

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is one of the most prevalent atrial tachyarrhythmia which is associated with disabling symptoms, impaired quality of life, ischemic stroke, heart failure, and increased all-cause mortality.1)2)3) The AFFIRM trial investigated the impact of antiarrhythmic drugs compared to rate control strategy to treat AF which found no benefit.4) However, post hoc analysis of AFFIRM trial revealed that overall survival was significantly better in patients who maintained sinus rhythm.3) Radiofrequency catheter ablation (RFCA) proved to be superior compared with antiarrhythmic drugs in maintaining sinus rhythm and is also free from side effects of antiarrhythmic drugs such as bradyarrhythmia and pro-arrhythmic effects.5)6)7) Furthermore, improvement in the overall survival was observed in subset of patients.8)
In recent days, RFCA has become a treatment of choice especially in symptomatic AF patients refractory to antiarrhythmic drugs. Although maintenance rate of sinus rhythm is significantly higher in RFCA than antiarrhythmic drugs, the absolute success rate of RFCA is still not satisfactory especially when AF is non-paroxysmal.9)10) Prior studies also demonstrated that patients with significant amount of low voltage zones (LVZs) are at risk of arrhythmia recurrence after RFCA.11)12)13) Furthermore, ablation of LVZ may reduce arrhythmia recurrence after RFCA according to previous studies.11)14)
The presence of LVZ in left atrium (LA) is a marker of atrial substrate.14) Fibrofatty infiltration into LA myocardium and consequent scar change is assumed to cause voltage decrease in LA.15) Recent technical advancements are enabling precise and quantitative measurements of LVZ. However, the predictive value of LVZ as compared to LA diameter, a traditional and most reliable predictor of recurrence after RFCA, is not fully determined.10) We performed this analysis to compare the predictive value of LA electrical (LVZ) vs. structural (LA diameter) remodeling.
METHODS
Ethical statement
The protocols of this specific study were approved by the Institutional Review Board of Korea University Medicine Anam Hospital (approval number: 2020AN0165). Written informed consent form was waived due to the retrospective nature of this study. We followed the ethical guidelines of the 2013 Declaration of Helsinki in all study protocols.
Patients
We screened all AF patients who underwent de novo RFCA in Korea University Medicine Anam Hospital from June 1998 to April 2019. Patient who underwent a voltage mapping were finally enrolled in this study.
Ablation procedure
Multi-polar catheters were positioned at high right atrium, low right atrium, distal coronary sinus, and right ventricle. Double trans-septal punctures were performed with 2 SL1 sheaths. From February 2019, deflectable sheaths were available and used based on the operator’s discretion. Three dimensional electroanatomic mapping was performed with NavX (St. Jude Medical, St. Paul, MN, USA) system.
Elimination of pulmonary vein (PV) and extra-PV triggers was the end-point of the procedure in paroxysmal AF patients. However, additional substrate modification to achieve non-inducibility was also performed based on the operator’s discretion. For substrate modification in non-paroxysmal AF, AF was induced after completion of PV isolation. If sustained AF (AF lasting more than 5 minutes) was induced, additional substrate modifications including linear ablation and complex fractionated atrial electrogram guided ablation were performed. During the study period, LVZ-guided ablation was not performed in our institution. The precise RFCA protocols of our institution in AF patients are reported in our previous studies.10)16)17)
Electroanatomic mapping
After double trans-septal punctures and insertion of ablation and mapping catheters, direct-current cardioversion was performed if the rhythm status was AF. Three-dimensional geometry and voltage mapping were performed under paced rhythm unless incessant triggers were observed. Since sinus rate differs among patients, we paced high right atrium with a pacing cycle length of 600 msec in all patients during voltage mapping. The AFocus II circular mapping catheter was used to construct 3-dimensional geometry and acquire bipolar voltage of each point in LA. During electroanatomic mapping, LA surface area (mm2), LVZ area (mm2), LVZ percentage ([LVZ area/LA surface area]×100) were measured. The area beyond PV and LA appendage (LAA) ostium were not included in the measurement.
Echocardiography
Prior to RFCA, transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) were performed. Diameter of LA was measured in parasternal long-axis view in TTE evaluation. Other parameters such as ejection fraction of left ventricle (LV), mitral valve inflow velocity (E), mitral annular tissue velocity (e′), and valve functions were also measured. During TEE evaluation, emptying, filling, and the average flow velocity of the LAA were measured. Spontaneous echo-contrast (SEC) and thrombus in LA or LAA were carefully evaluated with multiple views (high esophageal 0º, 45º, 60º, and 120º views) during TEE evaluation. The grade of SEC was divided into 4 stages: very mild (minimal echogenicity, only detectable transiently, or increasing gain setting required for the detection); mild (detectable without increasing gain setting); moderate (dense, swirling echogenic material, echogenic signal is dense in LAA compared to LA); or severe (dense, swirling echogenic material, echogenic signal is equivocal in LAA and LA). Dense SEC was defined as moderate or severe SEC.
Definitions
Atrial tachyarrhythmia referred to both AF and atrial tachycardia (AT). Any atrial tachyarrhythmia lasting for more than 30 seconds or documented in 12-lead surface electrocardiogram (10 seconds) 90 days after RFCA was defined as late recurrence (LR). AF was classified as paroxysmal if AF episodes did not last for more than 7 days. Non-paroxysmal AF was defined as AF lasting for more than 7 days or if it required direct-current cardioversion to terminate. LVZ was defined as area in LA in which bipolar voltage range ≤0.5 mV. Substrate modification was defined as any additional ablation lesion other than PV isolation or cavotricuspid isthmus ablation.
Detection of recurrence
Patients were discharged 2 days after RFCA. All patients were recommended to come to our outpatient clinic 2 weeks after discharge to check rhythm status and symptoms. Three months after RFCA, all patients underwent Holter evaluation for 24 hours. Additional Holter monitoring was performed 6, 9, and 12 months post-RFCA. Patients were advised to take portable event recorders whenever they experience symptoms suggestive of recurrence which was not detected by Holter monitoring. Symptom-based standard 12-lead electrocardiography, whether from our or another hospital was also an important part of recurrence detection process. The freedom from LR was calculated for 5 years of follow-up.
Statistical analysis
Continuous variables are described as mean ± standard deviation and unpaired t-test was used for comparison. Analysis of covariance with post hoc Bonferroni correction was used to compare means of multiple groups. Categorical variables are expressed as percentile value and χ2 or Fisher's exact test was used as appropriate. Freedom from LR was depicted using Kaplan-Meier survival curve analysis, and a log-rank test was applied to compare the difference between groups. Multivariable Cox regression analysis was performed to compare freedom from LR while controlling the influence of covariates. Variables that was statistically different according to LVZ area group were selected to be included in the multivariable model. Hazard ratio and its 95% confidence interval (CI) were calculated for each independent variable. Known risk factors for recurrence after RFCA in AF patients were also included in the model.18) Variation inflation factor was calculated to evaluate multicollinearity among covariates included in the multivariate model. The area under curve (AUC) of LA diameter and LVZ to predict LR was calculated by receiver operating characteristic curve analysis. The AUC of LA diameter and LVZ was compared by statistical method reported by Hanley and McNeil.19) Statistical significance was defined as p value <0.05 on a 2-tailed test. All statistical analyses were performed using IBM SPSS Statistics software, Version 24.0 (IBM, Armonk, NY, USA).
RESULTS
Patients
Figure 1 summarizes the flow of this study. From June 1998 to April 2019, a total of 3,120 patients underwent de novo RFCA in Korea University Medicine Anam Hospital. Male patients consisted 78.9% of the entire cohort. Mean age and CHA2DS2-VASc score were 55.74±10.96 and 1.27±1.26, respectively. Non-paroxysmal AF was diagnosed in 40.9% of patients. Detailed baseline characteristics of our RFCA cohort are summarized in our prior reports.10)20)
Figure 1
Flow of the study.
LA = left atrium; LVZ = low voltage zone; RFCA = radiofrequency catheter ablation.

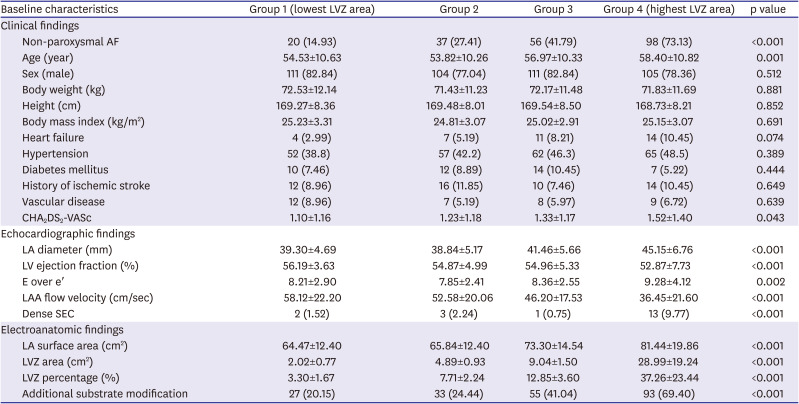
During electroanatomic mapping, 537 patients underwent LVZ mapping with AFocus II catheter. TTE was performed in all 537 patients and TEE in 532 (99.1%) patients. Baseline clinical, echocardiographic, and electroanatomic characteristics are described in Table 1. In brief, mean age, CHA2DS2-VASc score, and LA diameter were 55.93±10.65, 1.30±1.24, and 41.18±6.14, respectively. Non-paroxysmal AF was diagnosed in 211 (39.29%) patients. Patients were classified into quartiles based on LVZ area. Differences in baseline characteristics among these 4 groups are described in Table 2. Patients with high amount of LVZ had significantly higher prevalence of non-paroxysmal AF and dense SEC; greater LA diameter; lower ejection fraction of left ventricle and LAA flow velocity; and were older. The results of the statistical comparison between each subgroup are described in Supplementary Table 1.
Table 1
Baseline characteristics of the study population
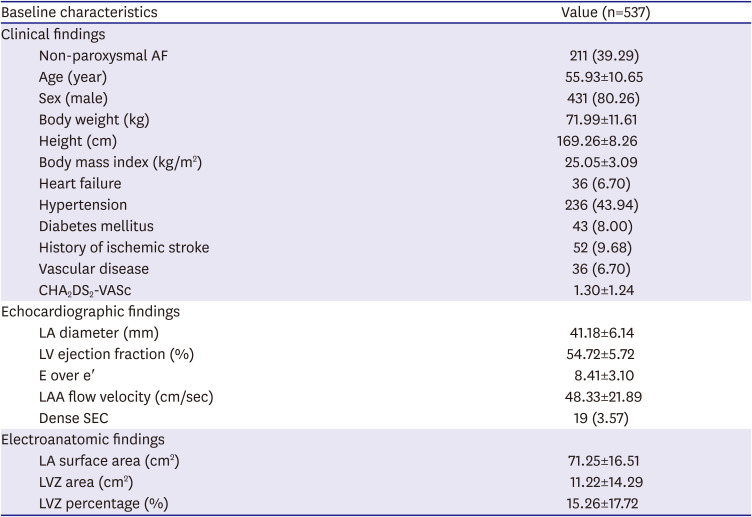
Table 2
Baseline characteristics according to LVZ area
Association between low voltage zone and echocardiographic findings
The diameter of LA differed significantly according to LVZ area (p<0.001; Figure 2A). Patients with group 1 (lowest LVZ area; 39.30±4.69 mm) and group 2 (38.84±5.17 mm) had significantly small LA diameter compared with group 3 (41.46±5.66 mm) and group 4 (highest LVZ area; 45.15±6.76 mm). No difference was observed between group 1 and group 2 (p>0.999). The flow velocity of LAA declined significantly as LVZ area increased (p<0.001; Figure 2B).
Figure 2
Association between LVZ and echocardiographic findings. (A) Difference in LA diameter according to LVZ area quartile. (B) Difference in LA diameter according to LVZ percentage quartile. (C) Difference in LAAFV according to LVZ area quartile. (D) Difference in LAAFV according to LVZ percentage quartile.
LA = left atrium; LAAFV = left atrial flow velocity; LVZ = low voltage zone.

The diameter of LA was significantly larger in patients with highest LVZ percentage (p<0.001; Figure 2C). However, no significant differences were observed among group 1 to 3 in post hoc analysis (Figure 2C). The flow velocity also differed according to LVZ percentage with group 4 (highest LVZ percentage) having lowest LAA flow velocity (p<0.001; Figure 2D).
Freedom from late recurrence
The risk of LR was significantly influenced by LVZ area quartile with group 4 (highest LVZ area) having the highest risk (p<0.001; Figure 3A). The percentage of LVZ was also associated with the risk of LR (p<0.001; Figure 3B). In multivariable Cox regression analysis, LVZ area as a quartile or 2 groups were significant risk factors for LR after RFCA (Table 3). Age, LA diameter, ejection fraction of left ventricle, E over e′, and LAA flow velocity were all significantly associated with the risk of LR in univariable analysis. However, these variables were not associated with LR in multivariable analysis with only AF type and LVZ being significant risk factors for LR.
Figure 3
Impact of LVZ on LR. (A) Freedom from LR was significantly affected by LVZ area quartile. The p value for (i) group 1 vs. group 2=0.774; (ii) group 1 vs. group 3=0.001; (iii) group 1 vs. group 4<0.001; (iv) group 2 vs. group 3=0.004; (v) group 2 vs. group 4<0.001; (vi) group 3 vs. group 4=0.054. (B) Freedom from late recurrence LR was significantly affected by LVZ percentage quartile. The p value for (i) group 1 vs. group 2=0.567; (ii) group 1 vs. group 3<0.001; (iii) group 1 vs. group 4<0.001; (iv) group 2 vs. group 3<0.001; (v) group 2 vs. group 4<0.001; (vi) group 3 vs. group 4=0.318.
LR = late recurrence; LVZ = low voltage zone.
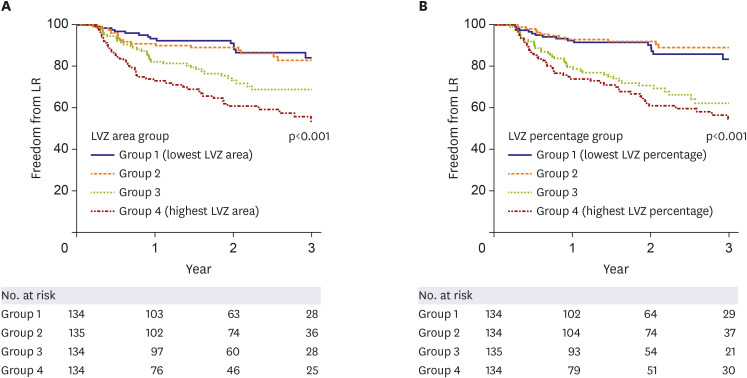
Table 3
Factors associated with late recurrence
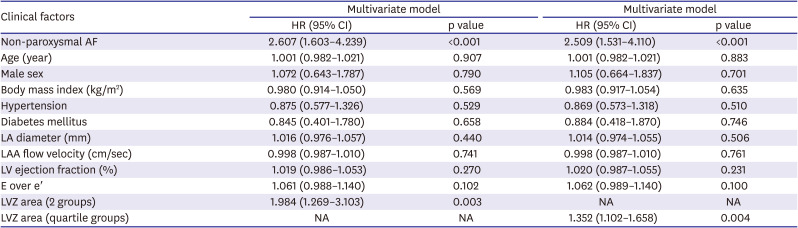
Variance inflation factor values among all covariates included in the multivariate model were below 2 indicating no multicollinearity was present in the model.
AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio; LA = left atrium; LAA = left atrial appendage; LV = left ventricle; LVZ = low voltage zone; NA = not available.
Electrical vs. structural remodeling
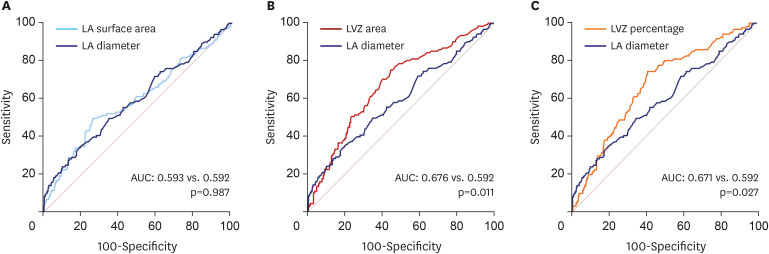
The diameter of LA (AUC, 0.592; 95% CI, 0.532–0.653; p=0.002), LA surface area (AUC, 0.593; 95% CI, 0.532–0.654; p=0.002), LVZ area (AUC, 0.676; 95% CI, 0.622–0.729; p<0.001), and LVZ percentage (AUC, 0.671; 95% CI, 0.617–0.724; p<0.001) were all able to predict the occurrence of LR. In AUC comparison analysis, LA diameter and LA surface area had similar predictive values for LR (0.593 vs. 0.592; p=0.987; Figure 4A). In contrast, LVZ area (0.676 vs. 0.592; p=0.011; Figure 4B) and LVZ percentage (0.671 vs. 0.592; p=0.027; Figure 4C) had significantly superior predictive values for LR compared with LA diameter.
Figure 4
Electrical remodeling vs. structural remodeling. (A) LA diameter and LA surface area showed similar predictive value for late recurrence. (B) LVZ area had significantly higher predictive value compared with LA diameter. (C) LVZ percentage had significantly higher predictive value compared with LA diameter.
AUC = area under curve; LA = left atrium; LVZ = low voltage zone.
DISCUSSION
This study demonstrated that (i) AF patients with higher amount of LVZ are at increased risk of LR after undergoing RFCA; (ii) amount of LVZ which reflects electrical remodeling can be a more reliable predictor for LR compared with LA diameter, a marker of structural remodeling. The results of our study justifiy routine performance of voltage mapping since it can add a predictive value for LR in AF patients undergoing RFCA. The current NavX system enables simultaneous mapping of both 3-dimensional geometry and voltage mapping and therefore, the additional risk for performing voltage mapping is negligible.
The underlying pathophysiology of AF is multifactorial. In paroxysmal AF, triggering activities from pulmonary and extra-PV foci are assumed to be the main factor and elimination of triggers are proven to be an effective treatment strategy.21) However, elimination of trigger foci might not be sufficient for non-paroxysmal type of AF.9)22) In STAR AF II trial, freedom from arrhythmia recurrence at 1 year in those who underwent PV isolation only was around 60%. Although addition of linear ablation or complex fractionated atrial electrogram-guided ablation did not improve the overall outcome, high recurrence rate suggests that we need a better understanding of the nature of non-paroxysmal AF and a better way to detect the culprit lesion.
Atrial myopathy is characterized by replacement of atrial cardiomyocytes by interstitial fibrosis.23)24) The degree of interstitial fibrosis in AF is closely related with the stage of AF. In the initial stage of AF, fibrosis is usually limited to PVs and surrounding LA myocardium. As AF progresses to non-paroxysmal stage, the remodeling process extends to the body of LA and even to right atrium.24)25)26) This remodeling process is often called as a substrate for AF. Substrate can not only trigger AF but also maintain AF. These observations suggest that PV isolation only strategy may not be sufficient for advanced stage of AF. Although we do not have an answer to efficiently eliminate these substrates for AF, further studies to find a better ablation strategy than PV isolation only are warranted.
In accordance with previous studies, our results demonstrated that LVZ which represents electrical remodeling of atrium can predict freedom from AF and AT after RFCA.12)15)27) The AUC was significantly higher in LVZ area or percentage as compared with LA diameter suggesting that LVZ can be a better predictor for LR than LA diameter, a widely used traditional risk factor for LR. The surface area of LA which was measured during electroanatomic mapping showed similar predictive value with LA diameter. These observations indicate that structural remodeling of LA is not a sufficient marker to estimate the risk of LR after RFCA and factors reflecting electrical remodeling can complement. The limitation of LVZ is that non-invasive method for quantification is lacking and it can only be evaluated during the procedure. However, a recent study reported that the presence of LVZ can be predicted by pre-procedural markers (sex, age, diabetes, type of AF, brain natriuretic peptide).28) Whether delayed gadolinium enhancement in cardiac magnetic resonance imaging correlates with LVZ acquired with electroanatomic mapping is another interesting area of future research.
Prior studies demonstrated atrial scarring results in a decrease of bipolar voltage and patients with high burden of LVZ are at higher risk of recurrence.12)15)27)29) However, whether ablation of LVZ, a substrate of AF, can improve the result of RFCA is not well validated and is a hot topic in the field of electrophysiology. Traditional linear ablation or complex fractionated electrogram-guided ablation strategy did not improve overall outcome compared with PV isolation only approach.9) Initial studies evaluating LVZ ablation provided promising results. A single-center randomized trial from Germany reported a significantly higher freedom from LR in voltage guided ablation group as compared with conventional substrate modification group.14) The STABLE-SR multi-center trial reported similar rate of freedom from LR in voltage guided ablation group vs. stepwise substrate modification group (linear ablation → complex fractionated atrial electrogram guided ablation) with lower fluoroscopy and ablation time.30) Large scale multi-center randomized trial is needed to further examine the impact of LVZ ablation on LR after RFCA.
Several limitations exist in this study. In our cohort, no cryoablation was performed and therefore, the impact of LVZ in cryoablation cannot be examined. During the study period, HD Grid catheter was not available and all electroanatomic mapping were done with AFocus II circular mapping catheter. Since HD Grid catheter has several advantages over AFocus II catheter such as perpendicular recordings of bipolar signals, it might be able to improve accuracy of LVZ identification. In this study, LA volume and volume index were not available and structural remodeling was evaluated with LA diameter.
In conclusion, the amount of LVZ in LA was significantly associated with LR after RFCA. Electrical remodeling represented by LVZ might be a superior predictor of LR as compared with LA diameter, a traditional marker of structural remodeling. The value of ablation strategy targeting LVZ should be determined in future studies.
 XML Download
XML Download