

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Medical doctors who undergo training to become specialists are called residents. This term was developed because these doctors tend to mostly reside most of the time at the hospital. Residents carry out two difficult roles: as medical doctors who treat patients and as trainees in learning clinical medicine. Thus, they are always exposed to various job-related stressors, such as long working hours, irregular work schedule, frequent night shift work, on-call work, high job demand, and insufficient job control.12 These occupational stressors increase the risks of depression, sleep disorder, fatigue, and metabolic syndrome.123456 Long working hours are also associated with smoking, alcohol consumption, and lack of exercise.7 Lack of sleep, fatigue, burnout, and unhealthy lifestyle of residents increase the risk of occupational injury at the workplace, which is directly related to patient safety.8910
Many studies have reported that extended working hours and working night shifts have a negative effect on health.11121314 In Korea, several studies on the residents’ training environment have been conducted. However, most of the studies were questionnaire-based studies. No study has assessed the objective health indicators of medical residents.151617 We aimed to analyze the 4-year annual health checkup (AHC) data of residents at a university hospital to identify changes in their health status and related factors.
Go to : 
METHODS
Participants
This study was conducted in medical residents working in a university hospital. The subjects enrolled in this study in the first year of their resident training between 2007 and 2013. The training period for medical residents was four years, which was the same for all. The AHC data of 699 residents from 2007 to 2016 were collected. Female residents (n = 187) were excluded because information regarding pregnancy, abortion, and childbirth, which significantly influences their health status, was not obtained. Additionally, 55 workers who did not undergo AHC properly or whose information was missing were excluded. Finally, 457 male residents were included as the study subjects.
Study variables
The subjects were categorized into the surgical, medical, and clinical support departments as per the characteristics of each department. General surgery, neurosurgery, obstetrics and gynecology, ophthalmology, orthopedic surgery, otorhinolaryngology, plastic and reconstructive surgery, thoracic and cardiovascular surgery, and urology were classified under the 1) surgical department. Dermatology, emergency medicine, internal medicine, neurology, neuropsychiatry, occupational and environmental medicine, pediatrics, and rehabilitation medicine were classified under the 2) medical department. Laboratory medicine, nuclear medicine, pathology, radiation oncology, anesthesiology and pain medicine, and radiology were classified under 3) clinical support department. Among the 457 participants, 188 (41.1%) worked in the surgical department; 199 (43.5%), medical department; and 70 (15.3%), clinical support department.
As the law for improving the training environment and status of the residents was not enforced in 2016, duty schedules at the hospital were reviewed and the data of mean working hours per week were obtained. Departments with mean working hours per week of < 80 hours were anesthesiology and pain medicine, dermatology, laboratory medicine, neuropsychiatry, nuclear medicine, occupational and environmental medicine, otorhinolaryngology, pathology, pediatrics, radiation oncology, radiology, and rehabilitation medicine. Departments with mean working hour per week of ≥ 80 hours were emergency medicine, general surgery, internal medicine, neurology, neurosurgery, obstetrics and gynecology, ophthalmology, orthopedic surgery, plastic and reconstructive surgery, thoracic and cardiovascular surgery, and urology.
Outcome variables
The test categories of AHC in this study were height, weight, systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting blood glucose (FBG), aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma glutamyl transpeptidase (γ-GTP), and total cholesterol (TC). Information on smoking, drinking, exercise, and medical history were obtained through interviews. Blood tests were performed after 12 hours of fasting. Subjects who had smoked less than five packs of cigarettes in their life were classified as never smokers, whereas those who had stopped smoking and those who smoked currently were classified as ex-smokers and current smokers, respectively. According to the drinking status, residents were classified as drinkers (who consumed > 20 g of alcohol per week) and non-drinkers. Residents were considered to perform regular exercise if they exercised for > 30 minutes a day at least twice a week. Body mass index (BMI) was calculated using the following formula: weight (kg)/height2 (m2).
Statistical analyses
Continuous variables such as BMI, SBP, DBP, FBG, AST, ALT, γ-GTP, and TC levels were compared using the paired t-test, Student t-test, analysis of variance, and Kruskal-Wallis test. Categorical variables such as smoking, drinking, and frequency of exercise were compared using the Pearson χ2 test. We compared the differences between the results of the 1st and 4th AHCs by department and working hours using analysis of covariance (ANCOVA). Models were adjusted for covariates including age (continuous), working hours per week (continuous), smoking (yes/no), alcohol consumption (yes/no), regular exercise (yes/no), and working department (surgery department: yes/no). SPSS version 26.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. Statistical significance was defined as P value < 0.05.
Ethics statement
The protocol of this study was approved by the Institutional Review Board (IRB) of Chonnam National University Hwasun Hospital (IRB number CNUHH-2018-050). We conducted a retrospective review of the participants’ medical records. The participants’ data were anonymized and stored in the Chonnam National University Hospital Clinical Data Warehouse (CDW). The data were used for research purposes in accordance with the Personal Information Protection Act. Each participant provided electronic informed consent regarding the collection and use of personal information before the checkup was conducted.
Go to :
RESULTS
All the 457 residents who participated in this study were male. We analyzed the health indicators during the 4-year resident training period. The AHC results in the first (1st AHC) and fourth (4th AHC) year of training were compared. The average working hours per week decreased as the resident grade went up, and the difference was statistically significant. BMI, SBP, DBP, AST, ALT, γ-GTP, and TC levels significantly increased in the 4th year AHC as compared to those in the 1st year AHC. The difference between the recent AHC results was compared with the previous year’s AHC results. Compared to the other years, the difference between the first and second years of training showed the highest increases in BMI and ALT, γ-GTP, and TC levels, all showing statistical significance (Table 1).
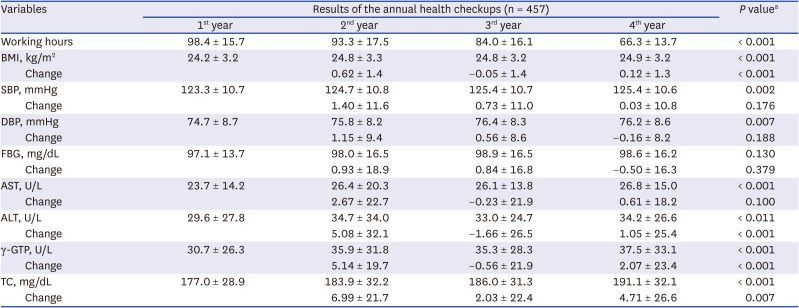
Table 1
Comparison of changes in the health indicators during four-year medical resident training period
Values are presented as arithmetic mean ± standard deviation.
BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, FBG = fasting blood glucose, AST = aspartate aminotransferase, ALT = alanine aminotransferase, γ-GTP = gamma glutamyl transpeptidase, TC = total cholesterol.
aP value was calculated using paired t-test between 1st year and 4th year annual health checkup results or ANOVA between the changes.
![]()
We analyzed the health behaviors during the 4-year resident training period. The number of smokers and drinkers decreased in the 4th year as compared to those in the 1st year of training. The smoking (21.0%) and drinking (85.8%) proportions in the 2nd year were the highest, and those in the 4th year were the lowest, at 16.0% and 79.4%, respectively. However, the differences were not statistically significant. The proportion of participants performing regular exercise increased from 35.7% to 68.5%, showing a statistically significant difference (P < 0.001) (Table 2).

Table 2
Comparison of changes in the health behaviors during four-year medical resident training period
![]()
The difference between the 4th and 1st AHC results was compared by department. BMI, DBP, and AST, ALT, γ-GTP, and TC levels showed the highest increases in the residents of the surgical department, which were statistically significant. Additionally, SBP and FBG levels showed the greatest increases in the residents of this department, but this was not statistically significant. In the surgical department, the decrease in the proportion of smokers was the lowest and the increase in the proportion of drinkers was the highest, and these differences were statistically significant. The proportion of those who exercised regularly showed the highest increase in the medical department, but this was not statistically significant (Table 3).
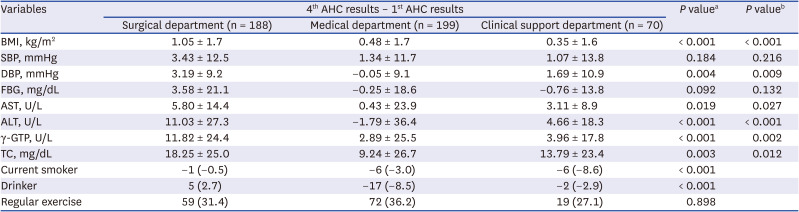
Table 3
The difference between the results of the 1st and 4th AHCs by department
Values are presented as arithmetic mean ± standard deviation or number (%).
BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, FBG = fasting blood glucose, AST = aspartate aminotransferase, ALT = alanine aminotransferase, γ-GTP = gamma glutamyl transpeptidase, TC = total cholesterol.
aP value was calculated using analysis of variance (ANOVA), or Pearson χ2 test; bP value was calculated by analysis of covariance (ANCOVA) and adjusted for age, working hours per week, smoking, alcohol consumption, and regular exercise.
![]()
A total of 134 residents (29.3%) worked < 80 hours per week and 323 worked > 80 hours per week (70.7%). The difference between the 4th and 1st AHC results according to working hours per week was also compared. FBG and AST levels significantly increased in the residents who worked ≥ 80 hours per week compared to those who worked < 80 hours. BMI, SBP, DBP, ALT, and γ-GTP levels were also increased in the residents who worked ≥ 80 hours per week compared to those who worked < 80 hours, but this was not statistically significant. In the residents who worked ≥ 80 hours per week, the decrease in the proportion of smokers was higher, and this difference was statistically significant. There were no significant differences between the two groups with respect to the proportions of alcohol consumers and regular exercisers (Table 4).
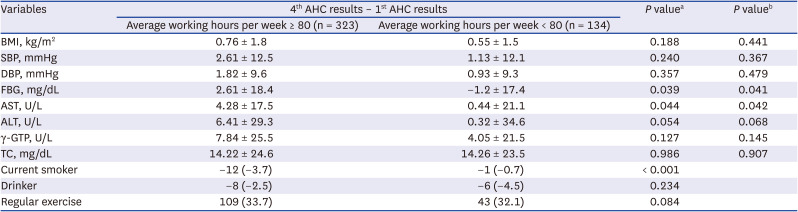
Table 4
The difference between the results of the 1st and 4th AHCs of medical residents by working hours
Values are presented as arithmetic mean ± standard deviation or number (%).
AHC = annual health checkup, BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, FBG = fasting blood glucose, AST = aspartate aminotransferase, ALT = alanine aminotransferase, γ-GTP = gamma glutamyl transpeptidase, TC = total cholesterol.
aP value calculated by Student t-test or Pearson χ2 test; bP value was calculated by analysis of covariance (ANCOVA) and adjusted for age, smoking, alcohol consumption, regular exercise, and working department.
![]()
Go to :
DISCUSSION
Workers’ working hours are gradually decreasing worldwide.18 In July 2018, the legal maximum working hours per week in South Korea were reduced to 52 hours from 68 hours. However, the medical service fields were exempted, and the maximum working hours have not been set. The characteristics of unhealthy working environments, such as long working hours, persist. Among the healthcare workers in Korea, medical residents’ working hours are long, and the workload intensity is also remarkably high. Such long working hours and high workload intensity have led to various social issues, such as medical malpractice and suicide.1920 As a result, a law for improving the training environment and status of the residents was enforced in 2017. This new law limits the maximum working hours per week to 88 hours for medical residents; however, this is still higher than that for most workers.21
In this study, the residents’ average working hours and night shift work per week were 85.5 hours and 2.4 days, respectively. Kim et al.’s study15 on Korean residents showed that the average working hours and night shift work per week were 87.3 hours and 2.6 days, respectively. Such long working hours and frequent night shift work can lead to a lack of adequate sleep, insufficient exercise, and inappropriate dietary habits, which more likely promote worsening of health indicators during resident training. On comparing the AHC results with those of the previous year, the highest deterioration was observed between the 1st and 2nd AHCs. Kim et al.15 reported that the workload is not consistently divided among the years of the training period. Thus, the working hours are longer in the early years of training, in the following order: 1st year (105.0 hours), 2nd year (98.5 hours), 3rd year (86.0 hours), and 4th year (77.2 hours) of the training period.15 Our study also showed similar results, in the following order: 1st year (98.4 hours), 2nd year (93.3 hours), 3rd year (84.0 hours), and 4th year (66.3 hours) of the training period. Working hours per week and the number of night shift workdays decreased as the years of training increased. In addition, the number of residents who exercised > 30 min a day at least twice a week increased as the years of training increased. As working hours and the number of night shift workdays decreased and the number of training years increased, residents were likely to have relatively more time to exercise. Efforts are required for distributing the heavy workload of the residents during the early years of training.
Our study results showed that during the training period, BMI, SBP, DBP, AST, ALT, γ-GTP, and TC levels of the medical residents significantly increased; these deteriorations were relatively high in the early period of training. On comparing by department, the residents in the surgical department showed the highest increase as compared to those in the medical and clinical support departments. On comparing by working hours per week, FBG and AST levels significantly increased in residents who worked ≥ 80 hours per week compared to the levels in those who worked < 80 hours. As the years of training increased, the proportions of smokers and drinkers decreased, whereas that of participants performing regular exercise increased. Hence, the proportion of participants performing health activities increased with increasing years of training.
In this study, the average working hours per week were 92.8 hours, 77.8 hours, and 87.8 hours in the surgical, medical, and clinical support departments, respectively. Kim et al.15 also reported similar results: 93.5 hours, 84.3 hours, and 82.4 hours in the surgical, medical, and clinical support departments, respectively. Additionally, Kim et al.,22 who analyzed the obesity pattern of doctors, reported that the proportion of obese doctors was the highest in the surgical department. In a previous study, dietary habits were also investigated. Obesity and overweight were associated with short hours of sleep, insufficient exercise, and inappropriate dietary habits.232425 Many studies have reported that obesity and overweight cause elevations of blood pressure, FBG level, liver enzymes, and cholesterol levels.2627282930 Due to the characteristics of the working environment, including surgeries, night shift work, and emergency patient treatment, doctors in the surgical department had poor dietary habits, such as irregular eating hours and late-night snacking.22 The long working hours and poor dietary habits of surgical residents seem to have resulted in poor AHC results compared to those in other departments. On comparing by working hours, working ≥ 80 hours had a worsening effect on health indicators compared to working < 80 hours. The long working hours and poor dietary habits most likely had worsening effects on the health indicators of the surgical department residents.
There are some limitations in this study. First, information about other confounders such as psychological factors and dietary habits were not obtained. Moreover, psychological states such as depression and stress were not evaluated. Depression has been reported to increase BMI and promote hypertension.3132 In particular, the prevalence of depression in residents has been reported to be higher than that in the general population.33 Further studies should also assess the dietary habits and psychological health status of the residents. Second, the 1st AHC of this study was conducted approximately 6 months after the starting the 1st year of resident training. Because the relatively highly stressful early periods in the 1st year of resident training and the one-year intern training period were excluded, the results may have been underestimated. Third, women were excluded from this study because information on pregnancy, childbirth, and abortion that can greatly affect their health status was not obtained. The study was conducted in male residents only; thus, the study results cannot be generalized. However, since the various health problems of women residents are also an important issue, and the health of women residents may be more vulnerable, it is essential to evaluate them.343536 Well-designed studies for the women residents in the future will also be required. Fourth, there was no external comparison group in the study. Although the comparative analysis was conducted by year, by department, and by working hours through internal comparison, it is necessary to select control subjects who have proper working times and no shift work as an external comparison group in further studies. Fifth, the study participation period of the subjects was long, from 2007 to 2013. There might have been changes in the working environment during this period. However, when the study participants were further analyzed by classifying them according to the time of participation, there were no variables showing a statistically significant difference. Lastly, this study was conducted based on the residents of a university hospital. The training environment and system differ greatly depending on the hospital; thus, the results of this study cannot be generalized. A study on all residents nationwide should be conducted in the future.
Lack of sleep is associated with high stress levels, attention deficit, and learning disorders, and cognitive–motor performance after 24 hours of continuous awakening is decreased to a level similar to that of blood alcohol at approximately 0.10%.3738 Studies have shown that insufficient sleep influences the occurrence of medical malpractice while dealing with surgery, anesthesia management, and difficult clinical symptoms.3940 In the United States, resident duty hours of > 80 hours per week, averaged over a four-week-period, are prohibited, whereas in Europe, resident working hours per week are restricted to 48 hours only.4142 In Korea, the maximum working hours per week of the residents are restricted to 88 hours after the amendment of the law for improving the training environment of and status of the residents in December 2017.21 However, Kim MK reported that 36% of the responders changed their work records to reduce the working hours from the actual schedule.15 There is still a gap between the law and reality in terms of unwanted long working hours and frequent night shift work. In order to reduce such gap, it is necessary to change the perception towards the fact that the health of the residents is as important as the health of the patient, along with effective work environment evaluation.43 Additionally, systematic management for the safety and health of residents is also considered necessary. This study was conducted before the enforcement of the law for improving the training environment and status of the residents. In the future, studies to assess changes in the health status after the enforcement of the law are required. We expect that the results of this study be used as a reference for policy research and establishing a healthy working environment for residents.
In summary, the medical residents’ health indicators significantly worsened, especially in the early training period, in surgical residents and in residents who worked long hours (> 80 hours per week). Efforts to restrict long working hours and distribute the workload during the four-year training period are required.
Go to :
 XML Download
XML Download