

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of death in Asia with increasing mortality owing to the combined impact of population aging, increasing epidemics of major risk factors, insufficient implementation of effective strategies in both primary and secondary prevention and residual risk from emerging risk factors.1) Dramatic efforts have been made to alleviate the harms to public health caused by CVD with surging activities and substantial progression made in CVD clinical research in many countries and regions of Asia, especially Eastern Asia.2) In recent decade, China, Korea, and Japan have initiated or joined more multicenter randomized controlled trials (RCTs) than in the previous decade. According to the data provided by ClinicalTrial.org of the National Institutes of Health in the United States, among 2305 phase III RCTs conducted in the cardiovascular field from 2011 to 2021, the numbers of RCTs involving China, Korea and Japan were 281, 231 and 201 respectively, approximately two times increase compared with the numbers from 2000 to 2010.3) Pragmatic clinical studies have also increased in these countries, including randomized or nonrandomized pragmatic clinical trials and observational studies (including registry studies) to assess the comparative effectiveness and safety of a wide range of management strategies of major CVDs in clinical practice. In the past 10 years, the importance of pragmatic clinical studies in evidence-based medicine (EBM) practice has been increasingly recognized as a source of evidence that is more applicable to the patients in which the intervention will be applied.4)5)6) Pragmatic clinical studies for CVD, initiated or conducted jointly by Asian countries have provided important evidence to support decision making for patients in clinical practice.7)8)9)10)11)12)13)14)
In this review, we aimed to describe the evolution of the conceptual framework of pragmatic clinical studies, share perspectives on the importance of pragmatic clinical studies for CVDs as a complement to conventional RCTs, as well as highlight the specific importance of pragmatic clinical research in improving evidence-based practice for CVD managements in Asia.
EVOLUTION OF THE CONCEPT OF PRAGMATIC CLINICAL STUDIES
The original concept of the pragmatic clinical study in therapeutic trials was proposed by two French statisticians, Schwartz and Lellouch, in a paper published in 1967 entitled “Explanatory and Pragmatic Attitudes in Therapeutical Trials.15) This paper was republished in 2009.16)
The authors of this article coined the term “pragmatic” and provided persuasive arguments for the differences between a pragmatic approach and an explanatory approach in therapeutic trials, as well as the importance of a pragmatic approach in clinical decision making for patients in daily practice. The concept was well summarized later by Sackett,17) as follows: “Pragmatic trials are primarily designed to determine the effects of an intervention under the usual conditions in which it will be applied, whereas explanatory trials are primarily designed to determine the effects of an intervention under ideal circumstances.” A Consolidated Standards of Reporting Trials (CONSORT) document “Improving the reporting of pragmatic trials: an extension of the CONSORT statement.” was published in 2008. This document provided simple comparisons of the characteristics of pragmatic trials and explanatory trials and added eight specific requirements to the reporting of pragmatic trials, based on original CONSORT checklist.18) Later, the concept of pragmatic study was further developed since differences between pragmatic trials and explanatory trials are multidimensional rather than dichotomy. In 2009, Thorpe et al.19) developed a tool called PRECIS (Pragmatic–Explanatory Continuum Indicator Summary) to describe multidimensional features of pragmatic trial or explanatory trial. PRECIS was updated to PRECIS II in 2015.20) The PRECIS II provided a more practical tool for the design of pragmatic trial and pragmatic clinical studies. According to PRECIS II criteria, trials can be classified into five grades from very explanatory to very pragmatic, using different strategies in nine domains of trial design, including eligibility, recruitment, setting, organizations, flexibility in delivery, flexibility in adherence, follow up, primary outcomes, and primary analysis. Table 1 provides the features of pragmatic trials in the nine domains.20) Obviously, the conceptual framework of pragmatic trials in PRECIS II covers a wider range of clinical trials designs with a combination of pragmatic and explanatory features, even covering the trials based on observational cohort studies.
Table 1
The features of pragmatic clinical study and factors reduced the extent of pragmatic approach in 9 domains of study design*
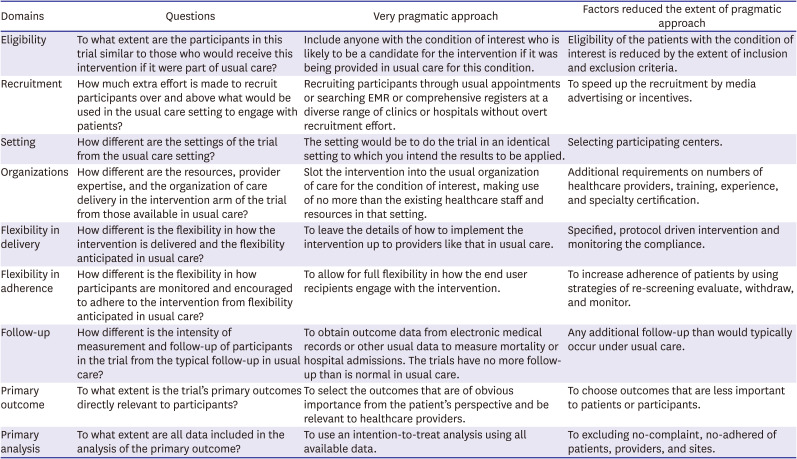
*Extracting from PRECIS II (Pragmatic–Explanatory Continuum Indicator Summary).20)
One of the underlying drivers of the evolution of pragmatic clinical studies may be the real-world clinical data with extensive coverage for inpatients and outpatients become widely available in electronic medical records (EMR), as well as the increasing feasibility of tracking the long-term outcomes of patients by interlinking medical insurance databases and death registry system databases.21)22) More importantly, rapid development of artificial intelligence (AI) in big data science and technology has promoted improvement in clinical data, which would strongly support the advancement of pragmatic clinical studies.23)
With increasing clinical trials using data of EMRs or other electronic health records to identify eligible patients, to deliver an embedded intervention, to identify trial outcomes, or a combination of these purpose, a new checklist in the CONSORT extension for the reporting of RCTs conducted using cohorts and routinely collected data (CONSORT-ROUTINE) was published in 2021.24) This document provides new standards for the reporting of the pragmatic clinical trials conducted using cohorts or routinely collected data.
These documents reflect the evolution of the concept of pragmatic clinical studies, from dichotomous to multidimensional with more comprehensive coverage regarding study types and designs.
THE IMPORTANCE OF PRAGMATIC CLINICAL STUDIES AS A COMPLEMENT TO EXPLANATORY RANDOMIZED CONTROLLED TRIALS IN EVIDENCE-BASED PRACTICE
In the past 30 years, EBM has replaced the old paradigm of empirically based medicine to become the mainstream medical paradigm in health care worldwide.25)26) As originally proposed by Dr. Guyatt, the paradigm of EBM referred to practice integrating best evidence, medical expertise, and patients’ values.27) The definition of EBM practice was further defined by Sackett et al.28) in 1996 as follows: “The practice of EBM means integrating individual clinical expertise with the best available external clinical evidence from systematic research. By individual clinical expertise we mean the proficiency and judgment that individual clinicians acquire through clinical experience and clinical practice.” The original concepts of EBM and EBM practice clearly imply the importance of evidence from pragmatic clinical studies in EBM practice. Indeed, it is not easy to judge where a treatment is suitable for an individual patient without combined evidence from both explanatory RCTs which evaluate the efficacy and safety of an intervention in selected patients under strictly controlled implementation environments, and pragmatic studies, which evaluate effectiveness and safety of an intervention in a largely unselected population of patients that received the intervention in real clinical practice. However, the EBM is often understood as explanatory RCT-EBM. In many countries, including Asian countries, a comprehensive system has been well established to support explanatory RCT-EBM practice. The system includes the following: 1) Regulatory processes for new products for medical treatment: explanatory RCT-based evidence is often a mandatory condition for approving new drugs or new interventional devices; 2) Clinical guidelines: the strength of recommendations for disease managements in clinical practice guidelines is based on the availability of explanatory RCT studies and systematic reviews of these RCTs26)29); 3) Quality of care assessment: the utilities of treatment strategies with evidence from RCTs often are used as indicators of performance measures in clinical practice30)31); 4) Publication: explanatory RCT studies are highly prioritized for acceptance by high quality journals. It is true that high quality randomized double-blind controlled clinical trials can provide an unbiased evaluation of efficacy and safety under experimental conditions. In fact, high-quality explanatory RCT studies are pivotal in the EBM paradigm and are often synonymous with best evidence.
However, there are increasing concerns regarding the limitations of explanatory RCTs.32)33) The following three core issues may explain the growing demands for pragmatic clinical studies as a complementary source of evidence to guide clinical practice for CVD.
The external validity of explanatory randomized controlled trials for patients with cardiovascular disease in clinical practice
A considerable number of studies and systematic reviews have reported lower representatives and questionable external validity of the evidence from at least some RCTs on interventions for CVD and other diseases.34)35)36)37)38)39)40) One study compared baseline characteristics and outcomes between patients recruited from a clinical registry and patients from 14 RCTs that evaluated the efficacy and safety of percutaneous coronary intervention (PCI) compared with coronary artery bypass graft. The study found that only 36% of the patients from clinical practice met the inclusion criteria of these RCTs.38) Another study compared the baseline characteristics and clinical outcomes of patients enrolled in a RCT (BIOSCIENCE trial) with patients included in the CARDIOBASE Bern PCI Registry in the same hospital. The study reported that non-participants in the RCT had a higher risk profile, with more women, older peoples, multiple morbidities and adverse prognoses, as compared with RCT participants.39) A large study examined the representativeness of antihypertensive drug trials. Among 110 RCTs on renin-angiotensin aldosterone system (RAAS) drugs, 90% (99 RCTs) of the trials recruited patients under 60-year-old, and 10% (11 RCTs) recruited older patients, defined as those aged ≥60 years. The incidence rates of serious adverse events (SAEs) in both the RCTs including older patients, and RCTs without older patients were compared with the incidence rates of SAE in a large number of patients with hypertension using RAAS drugs in real clinical practice by age and sex. Community-dwelling patients with hypertension had a significantly higher risk of SAE than patients in the above two types of RCT. The standardized ratio of SAE, after adjusting for age and sex, was 4.76 times higher than the RCTs including older-patients and 4.23 times higher than the RCTs with younger patients. The authors of that paper stated that the study results suggest “even accounting for age and sex, participants in hypertension trials and people with hypertension in the community are very different populations.”40) A recently published systematic review further addressed this issue. That systematic review reported estimated exclusion rates of clinical patients from 305 trials of treatments for 31 physical conditions. The median total exclusion rate was 77.1% of patients. Median exclusion rates for trials of common chronic conditions were high, including for hypertension (83.0%), type 2 diabetes (81.7%), chronic obstructive pulmonary disease (84.3%), and asthma (96.0%). The most frequently applied exclusion criteria were related to age, co-morbidities, and co-prescribing.41)
Evidence gaps for clinical questions in cardiovascular disease management
Several studies have revealed large evidence gaps for major clinical questions in CVD. One study examined the levels of evidence for 6,329 recommendations in 51 current guidelines of the American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology (ESC). Among 2,930 recommendations in ACC/AHA guidelines, 8.5% was classified as level A, 50% level B and 41.5% level C evidence. In 3,399 recommendations of ESC guidelines, 14.2% was classified as level A, 31.0% level B, and 54.8% level C evidence.40) The study compared the current guidelines with prior versions; the proportions with level A evidence showed no increase in either ACC/AHA (median, 9.0% [current] vs. 11.7% [prior]) or ESC guidelines (median,15.1% [current] vs. 17.6% [prior]). The authors of that study concluded that “among recommendations in major cardiovascular society guidelines, only a small percentage were supported by evidence from multiple RCTs or a single, large RCT. This pattern does not appear to have meaningfully improved from 2008 to 2018.”42) Other studies have presented similar results regarding the quality of evidence in the guidelines for atrial fibrillation.43) The authors of these studies appealed for the development and implementation of inexpensive methods to generate a large volume of evidence. These studies highlight the need for pragmatic clinical studies evaluating the comparative effectiveness of existing treatments, and novel methods of conducting clinical trials with less waste.
The quality of evidence from pragmatic clinical studies
It is a key question whether pragmatic clinical studies can provide reliable evidence or evidence comparable to explanatory RCTs. A good example of a pragmatic randomized clinical study for CVD intervention is TASTE (The Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia) trial. This study aimed to evaluate whether thrombus aspiration reduces mortality. The results of that registry-based clinical trial were published in The New England Journal of Medicine in 2013.44) The TASTE trial provided an example of combining the benefits of randomized treatment assignment with the best features of a large-scale clinical registry. This RCT/pragmatic clinical trial demonstrated some of the most important advantages of pragmatic trials, namely broad inclusion criteria to ensure wide clinical applicability, a simplified enrollment process to maximize the commitment and compliance of participating hospitals, and a substantial reduction in the expense associated with conducting a RCT. The study results have become important evidence in relevant guidelines.45)
The important RCT DUPLICATE initiative has been launched to emulate RCT with nonrandomized real-world study (RWS). The first report was published in 2021 on the first 10 trial emulations, evaluating CVD outcomes of anti-diabetes or antiplatelet medications.46) The researchers used patient-level claims data with the same inclusion and exclusion criteria. The intervention group and control group were matched using propensity scores to control for more than 120 pre-exposure confounders. The study found that the regulatory conclusions were equivalent in 6/10 trials; the effectiveness estimation, indicated using the hazard ratio (HR) was within the 95% confidence intervals of HRs from the corresponding RCT in 8/10 studies.46) Whereas the results of that study do not mean that an observational study based on routine clinical data can replaced a RCT, the findings at least provide an evaluation of comparability and differences in the effects and safety of certain intervention between pragmatic clinical studies and RCTs.
The importance of pragmatic clinical studies in evidence-based practice for CVD is obvious and may increase with further development of AI technology. It has become possible to evaluate and provide feedback more comprehensively and relatively rapidly using more pragmatic approach for issues of effectiveness and safety in clinical practice for any treatment or diagnostic strategy to support judgments with expertise and the patients’ values. Furthermore, the evidence produced using routine clinical data denoted real world evidence has greater extrapolations and lower costs and has been accepted by regulatory agencies of medical products in some countries, including in Asia.47)48)49) It is critical to emphasize that the evidence from pragmatic clinical studies is not dispensable but essential to guide clinical practice.
SPECIFIC NEEDS FOR PRAGMATIC CLINICAL STUDIES OF CARDIOVASCULAR DISEASE IN ASIA
Among all deaths from CVD, 58% of CVD deaths have occurred in Asia, with specific epidemic characteristics regarding the subtypes of CVD. Asia has a very large number of patients with one or more CVD risk factors, such as hypertension, dyslipidemia, diabetes, and established CVDs, including stroke and coronary heart disease (CHD), heart failure and atrial fibrillation (AF).1)50) Most patients with CVDs or risk factors require clinical treatments. Unfortunately, most RCTs in the field of CVD have included no or few patients from Asia.
Table 2 shows a comparison of the numbers of completed RCTs globally classified by the types of CVDs or risk factors and treatment strategies, with the corresponding numbers of RCTs joined by regions of Asia.3) For example, among 177 RCTs for PCI in patients with CHD, 33 (19%) included patients from East Asia, 14 (8%) included patients from South-east Asia and 9 (5%) included patients from South Asia; Among 69 RCTs for anticoagulant treatments in patients with AF, 24 (35%) included patients from East Asia, 11 (16%) included patients from South-east Asia and 9 (13%) included patients from South Asia.
Table 2
Comparison of the numbers of completed RCTs globally with the numbers of RCTs jointed by Asian regions*
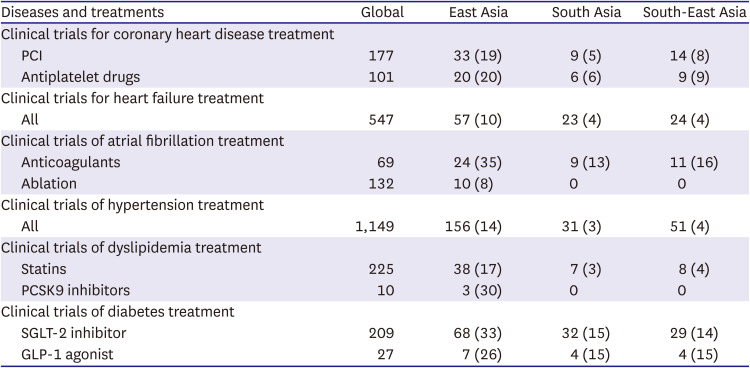
Values are presented as number (%).
RCT = randomized controlled trial.
*Data are obtained from ClinicalTrial.org of the National Institutes of Health in the United States. https://clinicaltrial.gov.3)
However, available evidence shows that Asian patients have specific effectiveness and safety issues with certain medical treatments recommended by clinical guidelines of the US or Europe based on evidence of RCTs with few or no Asian patients.
A series of expert consensuses, position statements and reviews have highlighted the differences in anti-ischemic effectiveness and bleeding risk of antithrombotic therapies between East Asian patients and White patients.51)52)53)54) The first expert consensus on this issue was the World Heart Federation (WHF) expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. This document, published in 2014, clearly indicated that the recommendations on antiplatelet therapy of the ACC/AHA and ESC guidelines were based primarily on large, phase III, randomized, controlled trials of the P2Y12 inhibitors clopidogrel, prasugrel, and ticagrelor. However, few East Asian patients were included in the trials conducted to assess the use of these agents. East Asian patients have differing risk profiles for both thrombophilia and bleeding compared with White patients, and a different ‘therapeutic window’ of on-treatment platelet reactivity might be appropriate in East Asian patients. The WHF produced this expert consensus statement to determine the antiplatelet treatment strategies that are most appropriate for East Asian patients.51) An updated expert consensus was published in 2020, in which, the issues regarding East Asian patients having reduced anti-ischemic benefits and increased bleeding risk with antithrombotic therapies as well as relevant strategies for East Asian patients, were further addressed.53)
One review by Cho well summarized the challenges regarding Asian patients with nonvalvular atrial fibrillation (NVAF) of using evidence from RCTs on non-vitamin K oral anticoagulants (NOACs) that were conducted among on predominantly non-Asian patients with NVAF.55) According to that review, the FDA emphasized the results of the RE-LY study showing that the dabigatran 150-mg dose was superior to warfarin for efficacy and similar for bleeding. But two Asian studies found that a fixed dose of 110 mg might be sufficient based on the comparable efficacy and favorable safety to 150-mg dose. Whereas the optimal doses of other agents NOACs in Asian population are uncertain, several real-world studies have provided pragmatic evidence that a reduced dose is associated with a significantly lower risk of stroke, major bleeding, intracranial hemorrhage, and mortality. Pharmacokinetic studies in Japan estimated that a 15 mg dose of rivaroxaban in Japanese patients was pharmacokinetically equivalent to a 20-mg dose in White patients.56) Another review reported that intracranial hemorrhage is a major concern in selection and dosing of NOACs among Asians because the risk of intracranial hemorrhage, the most devastating complication, was higher in Asians than in non-Asians and greater in patients with prior stroke/transient ischemic attack than in those without.57)
Some studies have also found high effectiveness and a high risk of adverse effects with statins in Asian patients.58)59) Therefore, only medium dose statins are recommended for CVD patients or patients with high CVD risk in the clinical guidelines issued by some Asian countries, such as China.60)
The cost-effectiveness of a treatment is critically important for many low- and middle-income countries. Asian countries need to conduct more comparative effectiveness studies and cost effectiveness studies based on EMR to help in decision making regarding clinical applications of old medications or new treatment strategies.61)
CHALLENGES OF PRAGMATIC CLINICAL STUDIES IN ASIA
Compared with the well-established theoretical and practice system of explanatory RCTs over the past nearly 70 years, pragmatic clinical studies remain a developing discipline with an incomplete theoretical and practice system.62)
Unclear scope and terminology
Just like at the beginning of any new sub-discipline in clinical research, the scope of the concept of pragmatic clinical studies is not well defined. Some researchers have considered pragmatic clinical studies to only include pragmatic RCTs, whereas others consider that pragmatic clinical studies also cover registry studies, as well as prospective or respective patient cohort studies in a clinical setting.6)24)63) Some reports have used the term RWS as an umbrella term covering pragmatic clinical studies.6) There is also some overlap in the scope of the conceptual framework between pragmatic clinical study and outcome studies, and comparative effectiveness research. It is important to conduct more systematic carding to clarify the current knowledge and rationality regarding the scope of pragmatic clinical studies, and develop unified definition, classification, and terminology for this emerging subdiscipline of clinical research.
Accessibility and quality of electronic medical records
Some common problematic issues and barriers exist to the use of EMR in pragmatic clinical research. One paper summarized all large EMR databases in China. However, the accessibility of these EMR databases was very low. Additionally, the availability of information necessary for clinical research is much lower than that in the United States and Europe.64) Other barriers to the use of EMR in pragmatic clinical studies include funding, ethical issues, and data quality including accuracy, completeness, and consistency.63)64)
Residual confounding effects in observational cohort studies
Whereas some pragmatic clinical studies use randomization methods to assign participants to an interventional group and control group, many pragmatic clinical studies used non-randomization or observational approaches to assess the comparative effects of an intervention strategy. When patients in the intervention and control groups are not assigned randomly, one main issue is how to ensure comparability between those patients that receive an intervention and those who did not. The risk of bias is sometime high for non-randomized pragmatic studies because the observed effects or the safety of an intervention may be affected by confounding factors.65) Certain methods are recommended to increase the comparability in observational cohort trials, including propensity score matching, inverse probability weighting and using instrumental variables et al.66)67)68)
CONCLUSIONS
Pragmatic clinical studies, as an emerging clinical research discipline, include a wide range of studies that are largely embedded with routine clinical practice aiming to evaluate comparative effectiveness and safety of different clinical intervention strategies. To increase awareness of the importance of pragmatic clinical studies in EBM practice for CVD in Asia, we described evolution of the conceptual framework of pragmatic clinical studies, from a dichotomous “pragmatic or explanatory” concept to an emerging clinical research discipline with multidimensional features and a comprehensive scope. A considerable number of studies support pragmatic clinical studies as an indispensable source of evidence in EBM practice because the evidence is more applicable to the patients in which the intervention will be applied. It is particularly important to increase the number of pragmatic clinical studies on CVD conducted in Asia because most of available evidence from explanatory RCTs has included no or few Asian patients. However, the available evidence shows there are considerable racial differences in the effects and safety of certain interventions between Asian and non-Asian patients. Clearly, it is not feasible to identify potential racial differences by repeating all explanatory RCTs that included no or few Asian patients in re-conducted RCTs among Asian population. Furthermore, as a continent mainly comprising low- and middle-income countries, Asia needs more cost-effective studies based on pragmatic clinical studies. Despite the many challenges and barriers, we expect that pragmatic clinical studies will continuously develop and become a mature sub-discipline of clinical research in Asia and worldwide.
 XML Download
XML Download