adjusted for age, household income, smoking, physical activity, alcohol consumption, body mass index, fasting serum glucose and total cholesterol levels, diabetes mellitus, use of aspirin or statin, classes of antihypertensive medications, and Charlson Comorbidity Index in propensity-score matched cohort.
ACC = American College of Cardiology; AHA = American Heart Association; CI = confidence interval; DBP = diastolic blood pressure; HR = hazard ratio; JNC7 = The Seventh Report of Joint National Committee; MACE = major adverse cardiac event; MI = myocardial infarction; PS = propensity-score.
*The p value <0.05 for hazard ratio.
![]()
DISCUSSION
In this study, we found that (1) elevated on-treatment DBPs was associated with an increased incidence of MACEs and CV mortality in patients treated for hypertension, not by the 2017 ACC/AHA definition (SBP <130, DBP ≥80 mmHg), but by the JNC7 definition (SBP <140, DBP ≥90 mmHg); (2) elevated on-treatment DBPs by the 2017 ACC/AHA definition was associated with an increased risk of stroke alone; and (3) the subgroup analysis stratified according to sex showed a significant difference in the primary endpoint and non-fatal stroke for elevated on-treatment DBPs by the JNC7 definition; women with elevated on-treatment DBPs by the JNC7 definition had a higher risk of CV events.
Although DBP was historically thought to be a key factor for adverse cardiac outcomes,21) the results of Framingham and other observational cohorts studies5)22) conducted after the 1990s found that there was a gradual shift from DBP to SBP as the main predictor of CV risk with age. However, several epidemiologic studies have consistently reported an increased risk of CV disease at a DBP of >75 mm Hg, 3)5)6)23) and that CV events increased sharply at a DBP >90 mmHg.24) Some studies have suggested that DBP is the strongest predictor of coronary heart disease in patients aged >50 years.25)26)
Diastolic hypertension without the elevation of SBP has been a distinct phenotype of hypertension in the early phase of hypertension. Nevertheless, several observational11)12)13)14)15)27) evaluating the prognostic implication of a specific hypertension phenotype rather than the threshold of DBP, have reported conflicting results. A recent study15) examined 14348 participants in the Atherosclerosis Risk in Communities (ARIC) (treated patients with hypertension) and showed that IDH defined by either the JNC7 guideline or 2017 ACC/AHA guideline was not associated with atherosclerotic CV disease, heart failure, or chronic kidney disease. The result of the study15) cannot be generalised to younger subjects because the minimum age of ARIC participants was 48 years, and DBP usually decreases with age.28) In contrast, Lee et al.13)14) reported that among non-treated adults in the Republic of Korea aged between 20 and 89 years with IDH, as defined by the 2017 ACC/AHA guideline, those with IDH as compared with normal BP, had significantly higher risks for subsequent CV disease events.
Interestingly, in our study, treated adults in the Republic of Korea with elevated on-treatment DBPs and achieved target SBPs by the 2017 ACC/AHA definition were associated with stroke alone. The reason for this is unclear, although it is apparent that IDH in non-treated subjects, and elevated DBPs in treated subjects who achieved SBP targets, need to be treated separately. In a pooled analysis of the ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial (ONTARGET) and Telmisartan Randomised Assessment Study in ACE Intolerant Subjects With Cardiovascular Disease (TRANSCEND) trials involving patients at high risk of CV disease who achieved low SBP of 120 to <140 mmHg, the lowest risk for all outcomes was observed at an achieved DBP of 70 to <80 mmHg.8) These data significantly influenced the decision to define a strict DBP range in the 2018 ESC/ESH guideline. However, the benefit of decreasing the DBP to <80 mmHg for patients on anti-hypertensive treatment still needs further supporting data.
In the Hypertension Optimal Treatment (HOT) Trial, the strategy to treat DBP to achieve a level of 80 mmHg showed no significant benefit compared with the achievement of a level of 90 mmHg, in patients without diabetes.29) In the HOT trial, the maximum benefits of treatment were observed in those who achieved a DBP between 80 and 85 mmHg. In the meta-analysis,7) including 16 randomised controlled trials, including the Systolic Blood Pressure Intervention Trial (SPRINT), HOT, and Action to Control Cardiovascular Risk in Diabetes (ACCORD) trials, intensive DBP lowering under 80 mmHg was beneficial in lowering stroke or the composite risks of stroke and coronary heart disease. The discrepancy among studies may originate on account of different baseline characteristics. The ONTARGET and TRANSCEND trials randomised high-risk patients. High-risk patients (aged ≥55 years) with at least one incidence of coronary artery, peripheral artery, cerebrovascular disease or diabetes mellitus were enrolled in the ONTARGET trial. In the HOT trial, the proportion of previous MI, stroke or diabetes mellitus was small. In our study, patients with a previous history of MI or stroke were excluded. The biological plausibility for diastolic J-shape phenomenon has been proposed and accepted, but the result of this study indicates that the threshold and range of the J-curve can differ even in treated hypertensive patients who have achieved a SBP target according to their baseline characteristics.
Our data showed the benefit of a lower target DBP <80 mmHg in people who have achieved low SBP (<130 mmHg) is less clear; however, it can be considered beneficial in reducing the risk of stroke. Nevertheless, the benefit of lower target DBP <80 mmHg for other secondary endpoints, including CV mortality, requires more supporting data.
It also needs to be noted that sex-stratified analysis in this study revealed that elevated on-treatment DBPs by the JNC7 definition was associated with higher risks of major CV events in women, which was mainly driven by an increased risk of stroke. This finding emphasises strict DBP control under 90 mmHg in women who have achieved low SBP <140 mmHg, to reduce the incidence of MACEs. Although there is a paucity of data describing the effect of sex on the optimal target BP for reducing the risk of adverse clinical outcomes, our study showed additional benefits from a stricter DBP-lowering treatment in female patients.
First, it was a retrospective cohort study using NHIS data, and thus had the inherent limitations of this type of analysis, although propensity-score matching was used to minimize the influence of unbalanced baseline characteristics. The purpose of NHIS data is for administrative-claim, and not for the research, which is its inevitable limitation and definitions of variables using ICD codes do not always reflect the actual clinical presentation. Second, this study’s population was of homogeneous Korean ethnicity, and hypertensive patients with past CV events were excluded; hence, caution is necessary before generalising the findings of this study to people with other ethnic backgrounds or high-risk patient profiles. Third, it is difficult to standardize BP measurement with NHIS dataset, as well as there are plenty of confounding variables associated with the assessment of BP level. We arbitrarily defined BP as the mean value of BP from two separate health examination at 2-year intervals within 4 years, which might be too less frequent and long-time interval to categorize the patients into the two DBP achieved group, although we performed a sensitivity analysis using SBPs at follow-up period as a time-varying covariate. Therefore, further studies are warranted with the more frequent BP measurements and randomized controlled studies to confirm our hypothesis. Fourth, temporal changes in the use of antihypertensive medication were not evaluated during the follow-up period. Finally, the data of BP from the health screening examination are fundamentally limited to predict CV events. Out of office BPs can be more reliable and relevant to clinical outcomes and the pattern of BP fluctuation is closely related the prognosis of CV disease.
In this nation-wide population-based study, subjects with elevated DBPs and achieved target SBPs in the JNC7 group had an increased risk for CV events, including mortality; however, this was not observed with elevated on-treatment DBPs in the 2017 ACC/AHA group with a lower DBP threshold of 80 mmHg. The results of this study provide evidence of the value of an DBP target in subjects who have achieved low SBP goals.
 XML Download
XML Download