

 PDF
PDF Citation
Citation Print
Print



STRUCTURE AND FUNCTION OF THE TRICUSPID VALVE
The tricuspid valve (TV) is the largest valve among 4 cardiac valves and is located between the right atrium (RA) and right ventricle (RV).1) The TV incorporates 3 (anterior, posterior, and septal) leaflets that are supported by the tricuspid annulus (TA), which is a part of the cardiac skeleton composed of dense fibrous tissue.1) The TA is elliptical shape when observed from the RA side, and is also a non-planar, saddle-shape having the lowest (close to the apex) point at the posteroseptal portion and the highest point at the anteroseptal portion (Figure 1A).2) Each TV leaflet is attached to chordae and connected to the RV wall through the papillary muscles. All these structures are forming a functional complex for stable coaptation of leaflets during the RV systole and prevent tricuspid regurgitation (TR).1)3)
Figure 1
Structure of the TV and the TA. Structure of the TV observed from the RA side, and normal geometry of the TA being saddle-shape with the lowest posteroseptal portion and the highest anteroseptal portion (A). In functional TR, the TV is enlarged toward the direction of PL and the height of TA becomes lower with disappearance of normal saddle-like morphology (B).
AL = anterior leaflet; PL = posterior leaflet; RA = right atrium; RV = right ventricle; SL = septal leaflet; TA = tricuspid annulus; TR = tricuspid regurgitation; TV = tricuspid valve.
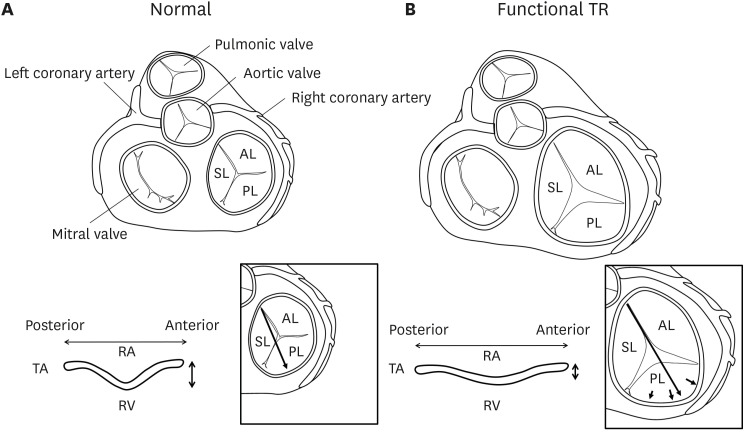
TV is a check valve between the RA and RV, prevents backward flow to RA and enhances blood flow to pulmonary circulation. Pulmonary circulation has higher vascular compliance and lower pressure compared to the systemic circulation.1) Thus, the RV has a thin wall (thickness of 3–5 mm) and a high surface-to-volume ratio which needs a smaller inward motion to stroke a same blood volume compared to the left ventricle (LV).1) Because of this physiologic background, given pathologic pressure overload to the RV, its adaptive capacity is significantly lower than that of the LV.1) With a chronic volume overload such as significant TR, the RV and RA fall to progressive dilatation, and the TA is enlarged toward the posterolateral direction, forming a planar shape and losing the normal saddle-like morphology (Figure 1B).4)5)6) Consequently, the TV apparatus falls to failure with accumulation of such structural alterations, therefore TR promotes more RV volume overload and more abnormal coaptation of TV, finally constitutes ‘a vicious cycle of TR.’3)7)
ETIOLOGIES AND CAUSES OF TRICUSPID REGURGITATION
Recently, there has been growing attention to the clinical significance of TR. In a community-based data with 20,000 persons, each prevalence of moderate and severe TR was 5% and 0.6%, respectively, which was similar to aortic stenosis (AS).8) Due to its pathophysiologic mechanisms, TR presents more commonly with left-side valve diseases than standing alone. Significant TR can be combined in about 25% of patients with severe AS, 30–50% of patients with severe mitral regurgitation (MR), and 30–40% of patients with mitral stenosis.8)9)10) Also, atrial fibrillation (AF) frequently causes gradual dilatation of RA with alterations in the TA structure, consequently it strongly promotes the development of TR.11)12)13) Therefore, in the current aging society with growing burden of valve disease, heart failure (HF) and AF as contributors to the development of TR, the prevalence and socioeconomic burden of TR are expected to be greater.14)15)
TR can be classified into primary and secondary TR.16) Primary TR is originated from organic TV pathologies including endocarditis, prolapse, rheumatic carditis, carcinoid, and Ebstein’s anomaly, and its proportion is about 8–10% in all patients with TR.16)17) The others belong to secondary TR, which means the absence of organic pathology, usually originating from all causes which interfere with intact coaptation of TV.17) Representatively, in patients with left-side valve disease, post-capillary pulmonary hypertension and resulted RV dysfunction can interfere with TV functions, therefore induce TR.18) One unique category of secondary TR is isolated TR that develops alone without left-side valve disease or pulmonary hypertension.10) Isolated TR comprises 10% of secondary TR and can be classified according to causative factors into AF-related (in about 50%), intracardiac device-related (20%), and by other causes (20%).7)19)
CLINICAL FEATURES OF THE PATIENTS WITH TRICUSPID REGURGITATION
In left-side valve diseases such as MR and AS, the elevated left atrial pressure and post-capillary pulmonary hypertension can be manifested with symptoms such as exertional dyspnea.18)20) Conversely, in TR, the elevated RA pressure is transmitted to the venous system of the whole body. Thus, the development of symptoms is relatively insidious.17)18) Usually, patients with TR do not present with overt cardiac murmur,8) and the patients are frequently asymptomatic even with incidentally detected mild to moderate TR on screening echocardiographic examinations.14) However, if patients have clinically overt symptoms and signs of right HF, TR is frequently much advanced and combined with irreversible RV damage.21)22) Because the systemic complications of right HF include liver cirrhosis, kidney dysfunction, and splenomegaly, patients are usually present with chronically wasted features. Thus, only the correction of TR can difficultly improve its poor clinical prognosis associated with these chronically debilitated features.17) At this stage of TR, it is a common frustrating real-world situation that the attending physician should discuss with patients selecting the highly risky surgery versus palliative treatment. In such clinical synopsis, the biggest problem for a physician in managing TR is that it is difficult to find an optimal point of intervention.14)17) Even in a patient with TR of moderate or severe degrees, diuretics can result in mimicking improvement as TR is sensitive to volume status. It can be another source of delayed intervention.14) Also, there has been a traditional misconception that TR combined with left-sided valve disease will be disappeared after the correction of causative left-side valve disease.16) Although this concept has been proven “not true” through the recent various clinical data, this has long been a barrier to the active therapeutic intervention of TR.23)24)
Despite such conventional ignorance, the clinical impact of TR has been clearly demonstrated through recent several clinical researches.21)25)26)27)28) Nath et al.21) reported a large-sized clinical data (n=5,223) that the patients with moderate TR (hazard ratio [HR], 1.17; 95% confidence interval [CI], 0.96–1.42) and severe TR (HR, 1.31; 95% CI, 1.05–1.66) presented significantly reduced survival compared to whom without TR. In a large-sized transcatheter aortic valve replacement (TAVR) registry (n=34,576), the mortality and readmission rate were significantly higher with increasing severity of TR.26) Topilsky et al.25) analyzed the prognosis of patients (n=353) with isolated TR by quantitative grading that the patients with severe TR (effective regurgitant orifice area [EROA] ≥40 mm2) showed significantly reduced 10-year survival compared to those without severe TR (38±7% vs. 70±6%; p<0.001).
CURRENT DIAGNOSTIC METHODS OF TRICUSPID REGURGITATION AND LIMITATIONS
The principle tool for the diagnosis of TR is transthoracic echocardiography (TTE).29) A comprehensive TTE examination for TR should include morphology and mobility of leaflets, completeness of coaptation, size of TA, and integrity of subvalvular structures.29) Also, sizes and functions of the RV and RA, and the severity of pulmonary hypertension should be assessed by TTE.29) Although TTE has such wide applications, it has also several important limitations.29) First of all, there is an inherent limitation of color Doppler, which is influenced by instrumental settings and various hemodynamic factors.24)29) Color Doppler is a velocity mapping (not a flow mapping), and the RV-RA pressure gradient is its direct determinant. Therefore, severity of TR on color Doppler is dependent on volume status and tends to be underestimated by reduction of volume loading.24) Because the amount of venous return to the right heart is variable according to respiration, TR jet area assessed by color Doppler can be exaggerated by almost twice during inspiration.16)24) Conversely, the TR jet area can be underestimated in TV prolapse with eccentric jet or in the RA with markedly elevated pressure.10) Because there are multiple sources of error in the diagnosis of TR depending only on color Doppler, a multiparametric approach is recommended in the current guidelines.29) The multiparametric approach aims to enhance the objectivity of diagnosis by complementing the limitations of individual parameters. The diagnostic parameters of TR are classified as qualitative, semiquantitative, and quantitative values.29)30) Qualitative parameters include leaflet morphology, jet size, density and shape of Doppler signal. Semiquantitative parameters are vena contracta (VC) width, proximal isovelocity surface area radius, and hepatic vein flow reversal. And quantitative parameters include EROA and regurgitant volume (RVol).29)30) Among those, given most of parameters consistently suggest mild or severe TR, the diagnosis is clear without difficulty.29) However, if there is inconsistency among parameters or given intermediate severity of TR, quantitative means are the most decisive variables, and moderate TR is diagnosed with EROA of 0.2–0.4 cm2 and RVol of 30–44 mL.29) But, a semiquantitative parameter, VC width (0.30–0.59 cm), is also used together as a determinant of moderate TR because of the difficulties of using quantitative parameters in routine practice.29) Calculating EROA and RVol can be a complex work in routine practice, and concern about measurement error is an important barrier to the general application of that parameters. Alternatively, the use of 2 additional targets to complement the diagnosis of TR is suggested, those are the diameter of TA and the morphology of TV coaptation.18) The TA diameter is relatively independent of volume status, and is an easily measurable target on routine TTE.18)24)31) Leaflet tethering caused by RV dysfunction results in incomplete TV coaptation (namely tenting), and it has been evaluated in various researches as the height, area, and volume of tenting to predict the severity and progression of TR.5)32)33)34) Because these values were only obtained from sophisticated post-processing in many studies, there are several problems with feasibility and reproducibility for application in routine practice.
Recently, Hahn et al.35) pointed out a serious problem with the conventional diagnostic system of TR (3 grades of mild, moderate, and severe), thus proposed additional grades of massive and torrential TR. The rationale of the 5-grade system is identifying “extremely severe TR,” which progressed for a very long time without intervention owing to its vague clinical manifestations.35) Although given a same grade of severe TR, there must be substantial variability in the amount of RVol. Therefore, defining massive and torrential TR for such heterogeneity seems reasonable.36) Also, a practical aim of the 5-grade system is to evaluate the treatment result of severe TR adequately.35) Recently, in the SCOUT (Percutaneous Tricuspid Valve Annuloplasty System for Symptomatic Chronic Functional Tricuspid Regurgitation) trial, the investigators found that despite a significant reduction of EROA (−0.22±0.29 mm2) by the transcatheter procedure for severe TR, still the TR grade remained as severe in the conventional diagnostic system.37) Therefore, a proposal for a new grading system for TR is reassuring with respect to such problems. However, considering the real-world situation in which even conventional 3-grade system is not fully implemented by multiparametric approach, there would be practical barriers for application of more complex diagnostic system and accumulation of clinical evidences.
Objective measurement of the RV and RA structure and function is essential in the diagnosis of TR. However, the RV has sail shape which means asymmetry and not a proper target for the assessment by 2-dimensional imaging, therefore TTE is an insufficient modality for that purpose.10)38) Currently, the representative parameters and the cut-off values for decreased RV systolic function are: TA systolic velocity (S’, <9.5 cm/s), tricuspid annular plane systolic excursion (TAPSE, <17 mm), and RV fractional area change (FAC, <35%).39) However, S’ velocity and TAPSE are targeted on a single point of the TA, and FAC is calculated from the single plane. Thus, those parameters have inevitable limitations to represent the global RV function.40) Also, S’ velocity has a limitation of the angle dependency, which is an important drawback of the Doppler technique.39)40) Therefore, cardiac magnetic resonance imaging (CMR) is the current golden standard for RV assessment which provides a raw 3-dimensional measurement value without a geometric assumption.41)42)43) CMR has an excellent spatial resolution which is adequate to visualize inside the RV cavity with coarse trabeculation.17) Direct measurement of RVol by the phase-contrast imaging is another strength of CMR, whereas EROA and RVol assessed by TTE are dependent on geometric assumptions.17) However, CMR also has serious limitations. Above all, despite the reality, “TR is a general medical issue,” the requirement of an expensive CMR equipment, protocol setting, and image specialists can be a special prerequisite.3) And, it requires a long scanning time and patient’s cooperation, such as breath-holding for the acquisition of optimal images, those are frequently limited by clinical situations.40) Additionally, motion artifact can be an important limitation as patients with TR are frequently combined with AF.40) Although the assessment of myocardial fibrosis of LV using CMR is recently highlighted in AS and MR,44)45)46) it is difficult by the current technology to perform tissue characterization of the RV because it has thin wall (3–5 mm).40)47)
As such, there is no single perfect diagnostic tool for TR, the multi-modality imaging will be the center of diagnosis similar to left-side valve diseases. A key point of multi-modality imaging is a comprehensive understanding of pathophysiology and a combination of complementary imaging tools. According to a recent study, the regurgitant fraction by CMR and RV strain by TTE are shown as significant predictors of survival in patients with severe TR.48) Furthermore, the addition of those parameters on conventional prognosticators (EuroSCORE II and HF symptoms) presented significantly enhanced diagnostic performance.48) Additionally, cardiac computed tomography (CT) can play another important role in the multi-modality imaging diagnosis of TR. With recent great advancements in TAVR procedures, clinical application of CT imaging is rapidly developing and involved in overall processes of TAVR, as it includes the AV morphology, severity of calcification, structures of LV outflow tract, ascending aorta, and vascular access.30) Concerning transcatheter procedures of TR, the cardiac CT will be an adequate tool to visualize the 3-dimensional TA. Additionally, it will help the decision of the device landing zone avoiding impingement of adjacent structures (right coronary artery and conduction system).17)40)49)
CURRENT STATUS OF SURGICAL TREATMENT OF TRICUSPID REGURGITATION
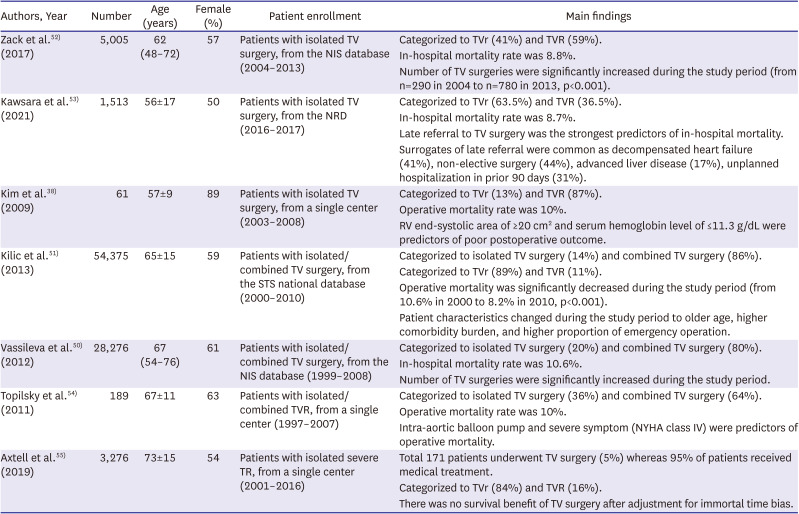
We summarized the clinical researches which reflected the real-world situations regarding the surgical treatment of TR, postoperative clinical outcomes, and difficulties in the decision of surgery (Table 1).38)50)51)52)53)54)55) Zack et al.52) reported a data from the National Inpatient Sample (NIS) which included 5,005 patients who underwent surgery for isolated TR during 10 years (2004–2013). During the study period, the number of TV surgery was significantly increased (from n=290 in 2004 to n=780 in 2013, p<0.001 for trend), and the in-hospital mortality rate was not changed significantly with the average of 8.8%.52) The study patients with surgery for TR had a high burden of comorbidities such as AF (49.7%), chronic kidney disease (18.9%), and liver disease (7.7%).52) Such findings suggest that: 1) the annual volume of surgery for TR is very small, being incomparable to surgery for MR (18,460 cases for a single year 2017, from the NIS database),56) 2) despite the increased number of TV surgery, it is still a stagnant field considering the explosive growth in number of TAVR owing to technical innovation (from 4,666 cases in 2012 to 72,991 cases in 2019, from the STS-ACC trans-catheter Valve Therapy Registry),57) and 3) the timing of TV surgery was inappropriately late in substantial number of patients. Kawsara et al.53) reported a large-sized clinical data of isolated TR surgery (n=1,513) from the Nationwide Readmissions Database. They reported that the in-hospital mortality rate was 8.7%, and the significant determinant factor of mortality was “late referral to surgery” (odds ratio, 4.75; 95% CI, 2.74–8.25, p<0.001), which was defined by the variables including acute decompensated HF, non-elective surgery, and advanced liver disease.53) Against the clinical data favored active implementation of surgery, there was also a contradictory viewpoint with questionable benefits of TR surgery. Axtell et al.55) reported a clinical data including total 3,276 patients with TR in whom 171 (5%) underwent TV surgery. In comparison between the surgery and medical groups, although the surgery group showed better clinical outcome in crude analysis, it was shown insignificant after a meticulous adjustment of biases.55) The authors emphasized that a period between the initial diagnosis and surgery (in which event never exist) gave a biased prognostic benefit to the surgery group, namely an immortal time bias.55)58) This is a reasonable critique for the limitations of retrospective clinical data. However, this issue should be repetitively addressed in the future.
Table 1
Summary of clinical data about surgical treatment of TR
| Authors, Year | Number | Age (years) | Female (%) | Patient enrollment | Main findings |
|---|---|---|---|---|---|
| Zack et al.52) (2017) | 5,005 | 62 (48–72) | 57 | Patients with isolated TV surgery, from the NIS database (2004–2013) | Categorized to TVr (41%) and TVR (59%). |
| In-hospital mortality rate was 8.8%. | |||||
| Number of TV surgeries were significantly increased during the study period (from n=290 in 2004 to n=780 in 2013, p<0.001). | |||||
| Kawsara et al.53) (2021) | 1,513 | 56±17 | 50 | Patients with isolated TV surgery, from the NRD (2016–2017) | Categorized to TVr (63.5%) and TVR (36.5%). |
| In-hospital mortality rate was 8.7%. | |||||
| Late referral to TV surgery was the strongest predictors of in-hospital mortality. | |||||
| Surrogates of late referral were common as decompensated heart failure (41%), non-elective surgery (44%), advanced liver disease (17%), unplanned hospitalization in prior 90 days (31%). | |||||
| Kim et al.38) (2009) | 61 | 57±9 | 89 | Patients with isolated TV surgery, from a single center (2003–2008) | Categorized to TVr (13%) and TVR (87%). |
| Operative mortality rate was 10%. | |||||
| RV end-systolic area of ≥20 cm2 and serum hemoglobin level of ≤11.3 g/dL were predictors of poor postoperative outcome. | |||||
| Kilic et al.51) (2013) | 54,375 | 65±15 | 59 | Patients with isolated/combined TV surgery, from the STS national database (2000–2010) | Categorized to isolated TV surgery (14%) and combined TV surgery (86%). |
| Categorized to TVr (89%) and TVR (11%). | |||||
| Operative mortality was significantly decreased during the study period (from 10.6% in 2000 to 8.2% in 2010, p<0.001). | |||||
| Patient characteristics changed during the study period to older age, higher comorbidity burden, and higher proportion of emergency operation. | |||||
| Vassileva et al.50) (2012) | 28,276 | 67 (54–76) | 61 | Patients with isolated/combined TV surgery, from the NIS database (1999–2008) | Categorized to isolated TV surgery (20%) and combined TV surgery (80%). |
| In-hospital mortality rate was 10.6%. | |||||
| Number of TV surgeries were significantly increased during the study period. | |||||
| Topilsky et al.54) (2011) | 189 | 67±11 | 63 | Patients with isolated/combined TVR, from a single center (1997–2007) | Categorized to isolated TV surgery (36%) and combined TV surgery (64%). |
| Operative mortality rate was 10%. | |||||
| Intra-aortic balloon pump and severe symptom (NYHA class IV) were predictors of operative mortality. | |||||
| Axtell et al.55) (2019) | 3,276 | 73±15 | 54 | Patients with isolated severe TR, from a single center (2001–2016) | Total 171 patients underwent TV surgery (5%) whereas 95% of patients received medical treatment. |
| Categorized to TVr (84%) and TVR (16%). | |||||
| There was no survival benefit of TV surgery after adjustment for immortal time bias. |
Among the present TV surgery, about 95% of cases are combined with left-side valve surgery, and 5% are targeted to isolated TR.59)60) Modes of the TV surgery are classified as TV repair (TVr) in 90% and TV replacement (TVR) in 10%.51) TVr is a current mainstream of the TV surgery, based on the concept that only reinforcement of coaptation will be sufficient to correct TR as 90% of the etiologies are secondary.17)49) TVr is classified to suture techniques such as Kay and DeVega procedures and annuloplasty using a prosthetic ring.7)17) In several previous clinical data, the suture based techniques showed higher recurrence rate of TR as 20–35%, whereas ring annuloplasty showed that of 10%.60)61)62)63) Therefore, ring annuloplasty is a current major TVr technique.17) In contrast, TVR has not been frequently performed in patients with TR from concerns of postoperative RV dysfunction and prosthetic valve-related complications.59) However, the patients with TVR in a retrospective data might represent more advanced TR with features of unfavorable leaflet morphology and severely dilated TA, and this could be a bias to the unsatisfactory clinical outcome after TVR.7)64) In a recent study comparing the patients with stand-alone TVr (n=132, 55%) and TVR (n=106, 45%), there was no significant difference in clinical outcomes (death and heart transplantation).64) However, the TA diameter was found as an effect modifier that TVR showed a better prognosis in those with TA >44 mm.64)
DILEMMA IN THE DECISION OF SURGERY
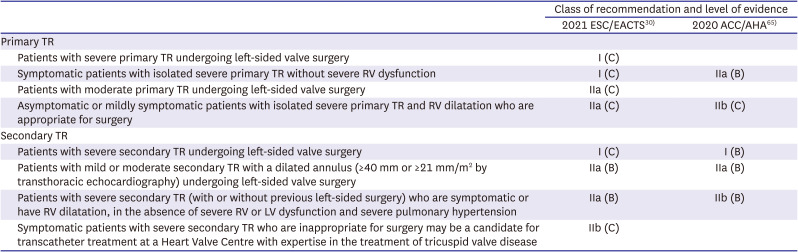
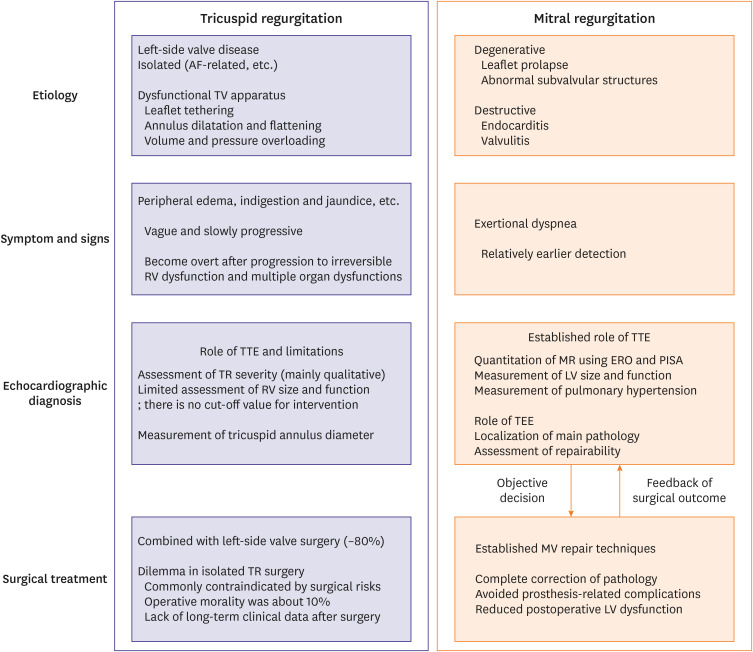
The practical reason why physicians have difficulty in the decision of TV surgery could be found in the current guidelines. The class I recommendation of surgery in the guideline is ‘presence of symptom,’ which is unclear and even it is a level of expert’s opinion (Table 2).30)65) Other surgical indications are described rather objectively according to individual clinical situations. In a patient with secondary TR who is planned to undergo left-side valve surgery, the TV surgery is recommended for severe TR (class I) or for TA dilatation (>40 mm, 21 mm/m2) regardless of TR severity (class IIa).30)65) The rationales of TV surgery combined with a left-side valve surgery are that: it does not significantly increase operative time and morbidity, and if redo surgery is required for aggravated TR after a long time, risk of surgery will be markedly increased.7)17)18)28) Therefore, major dilemma in the decision of TV surgery lies in primary TR or isolated TR. Above all, the first barrier to surgical decision for TR is high surgical mortality, reported in several retrospective studies as 8–10%.38)52)53)66) And, in a physician’s point of balancing potential risk and benefit, evidences regarding the technical completeness of surgery and long-term clinical outcome are the utmost important determinants. Although such data regarding TR is currently insufficient, it would be valuable to remind the established management flow in primary MR and gaps with the reality of TR (Figure 2). The landmark innovation in the treatment of MR was the establishment of mitral valve (MV) repair techniques which effectively corrected MV pathology and also reduced surgical morbidity.67)68)69) For the prediction of postoperative LV dysfunction, definition of surgical indications with preoperative LV ejection fraction and LV diameter was effective.70)71) And, objective surgical results could be assessed by regular follow-up of TTE in terms of recurrence of significant MR and recovery of LV function.68)72) However, situations of TR are quite different comparing to such successful history of MR treatment. First of all, the most common etiology of the TR is secondary. Even if a stable coaptation of the TV is obtained immediately after surgery, there possibly present progressive alterations in annular geometry and abnormalities in coaptation as observed in secondary MR.73)74) Because the evaluation of RV size and function by echocardiographic examinations is very limited, current guidelines do not comment on a surgical indication with that parameters.30)65) Although CMR is accepted as a standard imaging modality for the RV structure, enhancing its feasibility in routine practice is a remained mission for further development in the treatment of TR.3) Meanwhile, Kim et al.38) presented a valuable data in patients with isolated TR that routinely feasible parameters predicted poor postoperative outcome, those were RV end-systolic area of ≥20 cm2 and serum hemoglobin level of ≤11.3 g/dL. They commented that these parameters well reflected chronic wasting features of TR, and anemia and thrombocytopenia did not only mean hematologic derangements but were surrogate markers of systemic organ dysfunctions.17)38)
Table 2
Current recommendation for TR surgery in guidelines
| Class of recommendation and level of evidence | |||
|---|---|---|---|
| 2021 ESC/EACTS30) | 2020 ACC/AHA65) | ||
| Primary TR | |||
| Patients with severe primary TR undergoing left-sided valve surgery | I (C) | ||
| Symptomatic patients with isolated severe primary TR without severe RV dysfunction | I (C) | IIa (B) | |
| Patients with moderate primary TR undergoing left-sided valve surgery | IIa (C) | ||
| Asymptomatic or mildly symptomatic patients with isolated severe primary TR and RV dilatation who are appropriate for surgery | IIa (C) | IIb (C) | |
| Secondary TR | |||
| Patients with severe secondary TR undergoing left-sided valve surgery | I (C) | I (B) | |
| Patients with mild or moderate secondary TR with a dilated annulus (≥40 mm or ≥21 mm/m2 by transthoracic echocardiography) undergoing left-sided valve surgery | IIa (B) | IIa (B) | |
| Patients with severe secondary TR (with or without previous left-sided surgery) who are symptomatic or have RV dilatation, in the absence of severe RV or LV dysfunction and severe pulmonary hypertension | IIa (B) | IIb (B) | |
| Symptomatic patients with severe secondary TR who are inappropriate for surgery may be a candidate for transcatheter treatment at a Heart Valve Centre with expertise in the treatment of tricuspid valve disease | IIb (C) | ||
Figure 2
The established management flow in primary mitral regurgitation and gaps with the reality of tricuspid regurgitation.
AF = atrial fibrillation; ERO = effective regurgitant orifice; LV = left ventricle; MV = mitral valve; PISA = proximal isovelocity surface area; RV = right ventricle; TEE = transesophageal echocardiography; TTE = transthoracic echocardiography; TV = tricuspid valve.
FUTURE DIRECTIONS FOR ADVANCED TREATMENT OF TRICUSPID REGURGITATION
The balance between benefit and risk of treatment has been ever changed with the development of medicine. In recent years, there are several important clinical data regarding the preemptive surgery in patients with asymptomatic AS or MR.75)76) Therefore, treatment guidelines are also being updated according to these trends.30)65) For the development of TR treatment, the most important objectives will be minimization of surgical risk and development of risk stratification systems centered on imaging techniques. It is expected that the issue of delayed treatment decisions can be overcome through advances in multi-modality imaging and clinical evidence identifying key parameters for decision making (Figure 3). Recently, Lee et al.77) reported that a catheter-based transient TV reduction before the surgery for TR was shown to predict postoperative hemodynamic results. The current risk prediction models as EuroSCORE II78) and STS score79) are mainly focused on coronary bypass and left-side valve surgeries. Therefore, validation studies will be required whether those are effective in predicting surgical risk in patients with TR.
Figure 3
Current limitations and future directions for advanced treatment of TR.
CMR = cardiac magnetic resonance imaging; RCT = randomized controlled trial; RV = right ventricle; TR = tricuspid regurgitation; TTE = transthoracic echocardiography; TTVI = transcatheter tricuspid valve intervention.
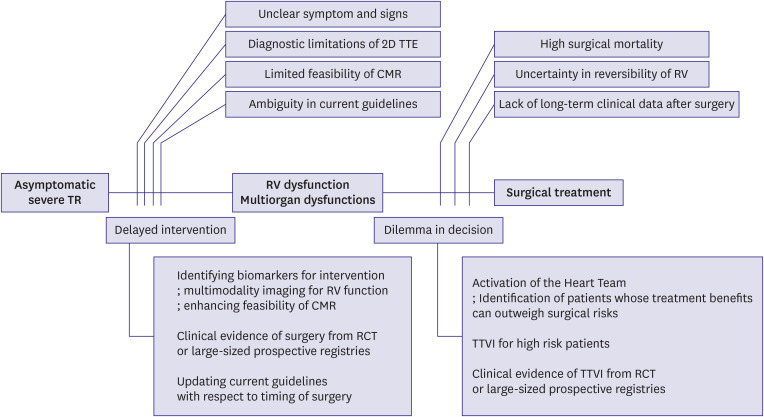
In addition, the activation of the Heart Team is highly recommended for clinical decision making in patients with severe TR and great comorbidities.30)65) This approach aims to predict the reversibility of the RV function and systemic conditions by TV surgery and to identify a group of patients in whom the treatment benefits can outweigh the risks. The Heart Team essentially includes cardiologists, cardiac surgeons, interventional cardiologists, and cardiac imaging specialists.30)65)80) Especially, it would be recommended to include HF specialists for patients with secondary TR, similarly for secondary MR.30)65) Finally, in a patient who is determined to have prohibitive surgical risks through discussions in the Heart Team, transcatheter tricuspid valve intervention (TTVI) can be recommended.30) TTVI is now in early stage of development, and the techniques are categorized to coaptation procedure, annuloplasty procedure, transcatheter TVR, and heterotopic caval valve implantation.17)49) To the present, even the largest clinical data of TTVI included less than 400 patients, and did not firmly document survival benefit and TR recurrence rate in a long-term follow-up.37)81)82)83) However, other transcatheter procedures such as TAVR and MV repair will serve as a solid basement for the development of TTVI in the future. It does not simply mean the development of catheter devices. During a recent decade, there was a great advancement in imaging diagnosis in parallel with TAVR,84) and a large number of interventional cardiologists for structural heart disease have been trained. Ultimately, in order to establish TTVI as a treatment of TR, a large-scale randomized controlled trial (RCT) will be required. However, if an implementation of large-sized RCT is seriously limited in the real world, construction of large-sized prospective registries will be an alternative which will include detailed clinical information and imaging data of TR and RV function. Also, the long-term prognosis after TTVI should be addressed, and expanded study topics such as antiplatelet and anticoagulation therapies after the TTVI should be elucidated.
CONCLUSIONS
Because there have long been problems with the diagnosis and treatment of TR, the patients with TR have been suffered from unsatisfactory clinical outcomes. Fortunately, the clinical importance of TR has been recently highlighted. To solve the current unmet needs and to improve the management of TR, we should perform further researches about TR in terms of pathophysiology, objective diagnosis with multi-modality imaging, the long-term interventional outcomes and the future treatment strategy optimized to individual patient.
 XML Download
XML Download