

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension is the most common modifiable risk factor for cardiovascular disease, the leading cause of death worldwide.1) In 2015, the estimated number of deaths that were associated with hypertension was 7.8 million, accounting for 14% of all deaths.2) As of 2018, the prevalence of hypertension in Korea was estimated to be 29% in people aged 20 or older and 33% in people aged 30 or older.3) According to the National Health Insurance Service database of Korea, the number of patients using medical service with diagnosis of hypertension increased from 3 million in 2002 to over 9 million in 2018. The estimated medical cost of treating hypertension was 3,830 billion Korean Won, accounting for 4% of all medical expenses or 16% of medical expenses for chronic diseases in 2019.3)
The prevalence of hypertension is known to be higher in men than in women, but not in all age groups. Blood pressure (BP) above normal range is highly common among elderly women, so the disease burden of hypertension is not less for women than men. Hypertension accounts for about 1 in 5 deaths of United States women and is a greater burden for women than men.4) Among adult Americans, men present higher prevalence of hypertension and lower control rate compared to women. However, after age 60, women suffer from higher prevalence, lower control rate, and more complications of hypertension, compared to their male counterparts.5) Despite these age- and sex- related differences in prevalence of hypertension, women are under-represented in many clinical studies.6)
Korea is the world's fastest aging country, and the average life span difference between men and women is wide, resulting in a rapid increase in the elderly female population. However, there is only limited data on the prevalence and absolute number of hypertension in women compared to those in men.7) Thus we analyzed national representative survey data to compare the prevalence of hypertension, the number of people with hypertension and their trends, between men and women.
METHODS
Ethical statement
The KNHANES were administered by the Korea Center for Disease Control and Prevention and approved by the Institutional Review Board (2007–02-CON-04-P, 2008-04EXP-01-C, 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C, 2013-07CON-03-4C, 2013-12EXP-03-5C, 2015-01-02-6C, 2018-01-03-P-A).
Participants and data source
This study analyzed the data from the Korea National Health and Nutrition Examination Survey (KNHANES). The KNHANES is a nationwide cross-sectional survey, conducted by the Korea Disease Control and Prevention Agency. The survey design, data collection, and detailed protocols in the KNHANES have been published.8)9) The survey chose a stratified and multistage clustered probability sampling method to select the representative households of Korean citizens who live in Korea. The KNHANES was initiated in 1998 and there have been 7 rounds of KNHANES between 1998 and 2018: KNHANES I (1998), KNHANES II (2001), and KNHANES III (2005) KNHANES-IV (2007–2009), KNHANES V (2010–2012), KNHANES VI (2013-2015) and KNHANES VII (2016–2018). Among total of 173,900 adults (average 24,842 per each round), 128,949 adults aged 20 years and older with valid BP measurement were included in the analysis. As an exploratory analysis, the comparison between men and women of the prevalence of comorbidities was conducted for 5,317 adults with hypertension in the 7th KNHANES (2016–2018).
The KNHANES was composed of health interview, health examination, and nutrition survey.9) Trained interviewers collected information about the age, gender, socioeconomic status, education, insurance type and lifestyle. The questionnaires included history of selected chronic diseases by a physician diagnosis and current use of agents for those diseases. Trained medical staff measured the anthropometric and biochemical information. All samples were venous blood gatherings in the morning after an 8 hour fast. Since 2005, for quality control, the protocol applied to all laboratory analyses and laboratory data was monitored to meet the standards with validity and reliability. The standard protocol was adapted when measuring BP. After of at least 5 minutes of rest and in sitting position, BP was measured on the right arm by a mercury sphygmomanometer (Baumanometer; Baum, Copiague, NY, USA). To increase accuracy, the average value of BP measured twice in 1998 and 2001, and the average value of the second and third BP measured three times after 2005 were calculated. BP and body measurements were performed for quality assurance and control in academic societies.8)
Definition of hypertension and other indicators
Hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg, diastolic blood pressure (DBP) ≥90 mmHg, or self-reported use of antihypertensive medication for the purpose of BP control. Hypertension was further classified into 4 categories of ‘undiagnosed,’ ‘diagnosed-but-untreated,’ ‘treated-but-uncontrolled,’ and ‘controlled’ hypertensions. Undiagnosed hypertension was defined as people currently having hypertension without previous physician diagnosis. Diagnosed-but-untreated hypertension was defined as people with physician-diagnosed hypertension but not taking antihypertensive medication regularly (<20 day/month). Treated-but-uncontrolled hypertension was defined as people with SBP/DBP ≥140/90 mmHg even with regular antihypertensive medication uses. Controlled hypertension was defined as antihypertensive medication users with SBP/DBP <140/90 mmHg. Stage 2 hypertension was defined as SBP ≥160 mmHg or DBP ≥100 mmHg. Elevated BP was defined as SBP ≥140 mmHg or DBP ≥90 mmHg with or without antihypertensive medication.
The prevalence of comorbidities (obesity, dyslipidemia, diabetes mellitus, cardiovascular disease, chronic kidney disease) accompanying hypertension was analyzed using the 7th (2016–2018) KNHANES data. Obesity was defined as high body mass index (≥25 kg/m2) or increased waist circumference (≥90 cm for men and ≥85 cm for women), according to the World Health Organization Asia–Pacific region guidelines,10) redefined for the Asian population. Dyslipidemia was defined as fasting total cholesterol ≥240 mg/dL, triglycerides ≥200 mg/dL, low-density lipoprotein cholesterol ≥160 mg/dL, high-density lipoprotein cholesterol <40 mg/dL, or current use of cholesterol-lowering agents.11) Diabetes was defined as having a fasting plasma glucose ≥126 mg/dL, the current use of antidiabetic agents or the use of insulin prescribed by physician due to a previous diagnosis of diabetes. Cardiovascular disease was defined as the previous diagnosis of stroke, myocardial infarction, or angina pectoris. Chronic kidney disease was also defined as being a previous diagnosis given by a physician.12) The number of comorbid diseases was defined as the number of known diseases among obesity, dyslipidemia, diabetes mellitus, cardiovascular disease, and chronic kidney disease.
Statistical analysis
Survey procedures of the Statistical Analysis System program (SAS 9.3 Institute Inc., Cary, NC, USA) were used to perform the analysis of a complex sample data. The sampling weights were applied to all analyses in order for the results to represent the Korean population as a whole. Sampling weights were used to reflect a complex sample design, non-response rate, and post-stratification.8)
The results of prevalence analysis presented as estimated prevalence and 95% confidence interval (CI) with sampling weights applied. The estimated number and 95% CI were calculated by adjusting the prevalence to the demographics of Korean population in each round’s median year from the Population and Housing Census, Statistics Korea.13) The female-to-male ratio was calculated by dividing the estimated prevalence in women by the estimated prevalence in men. Age-standardized prevalence was calculated based on the demographics of the Korean population in 2005 according to the Population and Housing Census, Statistics Korea.13)
RESULTS
Sex-specific trends in prevalence and number of people with hypertension
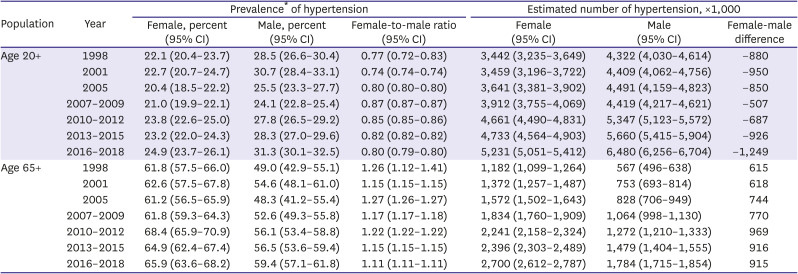
The prevalence of hypertension in Korean women aged 20 or older increased from 22.1% in 1998 to 24.9% in 2016–2018, and the prevalence of men increased from 28.5% to 31.3% during the same period (Table 1). However, this increase in prevalence seems to be due to the population aging, because age-standardized prevalence of hypertension did not increase during the same period (Supplementary Table 1). The estimated number of people with hypertension is steadily increasing over the same period: 3.44 to 5.23 million for women; 4.32 to 6.48 million for men. Currently, the number of male hypertension patients exceed the number of female patients by 1.25 million. However, when the analysis was limited to the elderly population aged 65 years or older, the prevalence showed increasing trends both for women (from 61.8% to 65.9%) and men (from 49.0% to 59.4%), with a higher prevalence in women. The estimated number of hypertensive elderly women increased from 1.18 million in 1998 to 2.70 million in 2016–2018, and the number of hypertensive elderly men increased from 0.57 million to 1.78 million during the same period. Currently, the number of elderly female hypertensive patients exceed the number of elderly male hypertensive patients by 0.92 million.
Table 1
Prevalence and number of people with hypertension in Korean men and women (age 20+ and age 65+)
Sex-specific trends in elevated BP and stage 2 hypertension
The prevalence and estimated number of elevated BP (SBP/DBP >140/90 mmHg regardless of the use of anti-hypertensive medication) in Korean adult populations have been decreasing, probably perhaps thanks to improved hypertension diagnosis and treatment rates. However, the absolute number of elderly (age 65+) people with elevated BP is rather increasing again recently, although the prevalence of elevated BP has dropped by half. In addition, the absolute number of elderly people with elevated BP is about twice as many women as men (Supplementary Table 2).
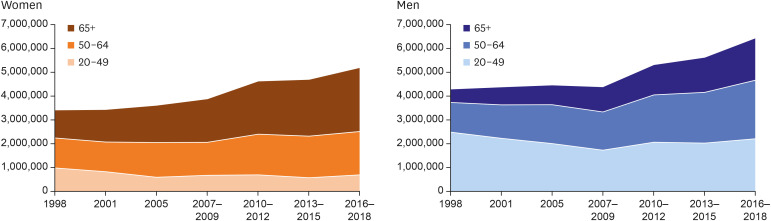
People with stage 2 hypertension have a very high risk of developing and dying of cardiovascular disease, so it can be a population-level indicator of cardiovascular disease prevention. In Korea, the stage 2 hypertension has been decreased significantly not only in the adult population but also in the older adults. However, 5.6 percent of the elderly women and 3.5 percent of the elderly men still belong to the group, which is equivalent to about 234,000 elderly women and 105,000 elderly men (Supplementary Table 3). Figure 1 shows time trends in the number of people with hypertension by three age groups (20–49, 50–64, and 65+) for women and men. Significant increase in the number of hypertensive patients was observed in women aged 65 or older and in men aged 50–64 or older.
Sex-specific trends in hypertension by management status
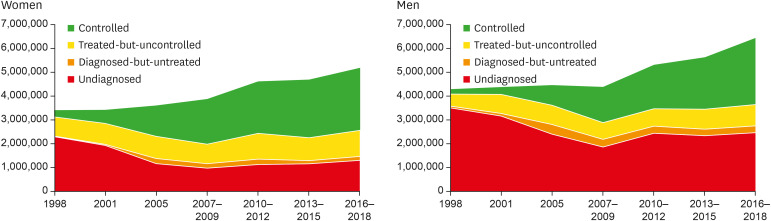
Figure 2 shows time trends in the number of people with hypertension by management status (controlled, treated-but-uncontrolled, diagnosed-but-untreated, and undiagnosed) for women and men. A decrease of undiagnosed hypertension and an increase of controlled hypertension were observed in both sexes. Currently, compared to men, women show smaller proportions of undiagnosed hypertension and diagnosed-but-untreated hypertension, but a larger proportion of treated-but-uncontrolled hypertension.
Sex- and age-specific trends in hypertension
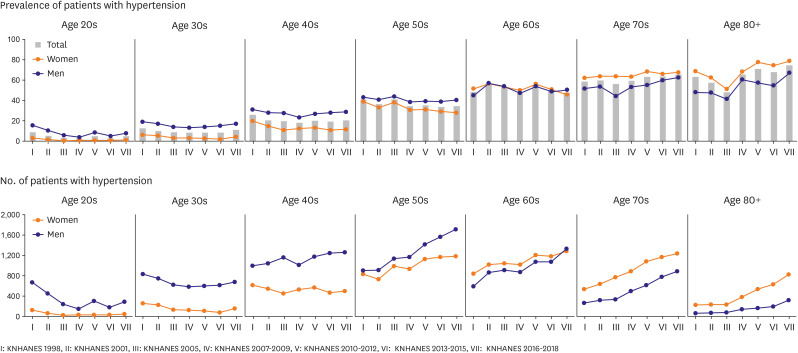
Figure 3 shows the prevalence and number of people with hypertension patients by sex and age over time. The prevalence of hypertension has been increased in those aged 70 or older, but there was no change in the younger age groups. The prevalence was higher for men until age 50s, similar for women and men in age 60s, and higher for women in age 70s or older. Changes in absolute number of people with hypertension were not the same as changes in the prevalence. The number of hypertensive patients did not increase among age 20s and 30s. The number of hypertensive patients in age 40s has increased only in men but not in women. The number of hypertensive patients in age 50s increased in both sexes, but the increase was steeper in men. In age 60s and 70s, increase in the number of hypertensive patients was similar for women and men, but the absolute number was greater for women. In age 80s, women outperform men in both increasing speed and the absolute number.
Prevalence of comorbidities among people with hypertension
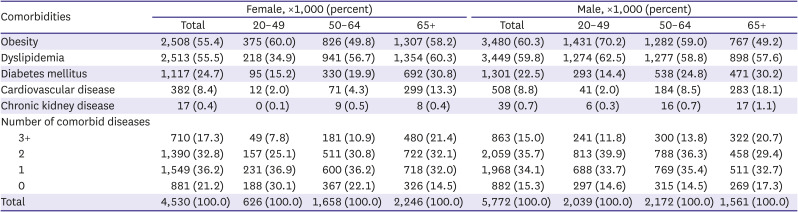
Table 2 shows the prevalence of comorbidities among people with hypertension, stratified by sex and age. In hypertensive women, the prevalence of chronic diseases such as obesity, dyslipidemia, diabetes mellitus, and cardiovascular disease increases as the age increases. In hypertensive men, the prevalence of obesity and dyslipidemia decreases with age, and diabetes mellitus, cardiovascular disease and chronic kidney disease increase as the age increases. As a result, multi-comorbidity (having at least two of the five conditions) was similar for overall women and men (50.1% versus 50.7%), but became more common in elderly women than in elderly men (53.5% versus 50.1%).
Table 2
The estimated number and prevalence of five comorbid diseases among hypertension patients
DISCUSSION
Over the last two decades, the estimated number of hypertension in men and women has steadily increased. In most parts of the world, including the United States, epidemic of obesity and the increasing detection rate of hypertension was the main contributing factors to the increasing number of people with hypertension. Between 1999 and 2014, the prevalence of obesity in adults in the United States increased significantly from 30.5% to 37.7%.5) There was a significant linear increase in obesity from 2005 to 2014, especially in women. However, it is unlikely that the increase in the number of hypertensive patients in Korea is caused by changes in obesity or hypertension detection rate. In Korea, increase of obesity was observed in men but not in women.8) In addition, national and private health checkups are very common in Korea, and the awareness rate of hypertension has not increased any more in recent years.3) Therefore, the main factor that increase the number of hypertensive patients in Korea would be the increase in the elderly population. Since the prevalence of hypertension is higher among women in the elderly population,2) it seems that the number of women with hypertension increases with the aging of society. The proportion of the of the population aged 65 and over in South Korea increased from 10.2% in 2008 to 16.4% in 2020, which corresponds to an aged society.13)
In our study, the prevalence and the number of hypertension are lower in women than in men until age 60s and 50s, respectively, but increase later in life. The increasing prevalence of hypertension in older women was often explained by hormonal changes after menopause. Estrogen causes endothelial vasodilation via upregulation of the nitric oxide pathway and inhibition or down regulation of sympathetic and renin angiotensin system activity, as well as endothelin production.14)15)16) Therefore, low postmenopausal estrogen levels may decrease arterial compliance and increase the risk of hypertension17)18) and cardiovascular disease6)18) in elderly women. Androgen deficiency after menopause also increases the risk of hypertension by increasing visceral obesity and contributing to adipocyte and endothelial dysfunction.6) In addition to hormonal changes, anatomical and physiological sex differences may contribute to sex differences in hypertension prevalence in old age.19)20) In association with the anatomical and physiological and sex differences of the heart and blood vessels, mean arterial pressure and pulse pressure increased faster in women than in men with aging.21) Hypertension in women can be particularly harmful. Several studies found stronger association of hypertension with ischemic heart disease mortality and myocardial infarction in women than in men.19) Pathological changes in blood vessels and heart in women with aging progress faster than in men, which is associated to the risk of coronary microvascular insufficiency and heart failure with preserved ejection,21) which is primarily associated with arterial stiffness and hypertension.22) Recently, hospitalization and mortality rates from heart failure have increased rapidly in Korea, and the rate of increase is much faster in women than in men.23)
The proportion of treated-but-uncontrolled hypertension is higher in women than in men. In addition, stage 2 hypertension is more prevalent in elderly women than in elderly men, and the estimated number of elderly women with stage 2 hypertension is more than twice that of men. Hypertension accompanied by multiple chronic diseases is also more common in elderly women than in elderly men. Taken together, it can be interpreted that the number of hypertensive patients with difficulty in controlling BP and a high risk of cardiovascular disease is increasing rapidly, especially in elderly women.
A study of the United States primary care clinics reported that women aged 65 to 80 were less likely to control their BP than men of same age, even after adjusting for multiple factors.24) Although biological aging related to endogenous stimulation seems to be a significant factor in the poor control of hypertension in women compared to men, the reasons for this sex difference are not clear.6) In addition to biological aging, the possible explanations for this age-related decline in BP control among women may include poor lifestyle modification including lower physical activity, inadequate treatment in women and non-adherence to antihypertensive in elderly women.4) In a nationally representative samples of adults in the United States, only 20.1% women reported participating in adequate physical activity that meets guidelines, and compared to 28.8% of men.25) Co-existing risk factors or clinical sequelae in elderly women may cause difficulty in controlling BP despite treatment. Hypertension frequently occurs with multiple comorbidities that may amplify the cardiovascular risk of an affected individual or a specific population.20) However, the factors lowering hypertension control rate in elderly women in Korea may be different from those in the Western population. Since Korean society has experienced huge changes over the past decades, there is a significant inter-generational difference also in gender inequality. Older women tend to be even more disadvantaged in education, occupation, and social networks than younger women. To improve BP control in elderly Korean women, further research is needed to evaluate the impact of biological, socioeconomic, behavioral factors as well as comorbidities on BP control.
This study has several limitations to be addressed. First, we cannot exclude the possibility of misclassification of hypertension. The KNHANES has measured BP values using a standard mercury sphygmomanometer, and employed quality control program of BP measurement. Nevertheless, changes in the screening environment and the BP measurement values may differ depending on the investigators. In addition, the BP readings were obtained on a single visit, so any variability in BP was not documented. Second, out-of-office BP measurement was not available. Therefore, we could not exclude white coat hypertension and could not include masked hypertension. Third, the KNHANES was designed to recruit representative sample of the Korean population, but institutionalized people were excluded from the sample. Thus, people with severe or complicated hypertension were less likely to be included. This might underestimate the prevalence and absolute number of hypertension.
In the younger and middle-aged adults, women tend to have lower prevalence and better management of hypertension than men, but in older women, the prevalence of hypertension increases rapidly, other comorbidities become frequent, and the BP control worsens. With the rapid aging, especially the surge in the elderly female population in Korea, the number of elderly women with hypertension and multi-comorbidities is rapidly increasing, which will be a serious public health challenge. A multi-pronged approach is needed to reduce the public health burden of hypertension in women. It is required to develop guidelines for the prevention and management of hypertension, which are tailored for different demographic groups. A population approach is also needed to increase awareness on the hypertension in women, and to achieve more thorough BP control especially for postmenopausal women.
 XML Download
XML Download