

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Approximately 15% of all pregnancies result in miscarriages. However, considering unrecognized biochemical pregnancies and early miscarriages, the prevalence may be as high as 60%.1 Although the definition of recurrent pregnancy loss (RPL) varies, it has been recently defined as more than 2 consecutive miscarriages. This definition excludes ectopic pregnancies, molar pregnancies, and implantation failure.23 RPL occurs in 1–5% of pregnancies and has adverse physical and emotional effects on couples who want to become pregnant.4
Because chromosomal abnormalities cause 75% of spontaneous abortions, both partners must undergo karyotypic evaluation.5 In addition, RPL can also be related to uterine malformations, endocrine diseases such as thyroid disease or diabetes, and autoimmune disorders such as thrombophilia or antiphospholipid syndrome (APS). Therefore, patients with RPL should be carefully examined and treated accordingly.6 However, the cause of RPL remains unknown in approximately 40–60% of the cases (unexplained recurrent pregnancy loss, URPL). These cases are mainly associated with dysregulations of the immune system or micro-thrombosis, and several studies have been conducted on this topic.7
Immunological imbalances in the uteroplacental interactions can cause implantation failure and lead to miscarriage. To date, the identified causes of alloimmune disorders include increased levels of natural killer (NK) cells,8 imbalances in T helper (Th) cells,9 and dysregulation of cytokines.10 Intravenous immunoglobulin G (IVIG) is a nonspecific immune modulator studied since 1994, when it was implemented as a treatment for RPL. IVIG has been used to treat autoimmune and inflammatory diseases such as idiopathic thrombocytopenic purpura, Guillain-Barré syndrome, and myasthenia gravis. Previous studies have shown that NK cell levels normalize upon IVIG administration in patients with RPL. However, the mechanism by which this occurs remains unknown.9 In 1996, Beer et al.11 first discovered that the peripheral blood NK cell proportion was higher than 12% (NK cell expansion) in patients with RPL. In subsequent studies, IVIG administration in a group of patients with RPL and expanding NK cells (NK cells ≥ 12%) decreased the NK cell levels and led to a 75–90% increase in pregnancy success rates.8121314151617 However, other studies have shown that IVIG treatment has no therapeutic effect.1819 A meta-analysis showed that IVIG treatment had no significant therapeutic effects (risk ratio for live birth in IVIG-treated patients = 1.17, P = 0.14).4
Hypercoagulability may be closely related to RPL. Aspirin, as an anticoagulant in patients with URPL, has been reported to increase the live birth rate and reduce late pregnancy complications.2021 Administration of low-dose aspirin can effectively prevent NK cell expansion-associated placental vascular changes, and antiphospholipid antibody syndrome.8
Currently, IVIG can be used only in patients with RPL and NK cell levels higher than 12%, following the IVIG use standards established by the Health Insurance Review and Assessment Service in 2017. However, studies have shown the differing effects of IVIG treatment in women with RPL, and to date, there are no specific guidelines for IVIG use. Interestingly, no study has evaluated the effectiveness of low-dose aspirin treatment in patients with RPL and NK cell levels lower than 12% (without NK cell expansion). Furthermore, most studies have involved patients with pregnancies achieved via assisted reproductive technology (ART). Therefore, the purpose of this study was to identify pregnancy outcomes in women with URPL who were empirically treated with IVIG combined with low-dose aspirin along with assessment of the possible association between the live birth rates and NK cells levels.
Go to : 
METHODS
Study setting and patients
The medical records of patients who had history of more than 2 consecutive miscarriages and were treated with IVIG and low-dose aspirin at Asan Medical Center from January 2000 to March 2020 were retrospectively analyzed. We defined miscarriage as pregnancy loss which has been confirmed as intrauterine miscarriage before 24 weeks of gestation.3 An initial fertility screening test was performed for all patients diagnosed with RPL and their partners. We excluded patients who met the following criteria: patients with a genetic abnormality or whose partner had a genetic abnormality, those with uterine structural malformations, those with endocrine diseases such as diabetes or thyroid disease, and those with coagulation and thrombophilia disorders. We also excluded patients with ectopic pregnancy, biochemical pregnancy, and recurrent implantation failure, because the purpose of the study was to determine whether IVIG combined with low-dose aspirin helps to maintain normal intrauterine implantation. In conclusion, we defined URPL as patients with a negative screening test for all of these exclusion criteria.
The following data were collected to evaluate the characteristics of the study population: age and number of previous miscarriages. The types of RPL were classified into primary RPL or secondary RPL. Primary RPL refers to recurrent miscarriages with no previous births, and secondary RPL refers to recurrent miscarriages that have previously experienced births or stillbirths. Pregnancy methods were divided as natural pregnancy, intrauterine insemination (IUI), in vitro fertilization-embryo transfer (IVF-ET), and frozen-thawed embryo transfer (FTET).
Pregnancy outcomes were either live birth or miscarriage. Both singleton and multiple pregnancies were defined as term delivery after week 37. Patients whose follow-up records were lost provided consent after the research was explained over the phone. The researcher compiled information regarding whether these patients gave birth, how many weeks pregnant they were when they gave birth, whether they had a healthy baby, and whether they had pregnancy-related complications. A total of 7 patients whose follow-up observations were lost underwent routine fetal ultrasound during their first and second trimesters and provided information about their pregnancy outcomes over the phone. In case of miscarriage, all patients aborted with normal intrauterine gestational sac without ectopic pregnancy. We collected the weeks at miscarriage, and the presence of fetal pole and fetal heartbeat on ultrasonography.
All patients diagnosed with RPL underwent screening tests for immunologic factors such as lupus anticoagulant, anticardiolipin IgG and IgM antibody, antinuclear antibody, anti-thyroid peroxidase antibody, and anti-thyroglobulin antibody. If there were any abnormal test results, autoimmune diseases were differentiated according to the findings of the rheumatologist or endocrinologist. We excluded patients who were diagnosed with autoimmune diseases and divided the remaining patients into autoantibodies positive (positive for at least one of the autoantibodies) or negative (completely negative for the autoantibodies) groups.
IVIG combined with low-dose aspirin treatment protocol
All patients diagnosed with URPL received IVIG at 0.2 g/kg or 10 g (fixed dose) every 2–3 weeks during the first trimester of pregnancy and then monthly IVIG until the end of the second trimester. IVIG treatment was started on the day that human chorionic gonadotropin quantification was confirmed, or the intrauterine gestational sac was identified on ultrasonography. In most cases, patients undergoing IVF-ET or FTET, IVIG administration began on the day of embryo transfer (ET). Some patients undergoing IUI started IVIG administration from the day of the IUI procedure according to the doctor’s opinion. In addition, patients diagnosed with URPL received low-dose aspirin (100 mg) as long as there was no bleeding, regardless of their NK cell fraction, from the date of confirmation of pregnancy or the day of ET to the end of the second trimester of pregnancy. In this study, we analyzed birth outcomes according to IVIG administration time by separating patients into groups administered before or after conception.
NK cell analysis
NK cell levels were measured in patients before natural conception attempts or before the initiations of ART, such as controlled ovarian hyperstimulation or hormone treatment for FTET. Antigen-positive cells were sorted from peripheral venous blood samples using FACSCantoTM II (Becton-Dickinson, San Jose, CA, USA) and monoclonal antibodies targeting lymphocyte surface antigens. The following stains were used: CD-3 fluorescein isothiocyanate, CD16-phycoerythrin (PE), CD56-PE, and CD45-allophycocyanin. The NK cell fraction was collected in CD-3/CD-16+CD-56 tubes and defined as a CD-3 negative and CD-16 and CD-56 positive. We defined NK cell expansion as an NK cell level higher than 12%.
Statistical analysis
Categorical variables are presented as percentages and were compared using χ2 and Fisher’s exact tests. Continuous variables were compared using Student’s unpaired t-test if the data were normally distributed as assessed by the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to compare continuous variables if the data were not normally. Statistical analyses were performed using SPSS, version 21 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered statistically significant.
Ethics statement
The study protocol was approved by the Institutional Review Board of Asan Medical Center (2020-0459). Informed consent was waived due to the retrospective and anonymous nature of the study and participants.
Go to :
RESULTS
Baseline patient characteristics and pregnancy outcomes
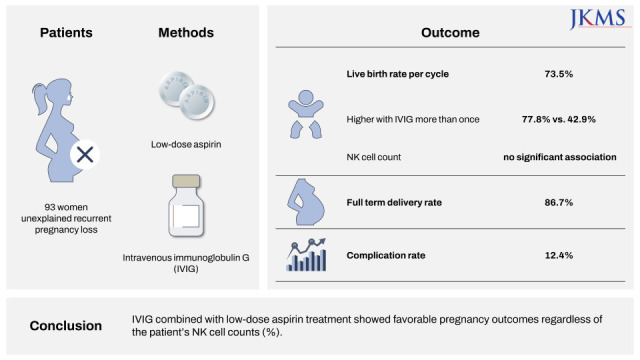
A total of 289 IVIG treatment cycles were screened, 176 cycles were excluded in accordance with the exclusion criteria. A total of 93 patients diagnosed with URPL and 113 pregnancy cycles were analyzed in the present study. The average patient age was 33.4 ± 3.75 years, and the average number of previous miscarriages was 3.1 ± 1.31. Most patients were primary RPL (73.3%). Of the 113 treatment cycles, the most common pregnancy method was natural cycle (62.8%), followed by IUI (17.7%) and IVF-ET (15.1%). Most patients received IVIG after confirmation of the pregnancy (78.8%). The live birth rate per cycle was 73.5%, and most infants were born at term (38.6 ± 1.0 weeks; 86.7%). Only 11 were born preterm (35.3 ± 1.9 weeks). Of the 7 cases of multiple pregnancies, all were healthy twins. There were no congenital malformations among newborn babies. The miscarriage rate per cycle was 26.5%, and most fetuses aborted in the first trimester of pregnancy before fetal heartbeat activity (46.7%) (Table 1).
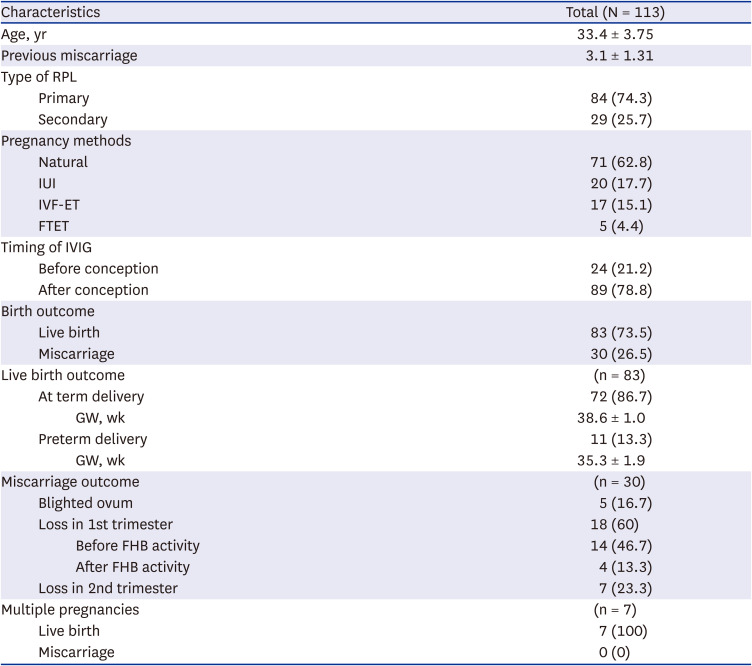
Table 1
Baseline patient characteristics
Values are presented as number (%) or mean ± standard deviation.
RPL = recurrent pregnancy loss, IUI = intrauterine insemination, IVF-ET = in vitro fertilization-embryo transfer, FTET = frozen-thawed embryo transfer, IVIG = intravenous immunoglobulin G, GW = gestational week, FHB = fetal heartbeat.
![]()
Efficacy of IVIG combined with low-dose aspirin in patients with URPL
Table 2 shows the comparison of live birth and miscarriage according to the subset of patients’ treatment with IVIG combined with low-dose aspirin. The live birth rate per cycle was higher than the miscarriage rate regardless of the type of RPL (primary RPL, 75%; secondary RPL, 69%, P = 0.526), pregnancy methods (natural, 71.8%; IUI, 85%; IVF-ET, 64.7%; FTET, 80%, P = 0.524), and timing of IVIG and aspirin administration (before conception, 70.8%; after conception 74.2%, P = 0.743). In addition, the live birth rate was comparable in patients who were completely negative for autoantibodies and positive for at least one of the autoantibodies (negative, 74.2%; positive 70.8%, P = 0.743). Most of the 113 cycles involved IVIG administration more than once (n = 99). Only 14 cycles received IVIG only once, and treatment was terminated in most cycles due to miscarriages (n = 8). Of the remaining 6 cycles, 2 cycles were discontinued because of hyperemesis and 1 cycle due to general weakness after IVIG administration. For the remaining 3 cycles, no specific reason for discontinuing the IVIG was found the records. The live birth rate was significantly higher in patients who received IVIG more than once, than in patients who received IVIG only once (77.8% [77/99] vs. 42.9% [6/14], P = 0.006). Of 113 cycles, only 62 had NK cell level measurements. The live birth rate was comparable between patients with and without NK cell expansion (69.7% [23/33] in NK cell levels ≥ 12%, and 65.5% [19/29] NK cell levels < 12%, P = 0.725).
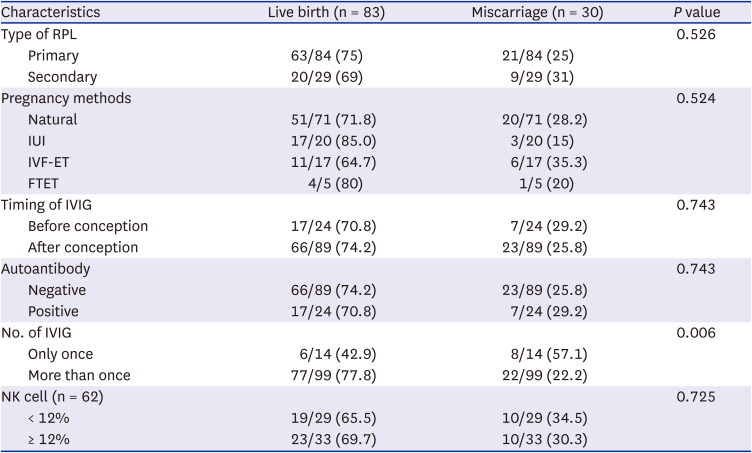
Table 2
Comparison of live births and miscarriages
Values are presented as ratio (%).
RPL = recurrent pregnancy loss, IUI = intrauterine insemination, IVF-ET = in vitro fertilization-embryo transfer, FTET = frozen-thawed embryo transfer, IVIG = intravenous immunoglobulin G, NK = natural killer.
![]()
Obstetric complications
Including all cases, 87.6% (n = 99) had no obstetric complications after IVIG and aspirin administration. Among the rest (12.4%, n = 14), preterm premature rupture of membranes (PPROM) was the most frequent (n = 5), followed by 3 cases of preterm labor (PTL), 2 of fetal death in utero, and 1 case of incompetent internal os of the cervix (IIOC). In addition, there were 3 cases of immediate complications after IVIG administration, 2 were nausea and 1 was general weakness (Table 3).
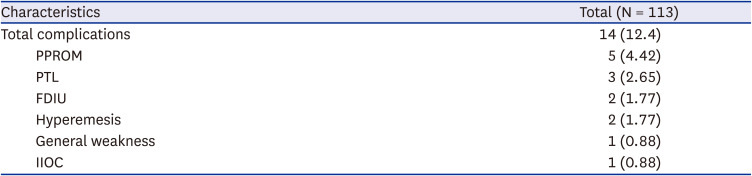
Table 3
Obstetric complications
| Characteristics | Total (N = 113) | |
|---|---|---|
| Total complications | 14 (12.4) | |
| PPROM | 5 (4.42) | |
| PTL | 3 (2.65) | |
| FDIU | 2 (1.77) | |
| Hyperemesis | 2 (1.77) | |
| General weakness | 1 (0.88) | |
| IIOC | 1 (0.88) | |
Values are presented as number (%).
PPROM = preterm premature rupture of membranes, PTL = preterm labor, FDIU = fetal death in utero, IIOC = incompetent internal os of the cervix.
![]()
Go to :
DISCUSSION
As IVIG has been used to treat various autoimmune and inflammatory diseases, it is no surprise that it has also begun to be used as an RPL treatment. Several clinical trials have been conducted since Carreras et al.22 reported the first successful treatment of IVIG in a patient with RPL in 1988. In the 1990s, studies reported an IVIG treatment efficacy of 62–74% in natural pregnancies,2324 similar to our results. Since then, the findings regarding IVIG treatment efficacy in IVF-ET or FTET have differed. Some studies reported no therapeutic effect, while others reported 80% live birth rates or higher.41225
Mechanism of aspirin is known to promote implantation by preventing thrombosis of maternal-placental interface due to its antiplatelet and anti-inflammatory effects.21 However, the therapeutic effect of low-dose aspirin was also controversial. Several meta-analyses found that low-dose aspirin was not associated with preventing pregnancy loss in URPL; however, treatment often includes empirical low-dose aspirin even in women without APS.2627 Most recent meta-analyses showed that low-dose aspirin may improve live birth rate for URPL, and a randomized trial suggested that preconception treatment with low-dose aspirin may improve reproductive outcomes in women who have had 1 or 2 pregnancy losses.2128 In our study, the total live birth rate was 73.5%, which was higher than the miscarriage rate, regardless of the method of pregnancy. Therefore, IVIG combined with low-dose aspirin treatment may effective for patients with URPL.
The subgroup analyses vary from study to study, and due to heterogeneity of study populations, opinions on the efficacy of IVIG in recent meta-analyses are conflicting.46293031 For example, Wang et al.29 concluded that IVIG may have potential benefits in the live birth rate in URPL, but evidence is insufficient (relative risk [RR], 1.25; 95% confidence interval [CI], 1.00–1.56; P = 0.05). However, subgroup analysis showed that the live birth rate marginally increased in secondary RPL (RR, 1.26; 95% CI, 0.99–1.60; P = 0.06), which is similar to that of the Egerup et al.’s study,32 and significantly increased in patients who received IVIG before conception (RR, 1.67; 95% CI, 1.3–2.14; P < 0.001). Similarly, Christiansen et el.4 found that IVIG has no therapeutic effect on live birth rate, but there may be some benefits when administered before conception. In another study, IVIG showed better reproductive outcomes in antibody positive patients compared to completely antibody negative, but the difference was not statistically significant.33 To summarize, most recent meta-analyses suggested that initiation of IVIG before conception, and treatment in women with abnormal immunity such as increased NK cell levels, could have a potentially beneficial effect on the live birth rate, although the evidence is still at level 2.31 In our study, the live birth rate was high regardless of type of RPL, timing of IVIG, and presence of autoantibodies. However, our study population had more patients with primary RPL, who were treated after conception. There are limitations to suggesting IVIG treatment for URPL due to the heterogeneity of study population and subgroup analysis. Therefore, more studies are needed to establish the efficacy and safety of IVIG treatment.
In our study, the term delivery rate was 86.7%, which was higher than that reported in another recent study,17 which seems to support the potential positive effects of IVIG on URPL. We administered a low IVIG-dose at a 2–3 weeks intervals with a dosage of 0.2 g/kg or 10 g (fixed dose). To date, there is no specific administration protocol for IVIG such as optimal dose, interval and initiation timing. Several studies included in the previous meta-analyses used an IVIG dosage of 0.4 g/kg every 2 to 3 weeks. However, the dose and administration method varied from 0.2–0.8 g/kg between months and weeks. The difference in the RR of miscarriage was not statistically significant when comparing low- and high-dose groups based on a total dosage of 84 g (P = 0.17).4293234 According to a study by Stricker et al.,15 which used a low dose of IVIG, 0.2 g/kg was administered within 2 weeks of pregnancy, followed by monthly dosing. The live birth rate was 75% up to 12 weeks of pregnancy and 95% up to 30 weeks of pregnancy. However, considering the half-life of IVIG, Saab et al.31 recommended that the interval of IVIG should not exceed 3 to 4 weeks. In our study, a low-dose of IVIG was administered every 2 weeks, leading to a high live birth rate in both the natural pregnancy and ART groups, so this protocol seems to be appropriate for patients with URPL.
In this study, most patients received IVIG more than once. There were only 14 cycles of single administration of IVIG, most of which had no side effects, but were discontinued due to miscarriage. Of the 6 cases in which pregnancy was maintained, only 2 cases were not treated with IVIG due to hyperemesis, and 1 patient was discontinued due to general weakness. However, the association between symptoms and IVIG was not clear. In the remaining 3 cases, the reason for interrupting IVIG treatment was not found in the medical records. In our study, there was no control group that did not receive IVIG, so patients who received IVIG only once and stopped taking IVIG for unavoidable reasons was set as a control group and compared with the multidose group. They showed a significantly higher live birth rate than patients who received IVIG only once. This result suggests that IVIG may increase the live birth rate of patients with URPL. However, the effect of IVIG treatment could not be determined because the patients were not compared to an untreated control group. In a recent study of women with RPL, the live birth rate with IVIG treatment was reported to be 86% compared to 42% for women without IVIG treatment.35 Several non-randomized studies also suggested that IVIG treatment may improve the pregnancy outcome.81236 In contrast, randomized controlled trials (RCTs) failed to prove the efficacy of IVIG treatment, and the live birth rate in the untreated group was similar to that in the IVIG treatment group (50% vs. 55%, P = 0.67).19 However, RCTs are very limited and there is heterogeneity between studies in which drugs of various settings, such as IV intralipid, anticoagulant and albumin, are administered to untreated controls.193738 Therefore, our study results suggest that IVIG treatment will be effective in URPL patients, but more studies are still needed due to the weakness of the design of the present study.
Although it has been reported that NK cell expansion is closely related to RPL, and IVIG treatment is generally known to help RPL by lowering NK cells, it is controversial whether NK cell measurements are appropriate predictors of birth rates. According to a meta-analysis by Tang et al.,39 the predictive value of NK cell counts for miscarriage, implantation failure, and miscarriage rates after ART is not significant. Therefore, more evidence is needed to determine whether IVIG treatment should be administered when NK cell fraction is at least 12% in patients with URPL. However, in Korea, it is not feasible to prescribe IVIG for the patients with URPL without NK cell expansion since October 2017, according to the regulation of Health Insurance Review & Assessment Service. Therefore, in the present study, we could recruit the data of the patients with URPL without NK cell expansion who had been treated with IVIG only before October 2017. The live birth rate was high both in the patients with and without NK cell expansion in this study. This finding suggests that IVIG treatment may increases the live birth rate in cases of URPL independent of the presence of NK cell expansion. In addition to reducing NK cell expansion, some of the known IVIG mechanisms act as immune modulators for balancing various cytokines, autoantibodies, and Th cells.8910 Lee et al.36 suggested that IVIG treatment for cellular immune abnormalities, including increased Th1/Th2 ratio without NK cell expansion, may improve pregnancy outcome. In another study, effect of IVIG on Th17 and regulatory T cells (Treg) in RPL has been investigated.35 IVIG treatment significantly downregulated Th17 cells and upregulated Treg cell. Moreover, mRNA expression levels of Th17/Treg cytokines, such as IL-17 and RORγt mRNA levels, were significantly decreased in IVIG treatment group compared to untreated group. Recently, extracellular vesicles (EVs) in plasma have been suggested as another mechanism for the therapeutic effect of IVIG for URPL.40 In this study, EVs were significantly increased in IVIG treatment group compared to placebo group (albumin treatment). However, the biological role of this phenomenon is unknown. These findings reviewed above indicate that IVIG treatment can lead to successful pregnancy outcome through various mechanisms, such as NK cell, T cell and other unknown cellular mechanism. Therefore, even in the absence of NK cell expansion, URPL can occur due to other immune abnormalities, so it is necessary to think about IVIG treatment based on only NK cells. However, since NK cell levels were assessed in only 62 patients in our study, and no untreated control group was included, these results should be interpreted cautiously. A further well-designed case-control study including untreated control groups is needed to clarify whether there may be any difference of effects of IVIG between those with and without NK cell expansion.
The use of IVIG combined with low-dose aspirin during pregnancy is empirically associated with few serious side effects for the mother and fetus, but different studies report slightly different results in this regard. According to Stricker et al.,15 PTL occurred in 8% of patients (2/24). The findings of that study are in line with our results in which PTL occurred in 2.65% of patients (3/113). However, 2 patients were delivered at approximately 36 weeks of pregnancy with healthy newborns. Moreover, there were 5 cases of PPROM, in our study, and 2 of them resulted in live births. In 1 case of IIOC, newborns were delivered at term during the second trimester of pregnancy after McDonald’s surgery. Finally, out of the 14 cases that presented with complications, 7 resulted in live births. Therefore, we concluded that IVIG and low-dose aspirin treatment had few negative effects. No other direct side effects related to IVIG were observed.
In summary, the present study is the first to analyze the results of IVIG treatment in natural and ART pregnancies and suggests that empirical treatment with IVIG and low-dose aspirin is effective even in patients without NK cell expansion. The high proportion of natural pregnancies in this study may be an important contribution to the diversity of study populations, considering that most studies focused on ART patients. In addition, a large set study analyzing 113 cycles with IVIG treatment can support the study of IVIG efficacy on RPL. Furthermore, the fact that all 113 cycles of pregnancy could be analyzed for obstetric complications can be a basis for proving the minimal side effects of IVIG and low-dose aspirin. However, this study has the following limitations: it was a retrospective study, not all the patients underwent overall immune tests, and we had no untreated control group. In addition, the fact that only data before 2017 were included in the case of using IVIG with less than 12% of NK cells may also increase the heterogeneity of the patient group. Lastly, we did not clarify whether the positive pregnancy outcome was due to low-dose aspirin or IVIG, because of the retrospective nature of the study. However, our data may provide a helpful information to patients who do not have an alternative treatment option for URPL, based on the favorable prognosis with the combined treatment. Although there was no adequate control group in this study, our IVIG combined with low-dose aspirin treatment results showed comparable live birth rates in other studies. RPL can occur due to several other immunological causes that are not yet known. For patients with URPL who have no other alternative treatment options, IVIG may be an opportunity. Even in the absence of NK cell expansion, IVIG treatment may be beneficial in improving pregnancy outcomes in URPL patients. Therefore, further well-designed case-control studies will be needed to identify cellular immune abnormalities in URPL and to determine the efficacy of IVIG treatment in appropriate patients.
Go to :
 XML Download
XML Download