

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometriosis is a benign, estrogen-dependent, chronic disease that is characterized by the presence and growth of endometrial-like tissue outside the uterus.12 Among the types of endometriosis, ovarian is the most frequent.3 If clinical evidence suggests endometrioma, medical therapy can be useful for patients without an immediate desire for pregnancy.4567 However, because the efficacy of medical treatment is limited, surgery to remove endometrioma and restore normal anatomy is necessary in some cases.8 Without postoperative medical therapy, the recurrence rate of endometrioma is 21.5% at two years and 40–50% at five years.9 In addition, surgical management of recurrent endometrioma can be more challenging and involves a considerable risk of reduced ovarian function.10 Therefore, postoperative medical therapy is recommended to prevent recurrence of endometrioma.11
There are several medical treatment options for endometrioma. Progestin, especially dienogest, is an effective drug for preventing recurrence of endometrioma after surgery.12 Additionally, oral contraceptive (OC) use after conservative surgery has been reported to reduce significantly the risk of endometrioma recurrence.913 Postoperative gonadotropin-releasing hormone (GnRH) agonist alone did not reduce the recurrence rate in a previous study.14 However, OC use after GnRH agonist has been effective for preventing recurrence as it suppresses endometriotic lesions and maintains the hypogonadal state induced by the GnRH agonist.15
One previous study compared the postoperative recurrence rate of endometrioma of OC after GnRH agonist versus that of dienogest treatment over 24 months. However, as no recurrent case was reported, no comparison could be performed.16
The present study was conducted to compare the long-term effects of OC after GnRH agonist treatment with those of dienogest treatment in prevention of endometrioma recurrence.
METHODS
Patients
Reproductive-aged women who underwent conservative laparoscopic surgery for ovarian endometrioma for the first time between January 2000 and December 2020, at Samsung Medical Center were considered for this retrospective study. The inclusion criteria were as follows: 1) pathologically confirmed endometriosis of the ovary, 2) followed up on the same regimen (OC after GnRH agonist or dienogest) for at least six months after surgery, 3) no lesion suspected to be remnant endometrioma on ultrasonography (USG) after surgery, and 4) visited a clinic regularly every three to six months. Patients were excluded if they had 1) undergone oophorectomy or hysterectomy, 2) undergone any previous ovarian surgery, 3) no postoperative medical therapy, 4) changed their regimen, 5) been administered either a GnRH agonist or OC alone, 6) use of GnRH agonist < 3 or > 6 months in the GnRH agonist followed by OC group, or 7) confirmed borderline tumor associated with atypical endometriosis.
Study design
Based on medication after surgery, patients were divided into two groups: those receiving OC after GnRH agonist and those receiving only dienogest (Visanne®; Bayer, Leverkusen, Germany). On the day that pathology was confirmed, GnRH agonist treatment or 2 mg/day dienogest was initiated. Three to six cycles of GnRH agonist (leuprolide acetate 3.75 mg, Leuprorelin®; Takeda Pharmaceuticals, Tokyo, Japan) were administered every four weeks subcutaneously in the OC group depending on patient condition. The OC was started four weeks after the last injection of GnRH agonist. In a previous study, since there was no difference in recurrence rate of endometrioma between a cyclic regimen and a continuous regimen,17 all patients receiving OC were prescribed a cyclic regimen to reduce discomfort caused by breakthrough bleeding. There are two types of cyclic regimens according to the number of pill-free intervals: 21/7 OC consists of 21 active pills and 7 days of no pill, whereas 24/4 OC consists of 24 active pills and 4 placebo pills. For 21/7 OC, patients were provided ethinyl estradiol 0.03 mg and drospirenone 3.0 mg (Yasmin®, Bayer) or ethinyl estradiol 0.02 mg and desogestrel 0.15 mg (Mercilon®; Alvogen, Pine Brook, NJ, USA) or ethinyl estradiol 0.035 mg and cyproterone acetate 2.0 mg (Diane-35®; Bayer). Before 2008, Mercilon was used as a third-generation OC. Starting in 2008, the fourth-generation OC Yasmin was adopted and used in place of Mercilon. All patients with a 24/4 OC regimen were prescribed ethinyl estradiol 0.02 mg and drospirenone 3.0 mg (Yaz®; Bayer), which was introduced in 2009. The OC regimen depended on the date and patient preference.
Preoperative cancer antigen 125 (CA-125) level was measured before surgery, and the revised American Society for Reproductive Medicine (rASRM) stage was evaluated during surgery. While taking medications, USG was performed every six to 12 months after surgery and when symptoms such as pelvic pain or abdominal discomfort were present. Recurrence of endometrioma was noted at an ovarian lesion of 2 cm or greater on USG.
Surgery
Laparoscopic cystectomy was performed by the same surgeon for all patients. During surgery, adhesiolysis, removal of visible peritoneal endometriotic lesions, or correction of anatomical distortion was performed depending on the status of endometriosis. An adhesion barrier (Interceed®; Johnson & Johnson Medical Devices Companies, New Brunswick, NJ, USA) was applied in all patients.
Statistical analyses
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Differences in baseline characteristics including CA-125 level and rASRM stage between the two groups (OC after GnRH agonist versus dienogest) were analyzed using the χ2 test or Fisher’s exact test for categorical variables and Wilcoxon rank sum test for continuous variables. In addition, differences among the three groups (21/7 OC after GnRH agonist, 24/4 OC after GnRH agonist, and dienogest) were evaluated using the χ2 test or Fisher’s exact test for categorical variables and Kruskal-Wallis test for continuous variables. P values were corrected using Bonferroni’s method for categorical variables and Tukey’s method for continuous variables in the case of multiple comparisons between the groups.
The cumulative endometrioma recurrence curve was presented using the Kaplan-Meier method and was compared between the groups with the log-rank test. A P value resulted from multiple testing due to both comparison between the GnRH agonist followed by OC and the dienogest groups and between the comparison among GnRH agonist with 21/7 OC, GnRH agonist with 24/4 OC, and dienogest was corrected using Bonferroni’s method. All P values < 0.05 were considered statistically significant.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This retrospective study was granted approval by the Institutional Review Board (IRB) of Samsung Medical Center and the requirement for informed consent was waived (IRB: 2020-06-044-004).
RESULTS
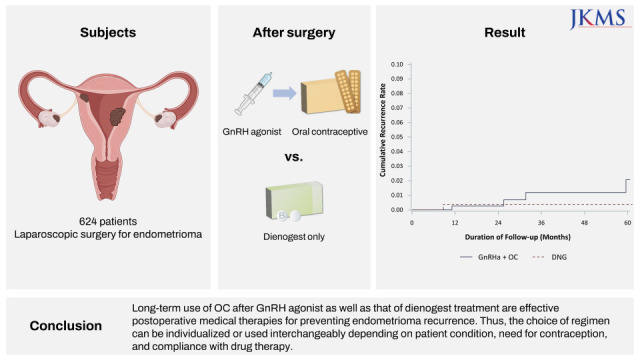
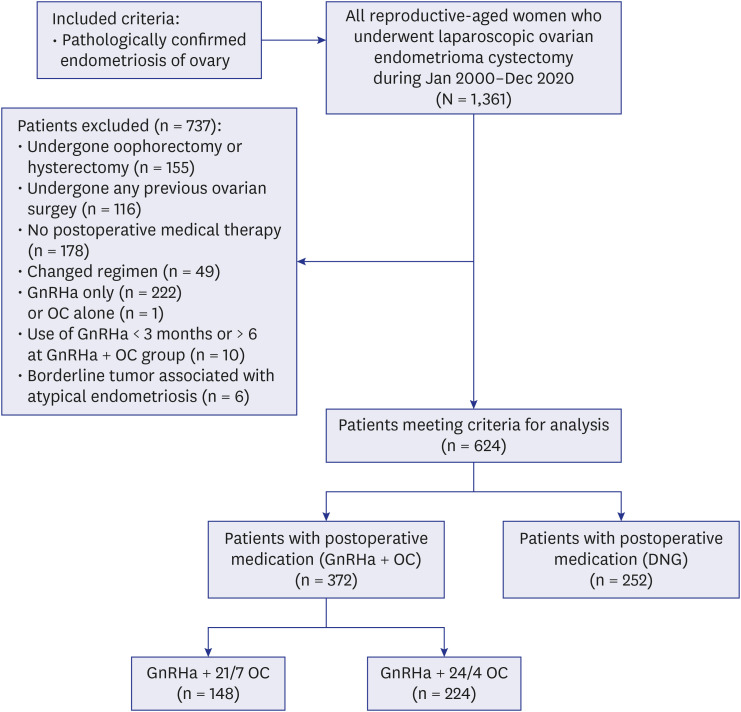
A total of 624 patients was included in this study (Fig. 1). Three hundred seventy-two patients used OC after GnRH agonist therapy and 252 patients used dienogest. Within the OC group, 148 used a 21/7 regimen, and 224 used a 24/4 regimen. The median follow-up period after surgery was 34.36 months (range, 6.3–238.75 months), and the median age of patients was 28 years (range, 15–48 years).
Fig. 1
Patient flow chart.
GnRHa = gonadotropin releasing hormone agonist, OC = oral contraceptive, DNG = dienogest.
The baseline characteristics of the GnRH agonist followed by OC group and the dienogest group are listed in Table 1. There were no significant differences between the groups in terms of age at surgery, body mass index, parity, age at menarche, cyst bilaterality, and endometrioma size, although there was difference in rASRM stage and preoperative CA-125 level. However, the rASRM stages of patients were all III or IV, which means a moderate to severe form of endometriosis and indicated need for surgery.
Table 1
Baseline characteristics
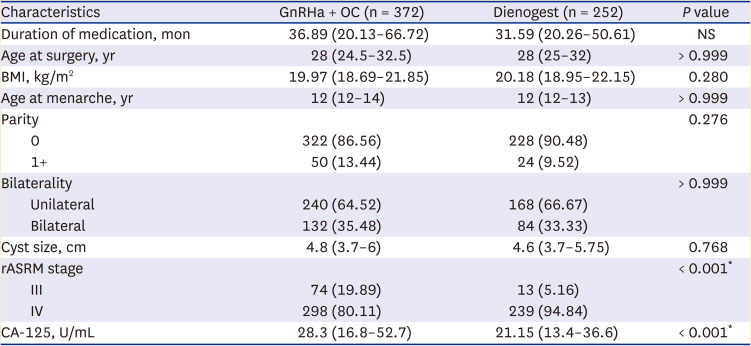
Data are expressed as median value with interquartile range or number (%).
NS = not significant, GnRHa = gonadotropin releasing hormone agonist, OC = oral contraceptive, BMI = body mass index, rASRM = revised American Society for Reproductive Medicine, CA-125 = cancer antigen 125.
*P < 0.05 between the two groups by Wilcoxon rank-sum test, Fisher’s exact test, or χ2 test followed by Bonferroni’s correction, as indicated.
The GnRH agonist followed by OC group was divided by pill-free period of 21/7 OC or 24/4 OC for subgroup analysis. Baseline characteristics of the three groups, GnRH agonist with 21/7 OC, GnRH agonist with 24/4 OC, and dienogest, are shown in Table 2. There were significant differences only in parity, rASRM stage, and CA-125 level among the three groups. Though parity was statistically different among the three groups (χ2 test with Bonferroni’s correction; P = 0.044), multiple comparisons using Fisher’s exact test with the Bonferroni method showed no significant difference between the dienogest and 24/4 OC groups (P > 0.999), 21/7 OC and 24/4 OC groups (P = 0.182), and dienogest and 21/7 OC groups (P = 0.080).
Table 2
Baseline characteristics of the study subjects according to postoperative adjuvant therapy: subgroup analysis
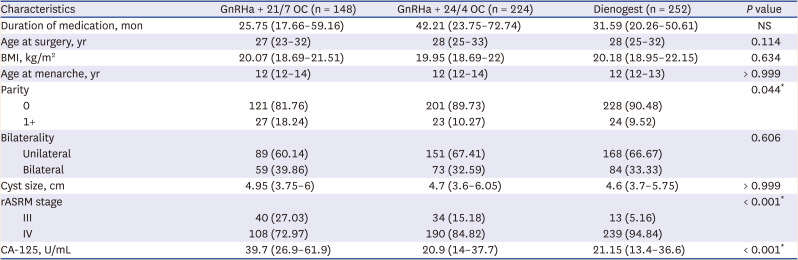
Data are expressed as median value with interquartile range or number (%).
NS = not significant, GnRHa = gonadotropin releasing hormone agonist, OC = oral contraceptive, BMI = body mass index, rASRM = revised American Society for Reproductive Medicine, CA-125 = cancer antigen 125.
*P < 0.05 between the three groups by Kruskal-Wallis test, Fisher’s exact test, or χ2 test followed by Bonferroni’s correction, as indicated.
Over 60 months of follow-up post-surgery, endometrioma recurred in five patients, four in the OC group and one in the dienogest group. The cumulative recurrence rate of endometrioma over 60 months was 2.08% (n = 4) in the OC after GnRH agonist therapy group and 0.40% (n = 1) in the dienogest group. There was no statistical difference in the cumulative recurrence curve of endometrioma between OC after GnRH agonist and dienogest groups (log-rank test with Bonferroni’s correction; P = 0.846) (Fig. 2). Subgroup analysis showed that the cumulative recurrence curves during 60 months of endometrioma for 21/7 OC, 24/4 OC, and dienogest were not statistically different (log-rank test with Bonferroni’s correction; P > 0.999) (Fig. 3). In addition, the recurrence rate of endometrioma was evaluated using multiple comparisons through the log-rank test. There was no significant difference in recurrence rates by pair. The first and last recurrence of endometrioma occurred at eight and 59 months after surgery, respectively, as confirmed by transvaginal USG during the follow-up period. At the time of recurrence, four patients were in their 20s and one in their 30s. All recurrent cases were rASRM stage IV.


DISCUSSION
In this study, we demonstrated that OC treatment after GnRH agonist is as effective as dienogest alone as postoperative medical therapy for preventing recurrence of endometrioma. In addition, subgroup analysis was performed by dividing the OC group after GnRH agonist treatment into 21/7 and 24/4 OC to determine whether the pill-free period had an effect on endometrioma recurrence, and there was no difference in recurrence rates between the two groups.
Progestin is an effective medical therapy for endometriosis in that it leads to atrophy and decidualization of ectopic endometrial tissue and induces anovulation by decreasing estrogen level.218 In the dienogest group, only one case of relapse occurred, a cumulative recurrence rate of 0.398% over 60 months. This is consistent with previous studies showing that a 0% to 1.8% recurrence rate of endometrioma when using dienogest as a postoperative medical therapy over 13 to 41 months.12161920
The use of GnRH agonist might be necessary as complete resection of endometrioma in surgical treatment is difficult, and microscopic dissemination cannot be treated.21 Although GnRH agonists are powerful suppressants, they cannot be used for a long period due to the side effect of bone loss.22 Therefore, OC is used after the GnRH agonist to maintain a low estrogen state, inhibiting the recurrence of endometrioma. The recurrence rate was significantly lower when OC was used after the GnRH agonist than when the GnRH agonist was used alone.15 In our study, the cumulative recurrence rate over 60 months was 2.08% in the group using OC after GnRH agonist treatment.
Since hemorrhagic functional ovarian cysts can affect the formation of endometriomas, suppression of ovulation might be effective for prevention of endometrioma recurrence. Therefore, OC can prevent endometrioma recurrence by ovulation inhibition.23
As such, progestin and OC are both effective methods to prevent recurrence of endometrioma after surgery. Although there are studies comparing progestin and OC in symptom improvement, there are not many studies on recurrence of endometrioma after surgery. A previous 24-month study aimed to compare endometrioma recurrence between two groups but was unable to perform the analysis due to lack of recurrence.16 The present study was a 60-month, long-term study that showed no difference in recurrence rates between the two treatment options.
Meanwhile, a study with a shorter pill-free period OC than 21/7 showed that the 17β-estradiol level was significantly lower and suppression of ovarian activity was more pronounced than that observed with the conventional 21-day regimen.24 Vlahos et al.25 stated that continuous OC seemed to be associated with a lower recurrence rate of endometrioma than cyclic OC. However, Seracchioli et al.26 demonstrated no significant difference in the recurrence rate of endometrioma between cyclic users and continuous users during 24 months of follow-up in their randomized controlled trial. Therefore, our study also divided the 21/7 and 24/4 regimens to determine if the pill-free period had an effect, but there was no statistical difference in the recurrence rate. Table 2 shows a difference in parity among the three groups (P = 0.044), likely due to the more recent introduction of 24/4 OC and dienogest.
The strength of this study is that it compared long-term results when using GnRH agonist followed by OC and dienogest after surgery for the prevention of endometrioma recurrence. Also, it was able to reduce bias in that only one surgeon did surgery, and nevertheless large, long-term data could be obtained. In addition, comparing the 21/7 and 24/4 OC by subgroup analysis showed that recurrence of endometrioma was not significantly inhibited regardless of the pill-free period. However, the shortcoming of this study is that the drugs used differed according to the time when the drug was newly released. Because 24/4 OC (Yaz) and dienogest (Visanne) were released after 21/7 OC (Diane-35, Mercilon or Yasmin), there is a possibility of selection bias. The inability to perform randomization of drug is also a limitation. Thus, it is necessary that a randomized controlled study will be needed to overcome this limitation.
In conclusion, both long-term use of OC after GnRH agonist and of dienogest were effective for postoperative medical therapies for prevention of endometrioma recurrence. Thus, the choice of regimen can be individualized or used interchangeably depending on the patient’s physical or medical condition, need for contraception, and compliance with drug therapy.
 XML Download
XML Download