

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Drug-eluting stent (DES) implantation has been a mainstay in treatment of coronary stenosis worldwide owing to its safety and efficacy.1) However, restenosis, stent thrombosis, neoatherosclerosis, and abnormal vasomotion remain significant limitations related to the implanted metallic stent that contribute to device-associated cardiovascular events.1)2)3)
Drug-coated balloon (DCB) treatment was initially introduced as a novel therapeutic strategy to overcome in-stent restenosis (ISR).4)5)6) This treatment is based on the rapid delivery of highly lipophilic drugs to the inner vascular surface after balloon dilation with a unique delivery matrix.7) Proper lesion preparation is essential to overcome the limitations of the balloon angioplasty, for example elastic recoils and flow-limiting dissections.8) The 2018 European guidelines on myocardial revascularization recommended DCB treatment in patients with bare metal stent (BMS) or DES ISR lesions (class I, evidence level A).9) An all-comers, prospective, multicenter registry revealed the safety of DCB treatment and low event rates.10) The feasibility of the technique in patients with small-vessel coronary artery disease has been suggested in several pilot studies and randomized trials because the “leave nothing behind” strategy of DCB treatment showed no further reduction of the lumen by metallic struts.11)12)13)14) The Third Report of the International DCB Consensus Group has documented that a DCB-only approach in de novo lesions of coronary small-vessel disease is now a valid treatment alternative to DES if current recommendations regarding optimal balloon angioplasty and subsequent DCB delivery are adequately followed.15) However, studies on the efficacy and safety of DCB treatment in patients with de novo coronary arterial lesions are still limited by moderate numbers of patients. Therefore, we performed this Korean Stent Failure Research (SFR) group DCB registry study to evaluate the efficacy and safety of DCB treatment for ISR or de novo lesions in real-world practice.
METHODS
Ethical statement
The study protocol was approved by the Ethics Committee at each participating center and was conducted according to the principles of the Declaration of Helsinki 2013.
Study population
The SFR DCB registry is a multicenter observational retrospective registry that enrolled patients with percutaneous coronary interventions (PCIs) with DCB treatment from 18 hospitals in Korea between January 2009 and December 2017. Structured medical record review was done to assess clinical events at 12 months.
Procedure
PCIs were performed according to current clinical practice standards. DCB treatment was performed with paclitaxel-eluting balloons (SeQuent Please; B. Braun, Melsungen, Germany and Pantera Lux, Biotronik, Berlin, Germany). Coronary stenotic lesions (ISR or de novo lesions) were predilated with compliant, noncompliant, scoring, or cutting balloons. DCBs were delivered and inflated for 30 to 60 seconds with a nominal pressure. Procedural success was defined as achievement of <30% diameter stenosis without dissection or coronary perforation. Final decision concerning dual antiplatelet treatment duration, type of P2Y12 receptor inhibitors, and use of glycoprotein IIb/IIIa inhibitors was left to the physician’s discretion.
Outcomes
The primary outcome was target lesion failure (TLF) at 1 year. TLF was defined as a composite of cardiac death (CD), target vessel myocardial infarction (TVMI), or clinically indicated target lesion revascularization (TLR). Secondary outcomes were each component of TLF. Deaths were considered CD unless a noncardiac cause could be documented. Myocardial infarction was defined according to the Academic Research Consortium definition.16)
An independent clinical event adjudication committee, composed of physicians who were not involved in this study, identified and adjudicated the defined clinical events in a blinded, unbiased manner.
Statistical analysis
Categorical variables were presented as numbers and relative frequencies (percentages) and were compared using the χ2 test. Continuous variables were expressed as mean ± standard deviation and were compared using the independent-sample t test or Mann–Whitney test, as appropriate. Calculations of cumulative event rates were based on Kaplan–Meier estimates. A multivariable Cox proportional hazards model was used with backward elimination based on Akaike information criterion to identify independent predictors of TLF. All p values were 2-sided, with statistical significance set at <0.05. All analyses were conducted using R version 4.0.4 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
All patients
From January 2009 to December 2017, 2,509 patients with 2,666 DCB-treated coronary artery lesions were included. The mean age was 65.7±11.3 years, 69.9% of the patients were men, 43.1% had diabetes, 66.0% had hypertension, and 17.9% were active smokers. Mean left ventricular ejection fraction (LVEF) was 57.5±10.8%. The indication for PCI was an acute coronary syndrome (ACS) in 1,566 patients (62.4%) (Table 1).
Table 1
Baseline patient characteristics
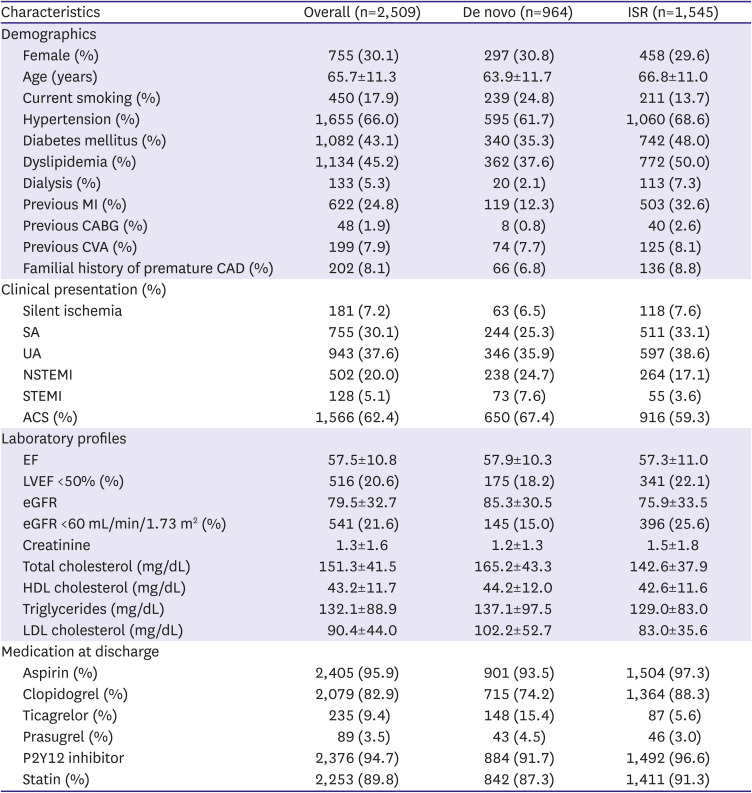
Data are presented as number/total number (%) or means ± standard deviations.
ACS = acute coronary syndrome; CAD = coronary artery disease; CABG = coronary artery bypass graft; CVA = cerebrovascular accident; EF = ejection fraction; eGFR = estimated glomerular filtration rate; HDL = high-density lipoprotein; ISR = in-stent restenosis; LDL = low-density lipoprotein; LVEF = left ventricular ejection fraction; MI = myocardial infarction; NSTEMI = non-ST segment elevation myocardial infarction; SA = stable angina; STEMI = ST segment elevation myocardial infarction; UA = unstable angina.
*Body mass index is the weight in kilograms divided by the square of the height in meters.
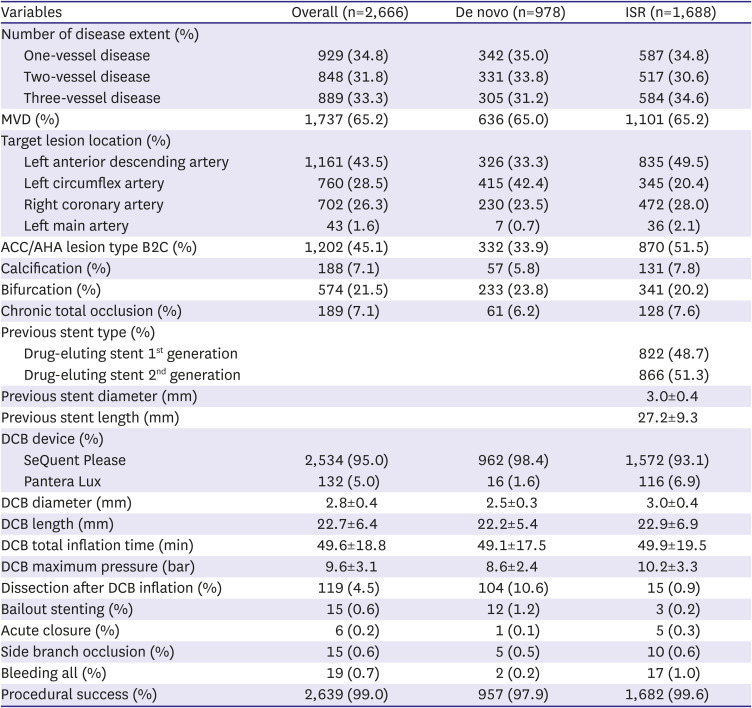
In 43.5% of the patients, the target lesion was located at the left anterior descending artery (LAD), in 28.5% in the circumflex coronary artery, and 26.3% in the right coronary artery. The SeQuent Please DCB was used in 95% of the patients and Pantera Lux DCB in 5% (Table 2). The mean length of DCBs was 22.7±6.4 mm, with a mean diameter of 2.9±0.5 mm. The mean duration of DCB inflation was 49.6±18.8 seconds. Coronary dissections and bailout stent implantation were observed in 110 (4.5%) and 15 (0.6%) patients, respectively. Procedural success rate was 99.0%. Baseline clinical and procedural characteristics of the study cohort are presented in Tables 1 and 2, respectively.
Table 2
Baseline characteristics of the lesions
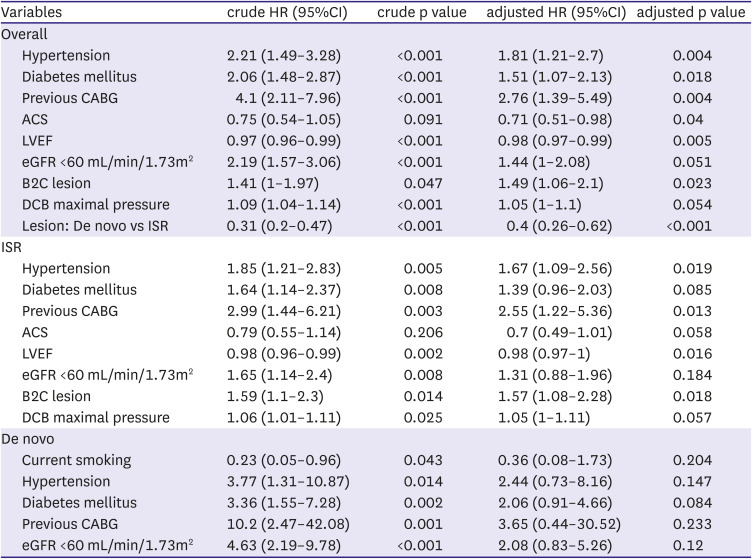
At 12 months, the primary outcome, TLF, occurred in 179 patients (6.7%); CD was observed in 43 (1.6%), TVMI in 39 (1.5%), and TLR in 137 (5.1%) patients (Table 3, Figure 1). The independent predictors of TLF in the multivariate Cox regression model are summarized in Table 4. A history of hypertension, diabetes mellitus, ACS, previous coronary artery bypass graft (CABG), reduced LVEF, B2C lesion and in-stent restenosis lesion were independent predictors of 12 months TLF in the overall population.
Table 3
Outcomes at 12 months

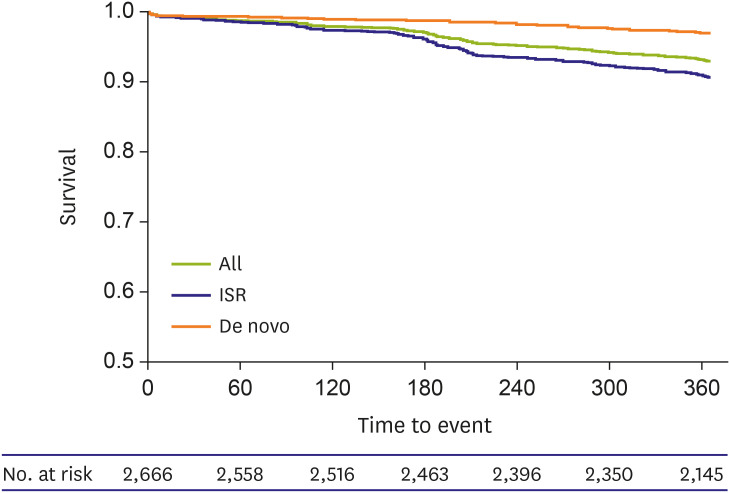
Table 4
Independent predictors of TLF
In-stent restenosis
This study included 1,545 patients with 1,688 ISR lesions. The frequency of cardiovascular risk factors was significantly higher in this group than in patients with de novo lesions except for the frequency of history of current smoking (Table 1). Eight hundred sixty-six (51.3%) of the patients with ISR lesions were treated with a second-generation DES (Table 2). The target lesions in more than half of the patients with ISR lesions were at the LAD. The diameter of the DCB was 3.0±0.4 mm and its length was 22.9±7.2 mm. The incidence of coronary dissection was 0.9% and the rate of bailout stent implantation was 0.2%.
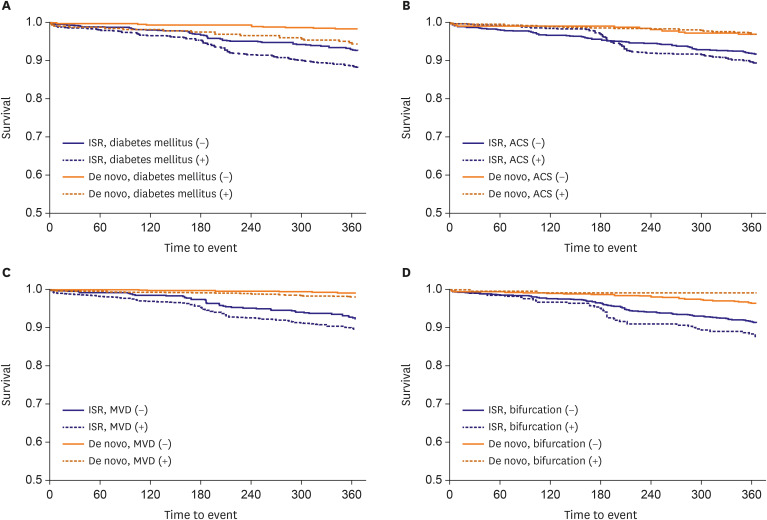
At 12 months, TLF occurred in 151 patients (8.9%); CD was observed in 33 (2.0%), TVMI in 37 (2.2%), and TLR in 160 (7.1%) (Table 3). There were no significant differences of event free survival in patient with ISR lesion according to diabetes mellitus, ACS, multivessel disease (MVD), bifurcation lesion (Figure 2). The history of hypertension, previous CABG, reduced LVEF and B2C lesion were independent predictors of 12 months TLF in patient with ISR lesions (Table 4).
De novo lesions
This study included 964 patients with 978 de novo coronary lesions. Clinical presentation was ACS in 67.4% of these patients. The target lesions were at the left circumflex coronary artery in 42.4% of the patients; 72.4% of the patients had small-vessel disease and 23.8% had bifurcation lesions (Table 2). The mean diameter of DCBs (2.5±0.3 mm) was significantly smaller in the de novo lesion group than in the ISR lesion group, whereas the incidence of coronary dissection (10.6%) and the rate of bailout stent implantation (1.2%) were higher (Table 2).
At 12 months, TLF occurred in 28 patients (2.9%); CD was observed in 10 (1.0%), TVMI in 2 (0.2%), and TLR in 17 (1.7%) (Table 3). There were no significant differences of event free survival in patient with de novo lesion according to diabetes mellitus, ACS, MVD, bifurcation lesion (Figure 2). There was no independent predictor of 12 months TLF in de novo group (Table 4).
DISCUSSION
In this large-scale multicenter Korean registry study, DCB treatment was applied to all comers with ISR or de novo coronary arterial stenotic lesions. The aim of the study was to evaluate the efficacy and safety of DCB treatment in Korean patients in real-world practice. To the best of our knowledge, this is the largest registry study to demonstrate the safety and efficacy of DCB treatment in this population, especially in patients with de novo lesions. The major findings of this study are as follows: a) DCB treatment in a real-world setting with 2,509 patients was safe and resulted in a low rate of TLF in patients with ISR or de novo lesions; b) a history of hypertension, diabetes, ACS, previous PCI, CABG, reduced LVEF, B2C lesion and ISR lesion were independent predictors of 12 months TLF in the overall study population.
DES are the most widely used devices in treatment of patients with coronary stenosis worldwide owing to their evidence-based safety and efficacy.1) Despite improvements in the ISR rates, significant limitations remain related to the persisting metallic stent.2)3)4) Drug-eluting bioresorbable vascular scaffolds (BVS) have been designed to overcome very late risks of DES.17) However, the first-generation BVS had a large strut to compensate for the insufficient radial strength of polymer materials, resulting in higher scaffold thrombosis rates than conventional DES, and was therefore expelled from the market.18) DCB are another novel concept for overcoming the limitations of DES, especially restenosis of metallic stents.4)
A large-scale registry study which included more than 2000 patients at 75 sites in 8 countries revealed the safety and efficacy of DCB treatment in real-world practice.10) The study reported that the rate of major adverse cardiac events (MACEs) was 11.6% in patients with DES ISR and 2.6% in patients with de novo lesions at a 9-month follow-up. The rate of coronary dissection after DCB treatment was 3% in patients with ISR lesions and 8.5% in patients with de novo lesions. Bailout-stent implantation was needed in only 4% of all patients. Jeger et al.12) compared the safety and efficacy of DCB with those of DES in patients with small native coronary artery disease. In this randomized trial, 382 patients were assigned to DCB and 376 to DES, and DCB was non-inferior to DES regarding MACE up to 12 months, with similar event rates in both treatment groups (DCB vs. DES: MACE, 7.5% vs. 7.3%; hazard ratio, 0.97 [95% confidence interval, 0.58–1.64], p=0.918).
Studies on the efficacy and safety of DCB treatment in East Asian populations have been limited by moderate numbers of patients. Chen et al. reported the results of The RESTORE ISR China Randomized Trial.19) In this head-to-head randomized trial, they examined only 240 Chinese patients treated with Restore DEB and SeQuent Please (120 patients per group) and revealed the acceptable efficacy and safety of both DCBs. Habara et al.20) reported the long-term safety and efficacy of DCB treatment in 468 Japanese patients with 550 ISR lesions. Late follow-up (18 months) angiography was performed for 377 (88%) of the remaining 427 lesions (excluding target lesion revascularization), and late restenosis was found in 2 lesions (2.5%) in the BMS-ISR group and 50 lesions (16.8%) in the DES-ISR group. Lee et al.21) investigated the effects of procedural optimization on the clinical outcomes of DCB treatment in patients with coronary artery disease. In this analysis, the effect of procedural optimization, including time delay to inflation defined as the delivery time of DCB from the duration between entering the guide catheter and inflation was elucidated.
The incidence of ischemic events was paradoxically lower in East Asian populations than in patients of European descent despite the high prevalence of gene polymorphisms and high on-treatment platelet reactivity in East Asians.22) Lower levels of the inflammatory marker C-reactive protein in East Asians have been observed,23) and patients of Asian/Pacific Islander descent had a 70% lower prevalence of venous thromboembolism compared to Europeans.24) Bleeding events occurred more frequently in East Asians than in Europeans treated with clopidogrel.25) This low thrombogenicity could partly explain the low incidence of ischemic events in East Asian patients.
In comparison with a previous study with the Western population, this large Korean registry study revealed a relatively low rate of events. These may be partially due to low thrombogenicity in this East Asian population.
DCB treatment in a real-world setting with 2,509 patients was safe and resulted in a low rate of TLF in patients with ISR or de novo lesions. Almost 1,000 patients with de novo coronary lesions were enrolled in this registry study and the mean diameter of DCB was very small (2.5±0.3 mm), whereas previous studies specifically focused on patients with small de novo coronary lesions and were limited by moderate numbers of patients. The incidence of TLF in patients with de novo coronary lesions was low. This finding from large registry data suggests that DCB treatment in patients with small de novo lesions is effective and safe; this result has been well elucidated by various lines of clinical evidence. Considering the efficacy of the DCB-only treatment in small coronary arteries, the treatment of de novo lesions in large coronary arteries seems to be both safe and efficient and the evidence for this is growing. To overcome significant limitations of DES, DCB studies in patients with large de novo coronary lesions seem to be essential. Emerging areas of interest also include drugs other than paclitaxel, the use of physiologic assessment to guide DCB treatment, and DCB use in primary PCI.
There are several limitations to our study. This analysis was based on retrospective, nonrandomized registry data. A comparison with a control group is not possible with such design. Patients and lesions included in this registry were selected, as indicated by ISR, de novo small vessel lesions, and acceptable results of balloon angioplasty. Therefore, the results of this study cannot be generalized to all patients scheduled for coronary intervention. There was no angiographic core lab and qualitative comparative analysis data were not available. Therefore, some important lesion characteristics, for example pre and post reference vessel diameter, lesion length, lumen diameter, and acute gain could not be analyzed, and the frequency and impact of geographic miss cannot be reported. The impact of procedural factors on the occurrence of TLF was not elucidated in this study. The number of TLF events in the de novo group is small, so the predictive power was weak and no independent predictor was found in this group.
In conclusion, this large multicenter DCB registry study revealed the favorable clinical outcome of DCB treatment in real-world practice in patient with ISR lesion as well as small de novo coronary lesion. Further prospective studies are warranted to confirm the current analyses and define the role and safety of DCB treatment in large de novo coronary artery lesions.
 XML Download
XML Download