

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical neural foraminal stenosis (FS) is a common cause of cervical radicular pain due to narrowing of the neural foramen caused by facet hypertrophy, degenerative osteophytes, or posterolateral disc herniation.12 Nonsurgical management of cervical radicular pain may consist of rest, analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and steroid injections.34
A cervical transforaminal epidural (TFE) steroid injection is a useful treatment option for cervical radicular pain.15678 However, cervical TFE steroid injections carry a small risk of catastrophic complications,89 and their efficacy has not been demonstrated in randomized controlled trials (RCTs).10 The most notable risk associated with TFE steroid injection is vascular trespass or unplanned injection into a vein or artery. Serious events, such as seizure, infarction of the brainstem or spinal cord, and death, presumably caused by vascular trespass with resultant distal embolization of a particulate steroid, have been reported.567911 Accordingly, several researchers have investigated more secure routes of steroid delivery in the vicinity of the involved nerve, including the facet joint (FJ) approach.71213
A pilot study by Richarme et al.12 demonstrated preliminary results on the efficacy of computed tomography-guided cervical FJ steroid injection in 17 patients with cervical radicular pain secondary to a cervical disk herniation (CDH). They reported pain relief of > 50% in 41% of patients and contrast extension in the foraminal space in five of seven patients with > 50% pain relief. In addition, Bureau et al.6 reported that FJ steroid injection was a valid, safe, and effective treatment of cervical radicular pain in patients with cervical spondylosis with or without CDH.
However, previous studies showed a short-term effect with a follow-up period of less than one month and enrolled a small number of patients. To our knowledge, no studies have compared the effects of FJ and TFE steroid injections in patients with cervical radicular pain with long-term follow-up and a large number of patients enrolled. Therefore, the aim of this retrospective comparative study was to evaluate the pain scores and functional disability in subjects receiving FJ and TFE steroid injections to treat cervical radicular pain due to FS.
Go to : 
METHODS
Study design
This study was a retrospective comparative review of chart data. Patient privacy and data confidentiality were maintained throughout the study. After the initial data collection, all patient identifiers were deleted from the dataset.
Participants
The study participants were patients who received a cervical FJ or TFE steroid injection at the outpatient Pain Centers of Ewha Womans University Seoul Hospital and Mokdong Hospital between 2019 and 2021. On the day of the procedure, before the injection, the patients were asked to fill out self-assessment questionnaires with their baseline information. To collect data and determine compliance with the inclusion criteria, the electronic clinical records and survey responses were retrospectively reviewed. We selected patients over the age of 18 who were diagnosed with FS based on their clinical profiles, medical examination results, and magnetic resonance imaging (MRI) results. Included patients also experienced cervical radicular pain caused by FS and underwent FJ or TFE injection to treat their symptoms.
The eligibility criteria were as follows: 1) cervical FS confirmed by MRI and concordant radicular pain along a specific nerve root in the upper arm; 2) the need for single-level FJ or TFE steroid injection; 3) cervical radicular pain for more than one month; and 4) a current pain score of 4 or more on a Numeric Rating Scale (NRS) of 0 (no pain) to 10 (worst pain imaginable) despite sufficient conservative treatment for at least one month, including physical therapy or oral medications such as pregabalin, gabapentin, tramadol, acetaminophen, or NSAIDs. The exclusion criteria were as follows: 1) the presence of psychiatric disorders; 2) evidence of vertebral fracture, tumor, pregnancy, or infection of the cervical spine; 3) coagulopathy; 4) allergy to iodinated contrast media; 5) laboratory results suggestive of inflammatory disease or rheumatoid disorders; 6) severe degenerative change in which the needle cannot approach the target area; and 7) cervical-referred pain characterized by axial neck pain, pain with pressure on the spinal column at the cervical facet joint level, and absence of neurologic symptoms.1415
Injection techniques
We performed an FJ steroid injection aseptically using fluoroscopic guidance with a 22 ga, 2.5-inch spinal needle. Subjects were placed in the prone position, and the C-arm was rotated 90° to allow for visualization of the lateral FJ. The appropriate entry site was the lateral border of the cervical FJ, which was marked on the skin. The skin and subcutaneous tissue were anesthetized with 1% lidocaine. Using intermittent fluoroscopy, we advanced the needle via a lateral approach toward the FJ. The needle was not placed too far medially to avoid the spinal cord in anteroposterior (AP) fluoroscopy. Once the needle reached the FJ, we injected 0.5–1.0 mL of contrast media and acquired fluoroscopy images to exclude the intravascular position of the needle and confirm the adequate distribution of the contrast media (Fig. 1A and B). Then, we injected 1 mL of a solution mixed with 1% lidocaine and 2.5 mg dexamethasone. The subjects were observed for 30 minutes post-procedure.
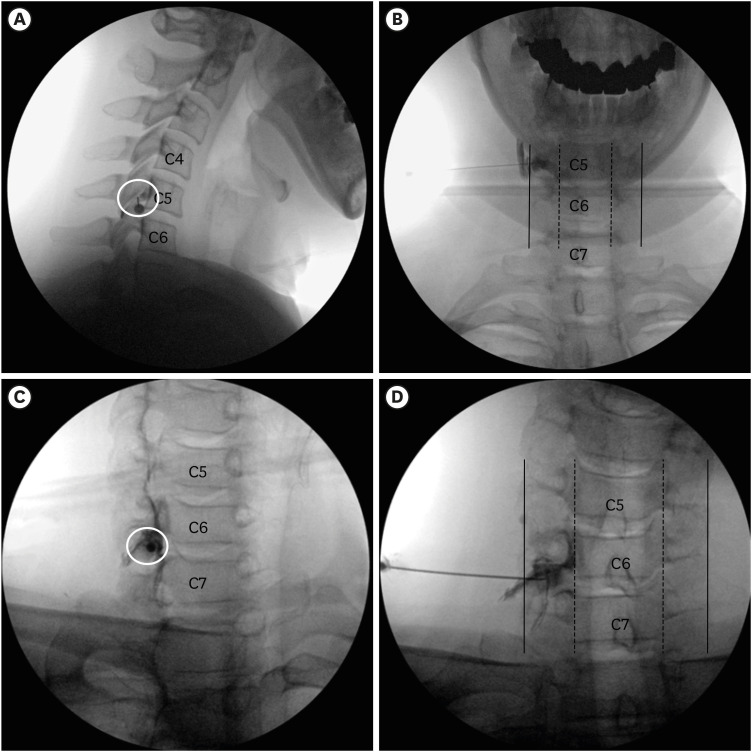 | Fig. 1Procedure of cervical facet joint and transforaminal epidural steroid injections. (A) Lateral and (B) AP view of needle position and the spreads of contrast media in the cervical facet joint steroid injection. (C) Oblique and (D) AP view of needle position and the spreads of contrast media in the cervical transforaminal epidural steroid injection. Circle: needle entry site, Line: articular pillar’s lateral border, Dashed line: articular pillar’s medial border.AP = anteroposterior.
|
The TFE steroid injection was aseptically performed using fluoroscopic guidance with a 22 ga, 2.5-inch Tuohy needle. The participants were in a supine position on a fluoroscopy table, and the C-arm was rotated between 45° and 55° obliquely to the ipsilateral side for visualization of the neural foramen with maximum transverse width. The appropriate entry site was posteriorly in the foramen at the division between the caudal and middle thirds. This was marked on the skin. The skin and subcutaneous tissue were anesthetized with 1% lidocaine. The Tuohy needle was advanced to the superior articular process via the tunnel vision technique. Then the needle was advanced into the neural foramen, touching its posterior border at the halfway point between the articular pillars’ medial and lateral borders in AP fluoroscopy. The needle should not be advanced beyond this point. The needle position was confirmed by real-time fluoroscopy with 0.5–1.0 mL of a contrast media (Fig. 1C and D). Intravascular injection was confirmed by diffusion of the contrast media through the vascular channel. Then, we injected 2 mL of a solution mixed with 0.5% lidocaine and 2.5 mg dexamethasone. The subjects were observed for 30 minutes post-procedure.
During the follow-up period, if the patient satisfaction score was equal to or above “good,” but the improvement of NRS score was < 50%, the injections were repeated at least two weeks apart. No additional injections were administered if the NRS score was 3 or less. If there was no pain relief or the pain worsened, or if the patient satisfaction rating was equal to or below “fair,” other treatments such as increasing the dose of analgesics, invasive procedures, or surgery were considered. “Excellent” indicated that the patient was ‘satisfied with the outcome, and the treatment was as effective as expected’; “good” indicated ‘not as effective as expected but willing to take the treatment again when the pain recurs’; and “fair” indicated ‘some effect but not enough to choose the treatment again when the pain recurs’; and “bad” indicated ‘same or worse effect as the previous treatment.’16
Clinical data review
A standardized chart abstraction form was used to extract data on demographics, treatments, pain severity, and functional assessments. Follow-up interviews were conducted during hospital visits one, three, and six months after the initial injection by nursing personnel not involved in the injection procedure.
The primary outcomes included NRS scores for pain and functional disability. The degree of functional disability was measured using the Korean version of the Neck Disability Index (NDI; range, 0–50), which is the most widely used questionnaire assessing cervical spine abnormalities.1718 It consists of 10 questions, including seven questions related to functional activity, two questions about symptoms, and one question about concentration. The final score is obtained by summing the scores of all the questions. A higher NDI score indicates increased functional disability associated with cervical abnormality.17 Additionally, a subgroup analysis was performed to divide patients into moderate (NRS scores 4–6) and severe (NRS scores > 7) pain groups based on baseline pain scores.19
The secondary outcomes included the proportion of responders and the Medication Quantification Scale (MQS) score. A “responder” was defined as a patient experiencing a ≥ 50% improvement in their NRS score and a ≥ 40% or more improvement in their NDI score.1720 Patients who did not show this degree of improvement and those who required more analgesics, other invasive procedures, or surgery during the follow-up period were categorized as non-responders. We used the MQS to quantify medication use.21 The scores were calculated for each pain-related medication based on weights assigned by pharmacologic class and dosage level and were summed to yield the total MQS score.
The variables correlating with effectiveness one month after the initial injection were also evaluated. Independent variables, including the injection method, age, sex, number of injections, FS severity, MQS, pain duration, and the presence of CDH were documented in the medical charts. Age was classified into five groups: < 39, 40–49, 50–59, 60–69, and > 70 years. FS severity was classified into two grades according to routinely obtained cervical axial MRI findings based on Kim et al.22 (Fig. 2). Grade 1 included patients with non-severe FS, in which the narrowest width of the neural foramen was ≥ 50% of the width of the extraforaminal nerve root at the anterior margin of the superior articular process. Grade 2 included patients with severe FS, in which the narrowest width of the neural foramen was < 50% of the extraforaminal nerve root. MQSs were divided into two groups (≤ 3 and > 3).23
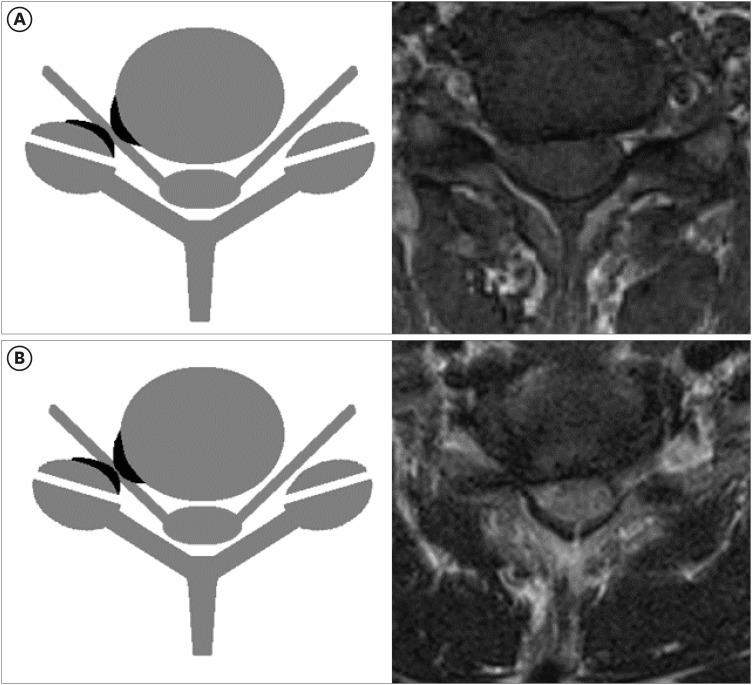 | Fig. 2Grading for cervical neural foraminal stenosis. (A) Grade 1, non-severe cervical neural foraminal stenosis, including the narrowest width of the neural foramen < (but > 50% of) the extraforaminal nerve root width. (B) Grade 2, severe cervical neural foraminal stenosis, including narrowest width of neural foramen same as or less than 50% of extraforaminal nerve root width.
|
Finally, we reviewed the charts for immediate side effects, such as vasovagal reactions, facial flushing, or brief, severe neck pain within minutes of injection, and any complications that occurred after the procedure (e.g., motor weakness, sensory change, infection, or hematoma) at the one-month follow-up visit.
Statistical analysis
The Shapiro-Wilk test was used to check the normal distribution of continuous variables. Continuous variables are represented as mean ± SD or medians (interquartile ranges), and categorical variables are displayed as numbers (percent). The Student’s t-test and Pearson’s χ2 test were used to compare the characteristics of the FJ and TFE groups regarding age, sex, number of injections, side of symptoms, target level, FS severity, MQS, pain duration, and the presence of CDH. At each time point (before the first injection and one, three, and six months after the initial injection), the NRS and NDI scores and MQS were compared by repeated-measures analysis of variance (ANOVA) with Bonferroni’s correction for post hoc comparisons. Univariate and multivariate logistic regression analyses with Pearson’s χ2 test were performed to assess whether the injection method, age, sex, number of injections, FS severity, MQS, pain duration, and the presence of CDH were independent predictors of treatment success. All data were statistically analyzed using Statistical Package for the Social Sciences (SPSS) version 23.0 (IBM Corp, Armonk, NY, USA). P < 0.05 was considered statistically significant.
Ethics statement
The Institutional Review Board centers of Ewha Womans University Seoul Hospital (SEUMC 2021-11-034) and Ewha Womans University Mokdong Hospital (EUMC 2021-12-035) approved the study. Since this study did not involve direct contact with the study population, the approval included a waiver of informed consent.
Go to :
RESULTS
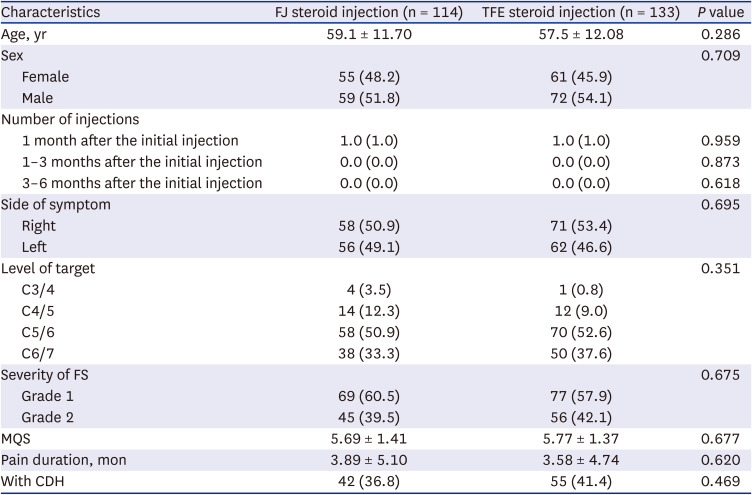
Of the 278 injections administered during the study period, including 130 FJ and 148 TFE steroid injections, 247 met the inclusion criteria and 31 were excluded. Ultimately, 114 and 133 patients received the FJ and TFE steroid injections, respectively (Fig. 3). Patient demographics and characteristics are shown in Table 1. There were no significant differences between the two groups in age, sex, number of injections, side of symptoms, target level, FS severity, MQS, pain duration, and the presence of CDH.
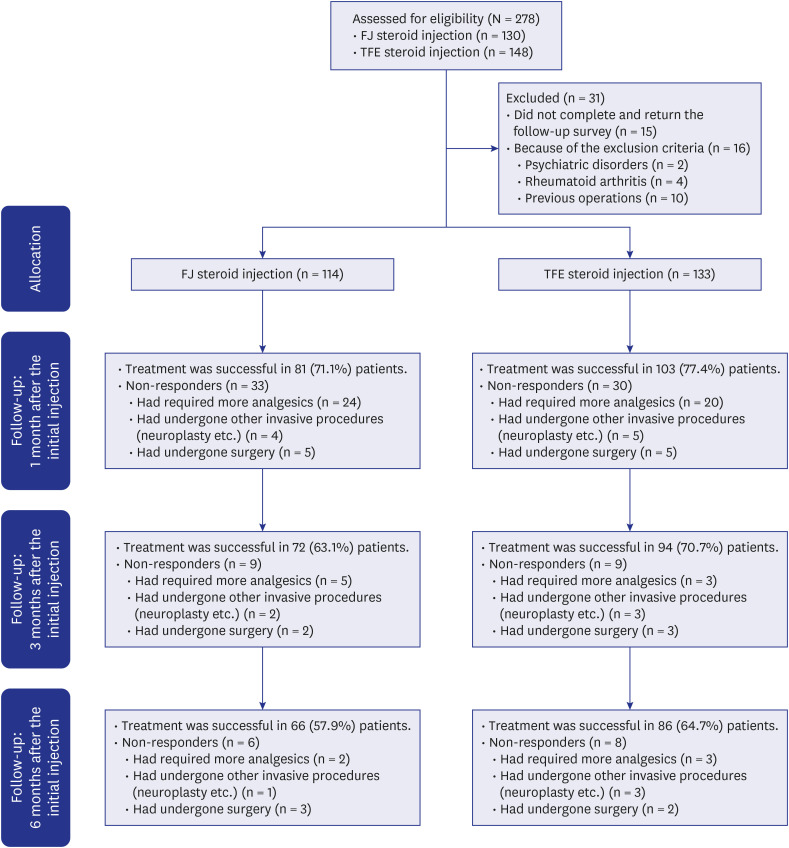 | Fig. 3Flow diagram indicating patient progress through the study.FJ = facet joint, TFE = transforaminal epidural.
|
Table 1
General patient characteristics
Values are presented as mean ± standard deviation, median (interquartile range: P25–P75), or number of patients (%).
CDH = cervical disk herniation, FJ = facet joint, FS = foraminal stenosis, MQS = Medication Quantification Scale, TFE = transforaminal epidural.
![]()
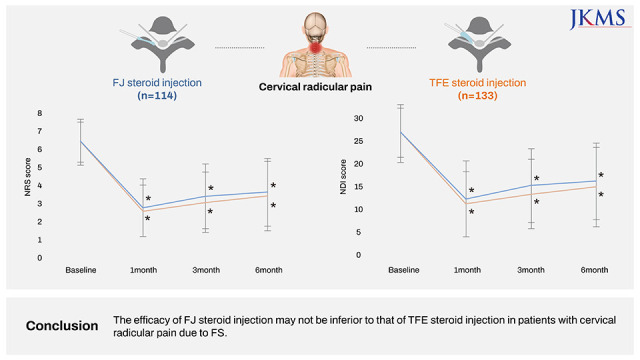
The NRS and NDI scores showed a significant improvement at one, three, and six months after the initial injection in both groups, with no significant differences between the groups during the follow-up period (Fig. 4). In the subgroup analysis, there was no significant difference in NRS and NDI scores between the two groups, except that the NRS and NDI scores of the severe pain group were significantly lower in TFE than FJ steroid injections three months after the initial injection (Fig. 5).
 | Fig. 4Pain scores and functional disability. (A) NRS scores. (B) NDI scores.FJ = facet joint, NDI = Neck Disability Index, NRS = Numeric Rating Scale, TFE = transforaminal epidural.
aP < 0.05: comparison of each variable at a specific time point with baseline.
|
 | Fig. 5Sub-group analysis. (A) NRS and (B) NDI scores of the severe pain group. (C) NRS and (D) NDI scores of the moderate pain group.FJ = facet joint, NDI = Neck Disability Index, NRS = Numeric Rating Scale, TFE = transforaminal epidural.
aP < 0.05: comparison of each variable at a specific time point with baseline; bP < 0.05: comparison of differences between the groups.
|
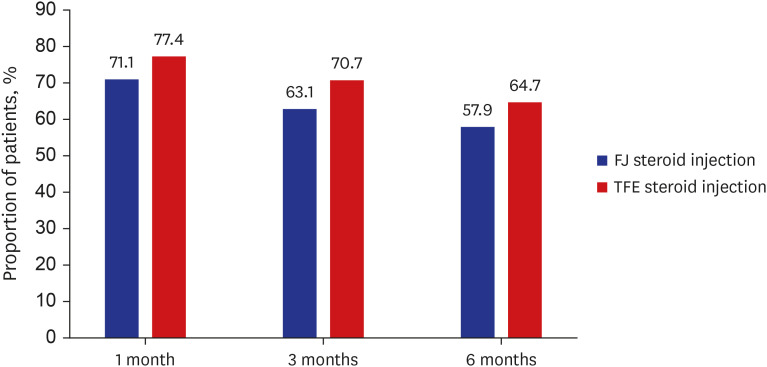
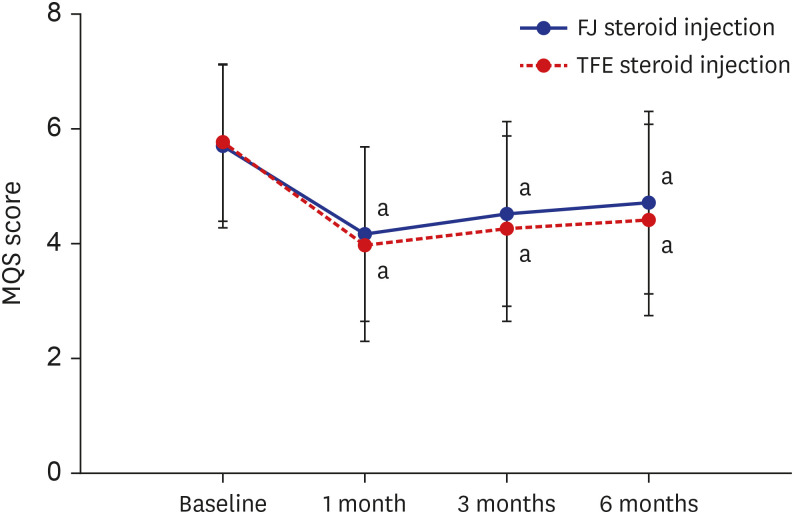
Given the definition of a “responder,” no significant differences were observed in the success rates of the procedure at one, three, and six months after the initial injection for either group (Fig. 6). The MQS was also not significantly different between groups at baseline or one, three, and six months after the initial injection (Fig. 7).
Univariate and multivariate logistic regression analyses revealed that the injection method, age, sex, number of injections, FS severity, MQS, pain duration, and the presence of CDH were not independent predictors of treatment success (P > 0.05; Tables 2 and 3).
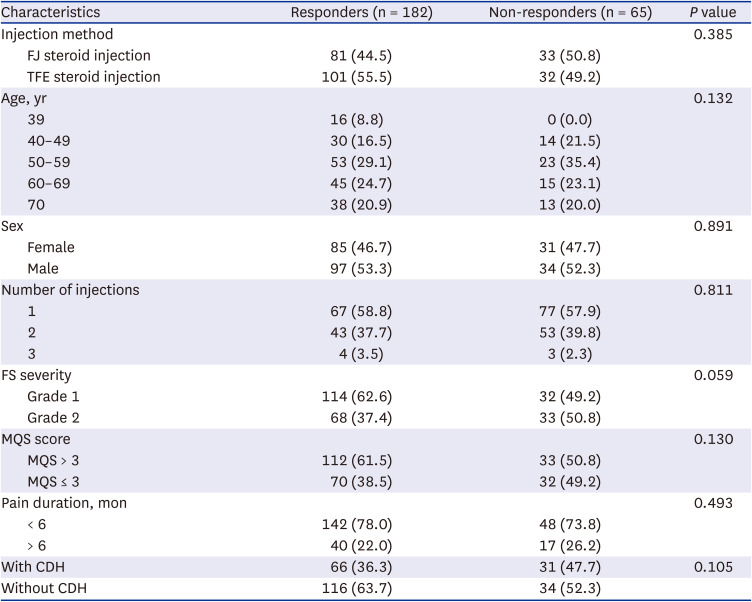
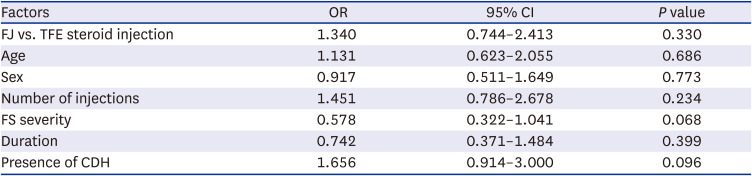
Table 2
Univariate analysis for possible outcome predictors of injection effectiveness
Values are presented as number of patients (%).
FJ = facet joint, TFE = transforaminal epidural, FS = foraminal stenosis, MQS = Medication Quantification Scale, CDH = cervical disk herniation.
![]()
Table 3
Multiple logistic regression analysis for possible outcome predictors for injection effectiveness
FJ = facet joint, TFE = transforaminal epidural, FS = foraminal stenosis, CDH = cervical disk herniation, CDH = cervical disk herniation.
![]()
Immediately after the procedure, three patients in the FJ group and two in the TFE group experienced vasovagal symptoms, and one patient in the FJ group and three in the TFE group experienced transient headaches (P > 0.05). Overall, at the one-month follow-up, three patients in the FJ group and four in the TFE group reported temporary exacerbations of pain 48 hours after the procedure. No cases of infection or hematoma were recorded during the one-month following the procedure.
Go to :
DISCUSSION
The purpose of this study was to evaluate the hypothesis that FJ steroid injection’s efficacy is not inferior to that of TFE steroid injection in patients with cervical radicular pain due to FS. Our results showed that the FJ and TFE steroid injections demonstrated a significant decrease in the pain score and an improvement in functional status at one, three, and six months after the initial injection, with no significant differences between them.
Cervical neural FS, a common cause of radicular pain in the upper extremity, is a disorder marked by neural foraminal narrowing and mechanical compression of the nerve root.12 Ventral compression is mainly due to disc bulges or herniations and osteophytes, and motor neurons are often affected. Dorsal compression is mainly produced by metamorphic facets and ligamentum flavum, and the sensory neurons are often involved. Since cervical nerve roots are located in the inferior portion of the foramen from the spinal cord 4–8 mm below the intervertebral disc, nerve roots are well protected, and hypertrophy and ossification of the FJ and ligament flavum are often pathogenic factors.2425
The compression of the nerve root causes an inflammatory response in which various inflammatory mediated cells and cytokines are implicated and cause radicular pain.12 The main effect of the TFE steroid injection is the reduction of the production and release of inflammation-related mediators, which inhibits the processes, leading to radicular pain. In addition, reducing this inflammation suppresses the edema at the nerve root or the tissues around the nerve root, decreasing compression of the nerve root.1726 However, the accidental injection of particulates into the blood vessels during TFE steroid injection can lead to serious complications, such as vertebrobasilar brain and cervical spinal cord infarcts.927 Meanwhile, a prospective study of 43,000 FJ injections illustrated that major complications, such as nerve damage, spinal cord stimulation, epidural hematoma, and infection, were extremely rare, proving the stability of the FJ injections.28
To the best of our knowledge, there are few studies on the effectiveness of FJ steroid injections. According to Dwyer et al.,29 FJ injection may require the skillful injection of the needle into a narrow joint space and can be more traumatic than a medial branch block. Cervical FJ injections have not been standardized because proper visualization of cervical anatomy using fluoroscopy can be difficult.3031 In addition, the angles and morphological properties of FJ in the cervical region have not been fully evaluated.32
There is only one RCT for FJ steroid injections in cervical radicular pain. Bureau et al.6 compared the efficacy of FJ and TFE steroid injections for the treatment of cervical radicular pain and reported that FJ steroid injection was at least as effective as TFE steroid injection in providing pain relief when the baseline pain severity score was low-to-moderate. They concluded that FJ steroid injection was a valid and safer alternative to TFE steroid injection in patients with cervical spondylosis with or without CDH. Their results were similar to ours in that there were no significant differences in reduction of the pain score and an improvement of functional status at one, three, and six months after the initial injection. They reported that the comparison between the two interventions remained inconclusive for a severe baseline pain level6; this also may be consistent with our subgroup analysis showing that NRS and NDI scores in the severe pain group were significantly lower in the TFE than the FJ steroid injections three months after the initial injection.
However, there are some differences between their study and our study. First, they enrolled a relatively small number of patients (a total of 56 subjects), which may have been insufficient to determine differences in meaningful pain relief and functional disability. Second, while short-term effects are also meaningful, they did not investigate long-term outcomes. Third, they included patients with spondylosis with or without CDH, but we enrolled patients with cervical radicular pain caused by FS. Fourth, we repeated injections according to established criteria (satisfaction score is above “good,” but improvement in NRS score is < 50%). Fifth, we conducted a multicenter study.
It is difficult to understand the exact mechanism underlying the effectiveness of FJ steroid injection in cervical radicular pain. Several studies suggested that the proximity of the facet joint ventral capsular recess to the intervertebral foramen and/or leakage of the medication from the facet joint into the epidural and/or foraminal spaces could contribute to the effectiveness of the FJ steroid injection. Kelekis et al.13 demonstrated an efficacious, feasible, and indirect cervical nerve root injection technique: puncture of the facet joint capsule with subsequent distribution of the corticosteroid intraarticularly, periradicularly, and within the epidural space. Won et al.33 mentioned that extra-FJ flow, including epidural leakage, showed high frequency at the lower cervical vertebrae, where there are many strains of capsular ligaments subject to peak FJ compression due to sliding.
Similar results have been reported in the lumbar FJ injection. Won et al.34 described that aberrant patterns of contrast flow, including epidural leakage, may be frequently observed. The epidural leakage was considered the result of facet joint capsule rupture. In such cases, an epidural injection may be considered as an alternative approach. Hwang et al.35 reported that 83.3% of patients who received lumbar FJ injections exhibited epidural spread of the contrast agent. They suggested that indirect epidural diffusion of the drug could contribute to pain reduction in patients with lumbar radiculopathy. Further, Yoo et al.36 performed lumbar FJ injections on 192 patients and reported that 64.6% of them were visually confirmed as epidural spread by analyzing the fluoroscope view.
The FJ is a synovial joint located between the articular processes of adjacent vertebrae and has a simple shape in the cervical and thoracic vertebrae but a more complex shape in the lumbar region. Its articular capsules are generally thin and loose, but they seem longer, looser, and thinner in the cervical region.33 Although the previous RCT6 and our study suggest that FJ steroid injection can be a valid and safe alternative to TFE steroid injection in patients with cervical radicular pain, FJ steroid injection may cause iatrogenic damage to the FJ capsule.34 Therefore, incorporating the FJ steroid injection in patients with cervical radicular pain should be at the physician’s discretion.
Our results showed no significant difference in the success rates of cervical FJ and TFE steroid injections based on the degree of FS. Kim et al.5 reported that the pain of the participants decreased regardless of the severity of cervical FS, and that there was no difference in the treatment results of TFE steroid injection between the non-severe FS and severe FS groups. Moreover, in 53 patients with cervical FS, there were no significant differences in the effects of TFE steroid injection between patients with non-severe and severe FS.1 Stafford et al.37 demonstrated that mechanical pressing of a nerve root without inflammation could lead to neurological deficits rather than radicular pain. Inflammation of the nerve root played a role in initiating the process leading to pain. The degree of inflammation, not FS, was thought to be a major factor influencing the intensity of radicular pain.1
The present study has several limitations. First, its retrospective design could have resulted in heterogeneity among the study participants. However, any shortcomings related to heterogeneity are limited because of the standardization of the patient demographics and clinical and imaging parameters before treatment and at each follow-up visit. Second, we could not exclude other treatments, such as physical therapy, from our study during the follow-up period. Third, NDI is mostly used to evaluate functional status because there are no specific outcome measures in patients with cervical radicular pain,1718 but NDI does not fully represent the therapeutic outcomes of functional disability.
In conclusion, our results showed that there is no significant difference in the pain reduction and functional improvements between FJ and TFE steroid injections. Therefore, the efficacy of FJ steroid injection may not be inferior to that of TFE steroid injection in patients with cervical radicular pain due to FS. Using the FJ approach to deliver steroids in the vicinity of the affected spinal nerve root appears to be a viable alternative to the TFE approach.
Go to :
 XML Download
XML Download