

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic limb threatening ischemia (CLTI) is the most advanced stage of peripheral artery disease (PAD) with high morbidity and mortality. Patients with CLTI have high risk for other cardiovascular disease such as coronary artery disease or carotid artery disease.1) In addition to risk factor control and optimal medical therapy, revascularization is recommended to minimize tissue damage in CLTI patients.2)3) Until now, the Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial is the only prospective randomized trial to evaluate long-term outcomes of revascularization in CLTI, and demonstrated that bypass surgery and balloon angioplasty are associated with similar outcomes regarding amputation-free survival (AFS).4) Although the optimal strategy for revascularization in CLTI patients is still controversial, endovascular therapy (EVT) have shown comparable outcomes to surgical bypass in recent studies.5)6)
In recent years, EVT has become a useful revascularization method as an alternative to surgical bypass in the management of CLTI patients in real-world practice.7)8) However, risk factors for poor long-term outcomes after EVT in CLTI patients have not been extensively studied compared to those after surgical bypass. Therefore, we investigated long-term outcomes of CLTI patients who underwent EVT and identified independent predictors for poor outcomes from a Korean multicenter registry data.
METHODS
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki as revised in 2013 and approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital and each participating hospital. The IRBs of the participating hospitals waived the requirement of informed consent due to the retrospective nature of the study (approval number: 3-2015-0165).
Study population
The Korean Vascular Intervention Society (K-VIS) Endovascular therapy in Lower Limb Artery diseases (ELLA) registry is a multicenter observational study with retrospective and prospective cohorts of patients with lower extremity artery disease treated with endovascular therapy (ClinicalTrials.gov: NCT02748226). The present study used data from the retrospective patient cohort, which consists of datasets from 3,073 patients with 3,972 target limbs treated between January 2006 and July 2015 in 31 Korean hospitals. The K-VIS ELLA registry study design and results have been described in detail previously.9) From this registry population, 1,036 patients with CLTI (1,292 limbs) were finally included in the current analysis. Data regarding the patients’ demographics, baseline clinical and lesion characteristics, clinical presentation, laboratory test results, treatments, and follow-up outcomes were collected from electronic medical records.
Definitions and study endpoints
The PAD of the lower extremity was defined as the presence of ≥50% narrowing of a lower extremity artery. CLTI was defined as Rutherford category (RC) 4, 5, or 6 disease (ischemic rest pain, minor tissue loss, or major tissue loss, respectively).10) Definitions of diabetes, hypercholesterolemia, smoking, congestive heart failure (CHF), anemia, and chronic kidney disease were described in a previous report.9)
Technical success was defined as successful revascularization with residual stenosis <30% and absence of flow-limiting dissection or a hemodynamically significant translesion pressure gradient. Major amputation was defined as any lower extremity amputation at the level of or above the ankle, and a minor amputation was defined as any lower extremity amputation below the ankle, including the foot or toe(s).
The primary outcome of this study was AFS defined as the absence of major amputation or death. Changes in the hazard rate of major amputation or death were also evaluated. Secondary endpoints were major adverse limb events (MALE; a composite of major amputation, minor amputation, and reintervention), and changes in the hazard rate for MALE were also analyzed.
Statistical analysis
Continuous variables are presented as mean ± standard deviation and were compared using Student’s t-test. Categorical variables are presented as number (percentage) and were compared using the χ2 test. Data were analyzed on a per-patient basis for clinical characteristics and on a per-lesion basis for the limb, lesion, or procedural characteristics. Cumulative incidences of clinical events were presented as Kaplan-Meier estimates and hazard rates for primary and secondary endpoints were obtained at 6-month interval. Univariate Cox proportional hazards regression analyses using baseline clinical, lesion, and procedural variables were performed to identify independent predictors of major amputation or death and MALE. The variables achieving a p value <0.25 in the univariate analysis were evaluated in the multivariate analysis model to determine the independent predictors of clinical events. The results were displayed as hazard ratio (HR) and 95% confidence interval (CI). All statistical analyses were performed using SPSS (version 23.0; IBM Corp., Armonk, NY, USA). All tests were two-sided, and p<0.05 was considered statistically significant.
RESULTS
Baseline characteristics
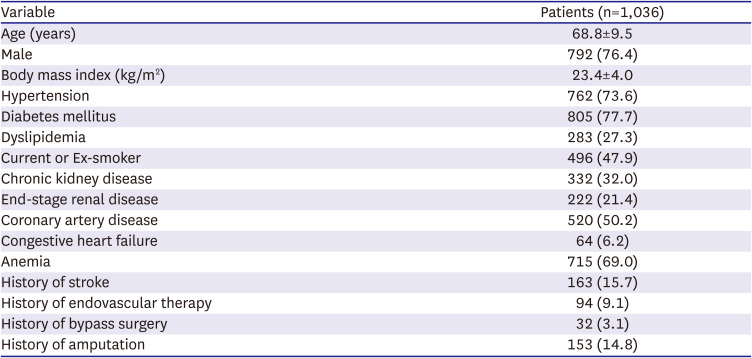
Baseline clinical characteristics of 1,036 CLTI patients enrolled are summarized in Table 1. Mean age was 68.8±9.5 years, and 76% of the patients were male. Diabetes mellitus and end-stage renal disease (ESRD) on dialysis were observed in 78% and 21% of patients, respectively.
Table 1
Baseline characteristics
Procedural characteristics and complications
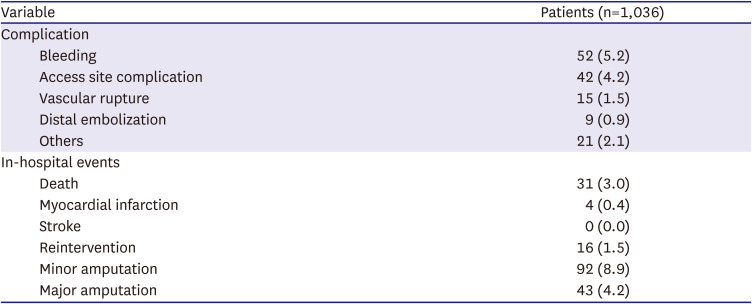
Table 2 demonstrates baseline lesion and procedural characteristics for 1,292 target limbs. Tissue loss was observed in 77% of patients (RC-5: 48%, RC-6: 29%). Three quarters of the lesions belonged to Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC) II class C/D. Femoropopliteal artery was the most common target vessel and 51% of the lesions were totally occluded. Technical success was achieved in 88% of the procedures (Table 2). The procedural complication rate and in-hospital event rate was 9% and 18%, respectively (Table 3).
Table 2
Lesion and procedural characteristics
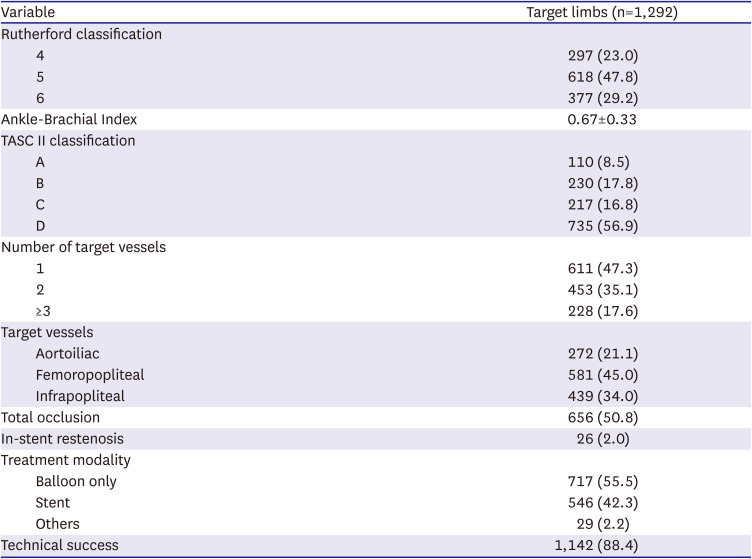
Table 3
Procedural complications and in-hospital events
AFS and predicting factors for major amputation or death
The median follow-up duration was 613 days (interquartile range 201–730 days). The Kaplan-Meier curve in Figure 1A illustrates AFS, and 5-year AFS rate was 69.8%. In the multivariate Cox regression model, age (HR, 1.476; 95% CI, 1.214–1.796; p<0.001), ESRD (HR, 2.340; 95% CI, 1.594–3.436; p<0.001), RC-6 (HR, 1.434; 95% CI, 1.014–2.028; p=0.041), and suboptimal EVT (HR, 1.798; 95% CI, 1.191–2.713; p=0.005) were independent predictors of major amputation or death (Table 4). Paradoxically, smoking (HR, 0.594; 95% CI, 0.405–0.870; p=0.007) was associated with improved AFS.
Figure 1
Kaplan–Meier survival curve and hazard rate of major amputation or death after endovascular treatment. (A) Kaplan-Meier survival curve demonstrating amputation-free survival after endovascular treatment in 1,036 patients with chronic limb threatening ischemia. (B) Hazard rate for major amputation or death after endovascular treatment at 6-month interval.
CI = confidence interval.
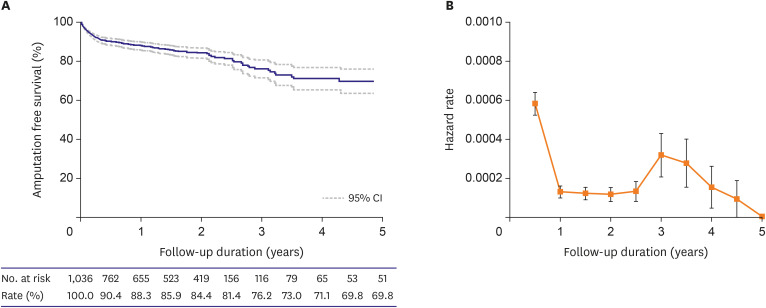
Table 4
Predictors of major amputation and death after endovascular treatment
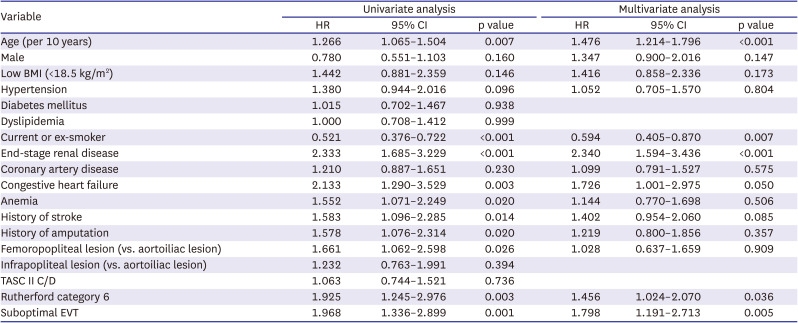
Figure 1B shows the change in hazard rate of major amputation or death after EVT at 6-month interval. Hazard rate of major amputation or death was highest in the first 6 months and remained low afterwards. However, it increased again around 3 years after EVT. Factors associated with 6-month major amputation or death were age (HR, 1.471; 95% CI, 1.158–1.869; p=0.002), ESRD (HR, 2.033; 95% CI, 1.275–3.243; p=0.003), RC-6 (HR, 1.633; 95% CI, 1.075–2.481; p=0.021), and suboptimal EVT (HR, 1.970; 95% CI, 1.196–3.245; p=0.008), whereas smoking (HR, 0.615; 95% CI, 0.392–0.963; p=0.034) was protective (Supplementary Table 1). However, after 6 months, low body mass index (BMI: HR, 2.423; 95% CI, 1.211–4.850; p=0.012), ESRD (HR, 2.444; 95% CI, 1.360–4.390; p=0.003), and history of stroke (HR, 1.959; 95% CI, 1.092–3.514; p=0.024) were independent predictors of major amputation or death (Supplementary Table 2). Smoking was not a significant predictor during this period.
Freedom from MALE and predicting factors for MALE
The Kaplan-Meier curve in Figure 2A demonstrates freedom from MALE, and 5-year freedom from MALE was 61%. Table 5 shows factors associated with MALE after EVT. In multivariable analysis, low BMI (HR, 1.505; 95% CI, 1.008–2.247; p=0.046), ESRD (HR, 1.648; 95% CI, 1.214–2.238; p=0.001), femoropopliteal lesion (HR, 1.877; 95% CI, 1.220–2.889; p=0.004), RC-6 (HR, 1.471; 95% CI, 1.104–1.960; p=0.008), and suboptimal EVT (HR, 1.847; 95% CI, 1.301–2.624; p=0.001) were independent predictors of MALE.
Figure 2
Kaplan–Meier survival curve and hazard rate of MALE after endovascular treatment. (A) Kaplan-Meier survival curve demonstrating freedom from MALE in 1,036 patients with chronic limb threatening ischemia. (B) Hazard rate for MALE after endovascular therapy at 6-month interval.
CI = confidence interval; MALE = major adverse limb events.
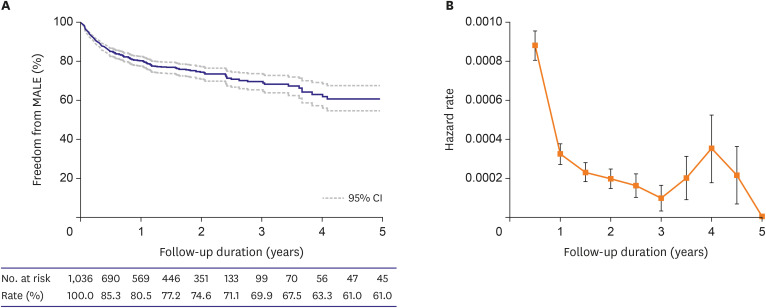
Table 5
Predictors of any amputation and reintervention after endovascular treatment
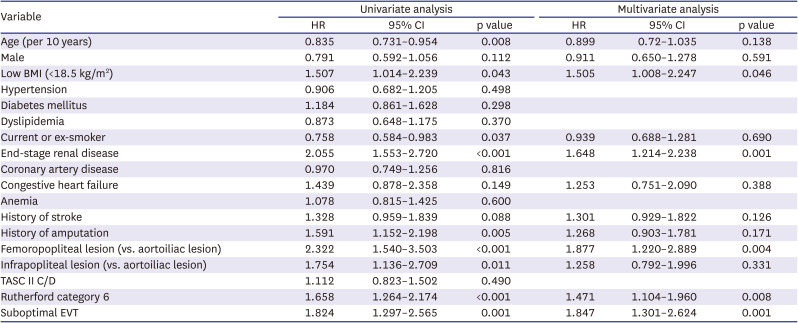
Figure 2B shows the change in hazard rate of MALE after EVT at 6-month interval. Similar to the hazard rate of major amputation or death, hazard rate of MALE was highest in the first 6 months and then increased again around 4 years after EVT. ESRD (HR, 1.520; 95% CI, 1.036–2.231; p=0.032), RC-6 (HR, 1.438; 95% CI, 1.003–2.063; p=0.048), and suboptimal EVT (HR, 1.914; 95% CI, 1.234–2.969; p=0.004) were independent predictors of MALE during the first 6 months after EVT (Supplementary Table 3), whereas low BMI (HR, 2.325; 95% CI, 1.311–4.125; p=0.004), ESRD (HR, 2.027; 95% CI, 1.223–3.361; p=0.006), femoropopliteal lesion (HR, 2.114; 95% CI, 1.112–4.019; p=0.022), and suboptimal EVT (HR, 2.033; 95% CI, 1.139–3.626; p=0.016) were significant predictors of MALE thereafter (Supplementary Table 4).
DISCUSSION
For CLTI patients, it is recommended to perform revascularization as much as possible to minimize tissue damage.2)3) Recent large-scale real-world data also showed that revascularization was associated with better outcomes in terms of amputation-free survival and overall survival in patients with CLTI.11) Although the optimal strategy for revascularization in CLTI remains controversial, EVT have shown comparable outcomes to surgical bypass in terms of mortality or AFS in many studies and their meta-analyses.4)5)6)12)13) With the development of new devices and various endovascular techniques, EVT first strategy has been widely accepted as an alternative to surgical bypass for the treatment of CLTI patients in real-world practice.7)8)
In this study, we investigated long-term outcomes of CLTI patients from a multicenter registry, who underwent EVT and managed under real-world conditions. Although direct comparison with previous studies is difficult, given the high risk of CLTI patients, outcomes observed in our study are considered acceptable. Long-term durability of EVT in CLTI patients is still debatable. The BASIL trial is the only prospective randomized trial to evaluate long-term outcomes of EVT in CLTI compared with bypass surgery.4) However, balloon angioplasty was the only EVT method in BASIL trial. Therefore, it would be hard to see that it reflects current practice. In a retrospective study using California nonfederal hospital data, Lin et al.6) demonstrated that open surgical bypass was associated with worse AFS compared with EVT (HR, 1.16; 95% CI, 1.13–1.20) during the 80-month follow-up period in patients with ischemic ulcers of the lower extremities. In a observational study using Medicare claims data, Mustapha et al. compared long-term outcomes with angioplasty, stenting, atherectomy, or surgical bypass in CLTI patients.5) All-cause mortality over 4 years was lowest with atherectomy (49.3%) and highest with angioplasty (54.7%). Major amputation rates over 4 years were 6.8% with atherectomy, 7.8% with stenting, 8.1% with angioplasty, and 10.8% with surgical bypass.
The risk of clinical events did not remain constant during the follow-up period. Iida et al. reported follow-up results of a prospective multicenter endOvascuLar treatment for Infrainguinal VEssel (OLIVE) registry, in which 3-year AFS and freedom from MALE were 55.2% and 84.0%, respectively.14) They found that the highest hazard rates were observed during the first 6 months for both major amputation or death and MALE. Therefore, they suggested that wound healing status after EVT during the first 6 months affect the outcome of the following 3 years.14) Our study findings were also consistent with those of Iida’s study. Moreover, when followed-up for up to 5 years, it was observed that the hazard rate increased again in our study. Around 3 years after EVT, the hazard rate of major amputation or death increased again, mainly due to an increase in mortality. The hazard rate of MALE rose again around 4 years after EVT, primarily due to an increase in reintervention. Similarly, in post-hoc analysis of BASIL trial, a hazard in AFS and all-cause mortality for balloon angioplasty was significantly increased compared to surgical bypass in the period beyond 2 years from randomization.4)15) These findings may suggest the importance of more complete revascularization and careful long-term surveillance after EVT. However, these results in our study were based on an analysis of later events from the relatively small number of patients. Therefore, later increase of clinical events during long-term follow-up period should be confirmed in the future prospective studies.
In this study, ESRD, RC-6, and suboptimal EVT were identified as independent predictors for MALE as well as major amputation or death. These findings are emphasizing the importance of renal function and wound severity, in addition to successful EVT, in the prognosis of CLTI patients. These results were consistent with those of previous studies.14)16)17) Additional risk factor for reduced AFS was age. Low BMI has been reported as a predicting factor for mortality in previous studies.14)18) However, in our study, it was identified as an independent predictor for MALE, not reduced AFS.
Subgroup analysis according to the lesion location demonstrated that patients with femoropopliteal lesion had worse outcomes in terms of amputation or death as well as MALE compared with those with aortoiliac lesions (Supplementary Figure 1). However, in the multivariate analysis, the femoropopliteal lesion location was an independent predictor only for MALE, not reduced AFS, and this is thought to be due to an increase in reintervention.
When analyzed by dividing the follow-up period after EVT into 6 months and beyond considering the highest hazard rate in the first 6 months, RC-6 was the predictor of early outcomes and low BMI was the predictor of late outcomes. However, ESRD was the predictor to affect both early and late outcomes regardless of the follow-up period after EVT.
Unusual finding in our study was that current or ex-smokers were paradoxically associated with improved AFS on both univariate and multivariate analyses. The same results were observed when only current smokers were included except ex-smokers. It may be due to the fact that the rate of patients with ESRD (14.1% vs. 28.1%, p<0.001), history of stroke (12.5% vs. 18.7%, p=0.003), or RC-6 (23.2% vs. 34.1%, p<0.001), which were independent predictors for reduced AFS, were significantly lower in current or Ex-smokers compared to non-smokers. However, considering the results of the multivariate analysis, this cannot be a sufficient explanation. Similar paradoxical results were also reported in some previous studies. O’Brien-Irr et al.19) reported that smoking was associated with improved sustained clinical success, defined as RC improvement without target extremity revascularization after EVT in chronic CLTI patients, although this association was not observed in multivariate analysis. Vierthaler et al.17) demonstrated that current or former smoking was correlated with improved freedom from amputation. Despite these paradoxical results, smoking is a strong risk factor for PAD and smoking cessation should be recommended in all patients with PAD.2)3)
This study had several limitations. First, the present study has the inherent limitations of retrospective analysis, including the possible presence of selection bias and uncorrected confounders. Second, information on ischemic wound healing or recurrence was not included our registry database. Therefore, wound outcome and predicting factors for wound recurrence were not analyzed. Third, we attempted to evaluate the overall long-term outcomes after EVT in CLTI patients under real-world setting. However, differences according to the specific EVT strategy were not evaluated in this study. In addition, considering the data collection period of this study, the latest EVT trend may not be sufficiently reflected. The comparison of outcomes between individual EVT methods will need to be addressed in the future prospective studies.
In conclusion, in retrospective analysis of Korean multicenter registry, long-term outcomes of EVT were acceptable in CLTI patients. ESRD, RC-6, and suboptimal EVT were common predictors for poor clinical outcomes.
 XML Download
XML Download