

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Esophageal cancer is the 10th most common cancer worldwide and the 6th leading cause of cancer-related mortality.1 Histopathologically, esophageal cancer is mainly classified as squamous cell carcinoma (SCC) and adenocarcinoma. SCC constitutes > 90% of all esophageal cancer cases in East Asian countries, including Korea, Japan, and China and the overall 5-year survival rate remains 25–30%.23 However, patients with mucosal or submucosal cancer without lymph node metastasis have a > 80% survival rate.4 Therefore, many attempts have been made to ensure early detection and intervention to increase the curability of treatment, which prolongs the survival of patients with esophageal squamous cell carcinoma (ESCC). Currently, ESCC is diagnosed by examination of endoscopic forceps biopsy or resection specimens, but these approaches cannot be easily performed because of their invasiveness and high cost.56 These specimens do not represent the intra-tumoral heterogeneity and mechanisms of tumor progression and resistance to treatment.7 Although non-invasive tumor markers such as SCC antigen and carcinoembryonic antigen have been used for early detection and monitoring tumor dynamics of ESCC in clinical settings, they do not have sufficient sensitivity and specificity for early diagnosis and tumor progression.8 Therefore, the identification of novel and effective biomarkers for early detection and prediction of tumor progression is important to improve clinical outcomes for ESCC patients.
MicroRNAs (miRNAs) are small non-coding RNAs (18–25 nucleotides long) that can function as oncogenes or tumor suppressors by translational repression or degradation of the target mRNAs.9 miRNAs are stably detectable in plasma and serum,10 and tumor-derived miRNAs are resistant to endogenous ribonuclease activity because they are packaged by several secretory particles such as exosomes and apoptotic bodies in blood.1112 Accordingly, circulating miRNAs can be present in a stable form, and their expression level is reproducible and consistent among subjects.13 miRNAs contribute to carcinogenesis and could provide new therapeutic strategies such as biomarkers and therapeutic targets for cancer. Numerous studies have demonstrated the role of miRNAs in the tumorigenesis and progression of various cancers and the potential of non-invasive biomarkers for diagnosis or prognosis of cancers.1415 Several studies have reported the potential application of circulating miRNAs in ESCC1617; however, the results are inconsistent because of the differences in research methods and included populations among studies.
Therefore, in order to find miRNAs that can be generalized for use in clinical practice, we selected four miRNAs (miR-18b, miR-21, miR-31, and miR-375) from the published academic literature as candidate targets for the plasma miRNA assay.1819202122 We hypothesized that these plasma miRNAs would be identified as potentially useful biomarkers in ESCC patients. Therefore, we investigated whether a plasma miRNA assay would be useful for differentiating ESCC patients from healthy controls. We then determined whether the plasma miRNA levels were associated with the clinicopathological characteristics of ESCC patients.
METHODS
Patients
Between May 2016 and April 2021, 16 healthy volunteers and 66 patients histopathologically diagnosed with ESCC who had not been diagnosed with other past or current malignancies were enrolled in the study at Pusan National University Hospital (Busan, Korea). The patients’ medical history, physical examination, complete blood count and biochemistry tests, endoscopic ultrasonography, and imaging studies using chest and abdominal computed tomography (CT) and/or positron-emission tomography with CT for tumor staging were investigated. Staging was assessed according to the American Joint Committee on Cancer tumor-node-metastasis (TNM) staging for esophageal cancer (8th edition).23
Treatment modalities
Treatment was individualized according to the initial clinical TNM stage at the time of diagnosis. Five of the 66 patients underwent neoadjuvant chemotherapy and additional surgical resection, whereas 12, 14, 18, 15, and 2 patients underwent surgical resection, concurrent chemoradiation, palliative chemotherapy, endoscopic submucosal dissection (ESD), and conservative treatment, respectively. In appropriately selected superficial ESCC patients, ESD was performed under conscious sedation.24 In patients with resectable esophageal cancer that was unsuitable for ESD, the Ivor Lewis esophagogastrectomy or 3-hole minimally invasive esophagectomy was performed.24 In patients with locally advanced or metastatic cancer, neoadjuvant or palliative chemotherapy with 5-fluorouracil and cisplatin was administered. Some patients underwent concurrent chemoradiation comprising two cycles of combined 5-fluorouracil and cisplatin with 50 Gy of radiotherapy in the same period.
RNA extraction
After obtaining informed consent, 3 mL peripheral blood was collected from healthy controls and ESCC patients before initial treatment with surgery, ESD, chemotherapy, or chemoradiation. Cell-free plasma was separated from blood samples within 2 hours after collection using a one-spin protocol (800 ×g force for 10 minutes at 4°C) to prevent contamination by cellular nucleic acids. Plasma samples were stored at −80°C until miRNA analysis.
Total RNA was extracted from 400 µL plasma samples using the mirVana PARIS™ (Thermo Fisher Scientific, Waltham, MA, USA) according to the manufacturer’s protocol. Briefly, to isolate miRNA from the blood samples, an equal volume of 2× denaturing solution was added to 400 µL plasma at 16°C, and the mixture was incubated for 5 minutes on ice. Next, 650 µL acid-phenol was added, and the tube was vigorously agitated for 10 seconds. After centrifugation at 10,000 ×g for 10 minutes at 4°C, the supernatant was transferred to a new tube and 1.25 times of ethanol was added. Following incubation for 5 minutes at 16°C, for each sample, a filter cartridge was placed into one of the collection tubes, 600 µL of the mixture was added into the filter cartridge, and the sample was centrifuged at 10,000 ×g for 30 seconds at 4°C. Then, 600 µL of wash solution 1 was added to the filter cartridge and the sample was centrifuged at 10,000 ×g for 30 seconds at 4°C. Next, 500 µL of wash solution 2/3 was added and the sample was centrifuged at 10,000 ×g for 30 seconds at 4°C. Then, 500 µL of wash solution 2/3 was added and the sample was centrifuged at 10,000 ×g for 1 minute at 4°C. The filter cartridge was then transferred to a new collection tube. Finally, total miRNA was eluted into 50 µL elution solution according to the manufacturer’s protocol, and was stored at −80°C after centrifugation at 10,000 ×g for 1 minute.
Reverse transcription (RT)-quantitative polymerase chain reaction (qPCR) of miRNAs
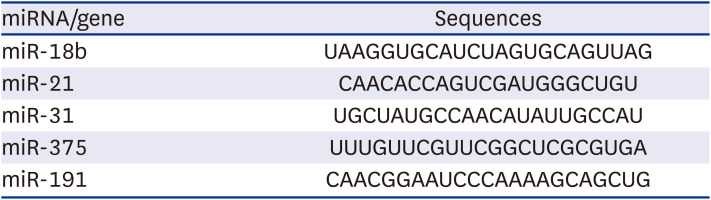
RT was conducted using a TaqMAN miRNA RT kit (Applied Biosystems, Foster City, CA, USA). The reaction system was 15 µL, containing 5 µL RNA extract, 1.5 µL 10× RT buffer, 0.2 µL RNase inhibitor (20 U/µL), 1 µL reverse transcriptase (50 U/µL), 0.15 µL 100 mM deoxyribonucleotide triphosphates, 3 µL specific miRNA primer (Table 1: miR-18b, miR-21, miR-31, miR-375, and miR-191), and 4.15 µL nuclease-free water. For the complementary DNA (cDNA) synthesis, the reaction mixtures were incubated at 16°C for 30 minutes, 42°C for 30 minutes, and 85°C for 5 minutes.
Table 1
MicroRNA sequences and internal reference
| miRNA/gene | Sequences |
|---|---|
| miR-18b | UAAGGUGCAUCUAGUGCAGUUAG |
| miR-21 | CAACACCAGUCGAUGGGCUGU |
| miR-31 | UGCUAUGCCAACAUAUUGCCAU |
| miR-375 | UUUGUUCGUUCGGCUCGCGUGA |
| miR-191 | CAACGGAAUCCCAAAAGCAGCUG |
Subsequently, RT-qPCR was performed using the RG-6000 Real Time PCR (Corbett Research, Sydney, Australia) with TaqMan® Universal PCR Master Mix II, no UNG (Thermo Fisher Scientific). The 20 µL reaction mixtures for the RT-qPCR contained 2 µL cDNA, 10 µL master mix, 1 µL assay primer, and 7 µL nuclease-free water. The reactions were incubated at 95°C for 10 minutes, followed by 40 cycles at 95°C for 15 seconds and 60°C for 1 min. The cycle threshold (Ct) values were calculated using Rotor-Gene 6000 series software 1.7 (Corbett Research). The expression levels of miRNAs from plasma samples were normalized to those of miR-191 and calculated using the equation 2−ΔΔCt.25 ΔCt was calculated by subtracting the average Ct value of the corresponding reference miRNA from that of the miRNA of interest.
Statistical analysis
Data are expressed as median, range or interquartile range (IQR). The Mann-Whitney test was used to compare the miRNA expression levels between ESCC patients and healthy controls. Receiver-operating characteristic (ROC) curves and the area under the curve (AUC) were used to further evaluate the levels of the four miRNAs to differentiate ESCC patients from healthy controls. The sensitivity, specificity, and positive and negative predictive values of the miRNAs for differentiating ESCC patients from healthy controls were expressed using 95% confidence intervals (CIs). Differences in the four miRNAs according to clinicopathologic characteristics were analyzed using the Mann-Whitney test or Kruskal-Wallis test. All statistical analyses were performed using IBM statistical package for the social sciences (SPSS) version 22.0, for Windows (IBM Co., Armonk, NY, USA). All P values were two-sided, and statistical significance was set at P < 0.05.
RESULTS
Baseline clinicopathologic characteristics of ESCC patients
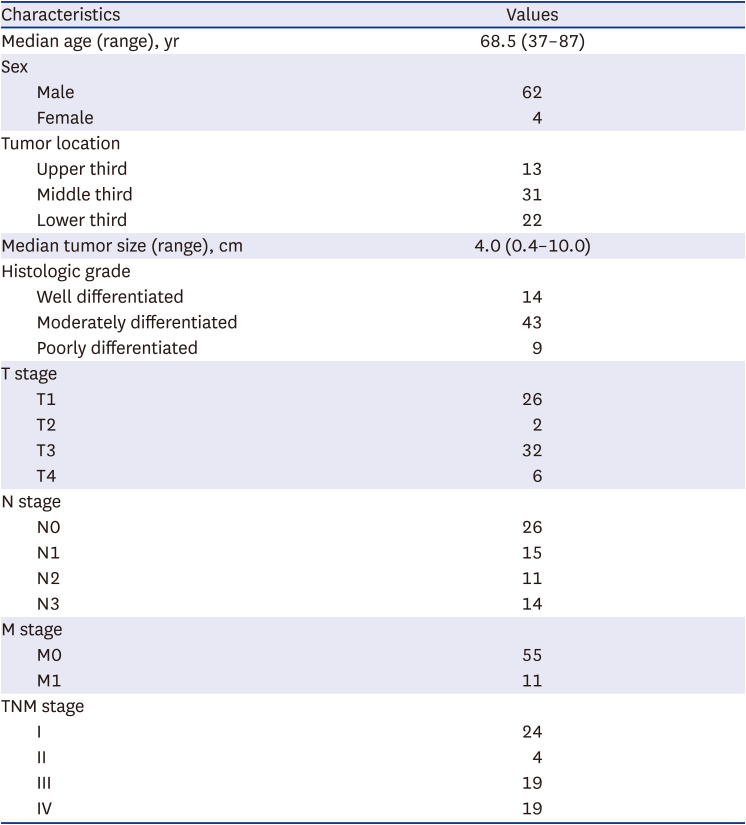
The clinicopathologic characteristics of the 66 ESCC patients including 62 men and 4 women with a median age of 68.5 (range, 37–87) years are summarized in Table 2. Thirteen tumors were located in the upper third of the esophagus, whereas 31 and 22 were in the middle and lower third, respectively. The median tumor size was 4.0 (range, 0.4–10.0) cm and histopathologically, 14, 43, and 9 tumors were well, moderately, and poorly differentiated, respectively. With regard to T and N stages, 26, 2, 32, and 6 tumors were T1, T2, T3, and T4, respectively and 26, 15, 11, and 14 tumors were N0, N1, N2, and N3, respectively. Distant metastases were observed in 11 patients. For TNM stage, 24, 4, 19, and 19 patients were diagnosed with stage I, II, III, and IV disease, respectively.
Table 2
Baseline clinicopathologic characteristics of 66 patients with esophageal cancer
Expression of four plasma miRNAs in ESCC patients
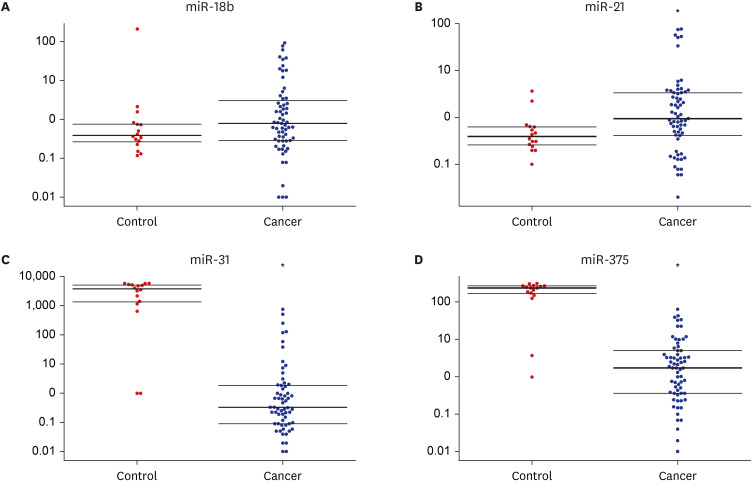
The expression level of plasma miR-21 was significantly higher in ESCC patients than in healthy controls (0.95 [IQR, 0.39–3.02] vs. 0.40 [IQR, 0.27–0.77], P = 0.022; Table 3, Fig. 1). In contrast, the expression levels of plasma miR-31 and miR-725 were significantly lower in ESCC patients than in healthy controls (0.30 [IQR, 0.09–1.88] vs. 3878.76 [IQR, 1,367.05–5,294.04], P < 0.001 and 1.73 [IQR, 0.39–5.06] vs. 240.14 [IQR, 170.20–264.05], P < 0.001, respectively). The expression level of plasma miR-18b was higher in ESCC patients than in healthy controls, but the difference was not statistically significant (0.79 [IQR, 0.29–3.02] vs. 0.39 [IQR, 0.27–0.77], P = 0.164).
Table 3
Expression levels of four plasma microRNAs between healthy controls and patients with esophageal cancer

Fig. 1
Expression levels of four plasma microRNAs in 16 healthy controls and 66 patients with esophageal cancer. (A) miR-18b. (B) miR-21. (C) miR-31. (D) miR-375.
Horizontal line: median with interquartile range.
*P value < 0.05.
The ROC curves were analyzed to determine whether the plasma miRNAs could be used as potential diagnostic biomarkers for differentiating ESCC patients from healthy controls (Fig. 2). The AUCs were 0.613 (95% CI, 0.497–0.721) for miR-18b, 0.687 (95% CI, 0.572–0.786) for miR-21, 0.876 (95% CI, 0.781–0.940) for miR-31, and 0.920 (95% CI, 0.838–0.968) for miR-375. At the cut-off values of 0.83, 0.69, 508.46, and 63.12, the sensitivities and specificities in the diagnosis of ESCC were 81.3% and 47.6% for miR-18b, 87.5% and 61.9% for miR-21, 87.5% and 98.4% for miR-31, and 87.5% and 100% for miR-375, respectively (Table 4).
Fig. 2
Receiver-operating characteristic curve analyses of four plasma microRNAs to discriminate patients with esophageal cancer from healthy controls. (A) miR-18b. (B) miR-21. (C) miR-31. (D) miR-375.
AUC = area under the curve.
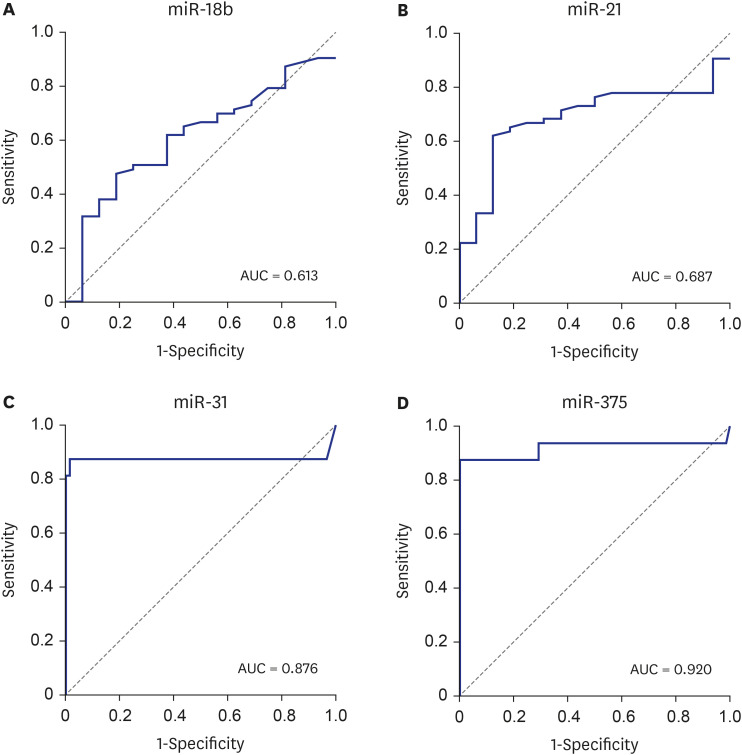
Table 4
Sensitivity, specificity, and positive and negative predictive values of four plasma microRNAs for differentiation of patients with esophageal cancer from healthy controls

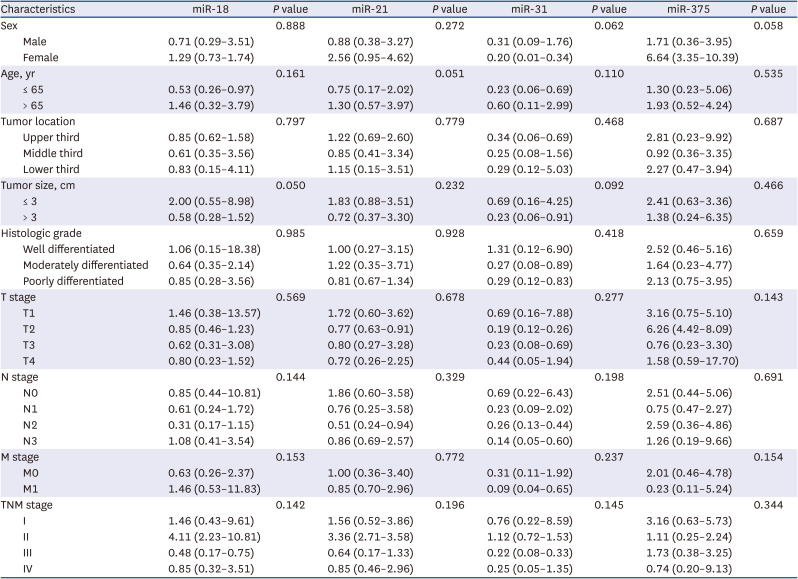
Table 5 summarizes the expression levels of the four plasma miRNAs according to the clinicopathologic characteristics of the 66 ESCC patients. There was no difference in the expression levels of the four miRNAs according to sex, age, tumor location, histologic grade, and TNM stage, except for the lower expression level of miR-18b in patients with a large tumor (> 3 cm) than in those with a small tumor (≤ 3 cm).
Table 5
Expression levels of the four plasma microRNAs according to clinicopathologic characteristics of 66 patients with esophageal cancer
DISCUSSION
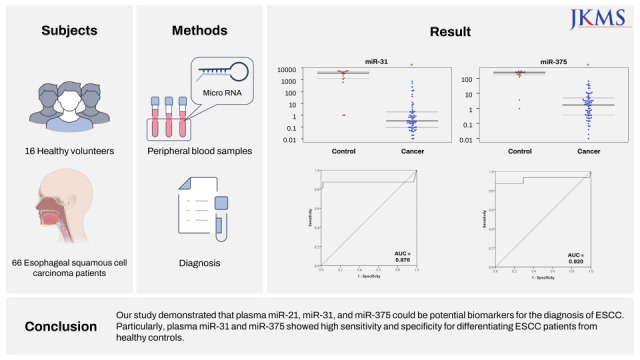
The reported expression profiles of various circulating miRNAs in ESCC are inconsistent.181920212226 In the present study, we selected four miRNAs and investigated their expression levels in the plasma of ESCC patients based on previously published literature. We found that plasma miR-21, miR-31, and miR-375 could be potential biomarkers for ESCC diagnosis. Particularly, miR-31 and miR-375 showed high sensitivity and specificity for differentiating ESCC patients from healthy controls.
Presently, endoscopy with forceps biopsy remains a standard modality for diagnosing ESCC, but it has several limitations such as invasiveness, the possibility of missing small lesions, and sampling error. Although the use of advanced diagnostic technologies such as narrow-band imaging can increase the detection rate of ESCC, population-based screening is ineffective because of the relatively low incidence of ESCC. Thus, endoscopic screening for ESCC is limited to individuals who are at a high risk. Considering the low invasiveness of blood sampling, circulating miRNAs could be ideal biomarker candidates.
Although the exact sources of circulating miRNAs are unknown, mature miRNAs are packed into exosomes in cells and then released into the blood through extracellular secretion.27 Therefore, circulating miRNAs can reflect the expression of miRNAs in tumor tissues to a certain degree. The expression patterns of circulating miRNAs are consistent with those of tumor tissue miRNAs in ESCC.2128 Considering that blood samples are more convenient to collect and blood miRNAs are stably detected at reproducible expression levels, circulating miRNAs can be optimal tumor biomarkers.29
miR-18b belongs to the miR-106a-363 cluster located on chromosome X, which encodes six miRNAs (miR-106a, miR-18b, miR-20b, miR-19b-2, miR-92-2, and miR-363). Because miR-18b is highly expressed in various tumors, especially in advanced gastric and colorectal cancers, it is mostly regarded as an oncogenic miRNA via participation in the regulation of the cell cycle, proliferation, and migration.30313233 Owing to the paucity of available data on the expression of miR-18b in ESCC, we also analyzed this marker in the present study. The lack of a significant difference in the expression levels of plasma miR-18b between ESCC patients and healthy controls and the absence of a correlation between its expression levels and most clinicopathologic characteristics, except for tumor size, suggests it might not be an efficient candidate biomarker for ESCC.
miR-21, a well-known onco-miRNA, is linked to tumor aggression and carcinogenesis, in part, by preventing apoptosis,34 and is overexpressed in various gastrointestinal cancers.35 In the present study, plasma miR-21 expression was significantly upregulated in ESCC patients compared with healthy controls, which is consistent with the results of previous studies.363738 Although some previous studies have reported that higher blood miR-21 was associated with metastasis,38 the plasma miR-21 level had no relationship with sex, age, tumor location, TNM stage, and other clinicopathologic characteristics in the present study, similar to other existing reports.3639 A recent meta-analysis showed that ESCC patients with high circulating miR-21 levels had significantly shorter overall survival than those with low levels did.18
The importance of miR-31 in cancers has been suggested; however, its potential roles as a tumor suppressor or oncogenic factor remain controversial. miR-31 is reported to be upregulated in head and neck, lung, and colorectal cancers,404142 but downregulated in gastric, breast, prostate, and ovarian cancers.43444546 A study investigating miR-31 in ESCC tissues and sera reported that ESCC patients had a higher expression of miR-31 in serum compared with healthy controls and the level of serum miR-31 was elevated with an increase in the grade of TNM stage, consistent with the results observed in the tissue samples.47 However, in the present study, the expression level of plasma miR-31 in ESCC patients was significantly lower than that in healthy controls, and the miR-31 level was not associated with TNM stage and other clinicopathologic characteristics. These inconsistent results of miR-31 might be due to the difference in baseline demographics (sex ratio, age distribution, and TNM stage) of the included patients. Moreover, the functional mechanisms of miRNAs in tumors are extremely complex where one miRNA can regulate several target genes and several miRNAs can regulate one target gene. This complex relationship could lead to varying expression levels of oncogenes and tumor suppressor genes in target genes. Therefore, comprehensive studies on the role of miR-31 in ESCC are needed to establish its potential has oncogenic or tumor suppressor role.
miR-375 was first identified in the murine pancreatic MIN 6 β-cell line, and several studies have shown that it functions as a tumor suppressor gene in various cancers.484950 miR-375 has also been reported to play a tumor suppressive role in ESCC by inhibiting cell proliferation, colony formation, and metastasis in vitro and in vivo.51 In the present study, the significantly lower expression levels of plasma miR-375 in ESCC patients than in healthy controls were consistent with the results of previous studies, which also showed a similar miR-375 expression tendency in plasma and primary ESCC tissue samples in most cases.2136 Similarly to our results, there was no significant correlation between the level of plasma miR-375 and clinicopathologic characteristics in these studies.2136 A recent meta-analysis demonstrated that the downregulation of miR-375 was significantly correlated with poor overall survival in patients with head and neck cancer or ESCC.22
Our study has some notable limitations that should be addressed in future studies. First, because we focused on the level of plasma miRNAs at the time of diagnosis, we did not collect long-term follow-up data, such as therapeutic response and survival. Second, the number of cases included in the present study was relatively small, as this was a single institution-based study. Therefore, a larger sample size is required to validate the role of miRNAs as biomarkers for ESCC, as shown in the present study. Third, profiles of circulating miRNAs could differ according to the specimens analyzed, such as plasma versus serum, and the RT-qPCR test methods (TaqMAN probe method versus SYBR green method). Some meta-analyses have suggested that plasma-based specimens have a higher accuracy than serum-based specimens,5253 whereas others showed the opposite tendency.5455 Generally, the TaqMAN probe method might have a higher specificity than the SYBR green method, which may, in turn, have a higher sensitivity than the TaqMAN probe method. A recent meta-analysis of miRNAs in ESCC showed that both plasma and serum could be recommended as clinical specimens and there was no statistically significant difference between miRNA detection methods.16 Finally, miRNAs detected in patients with ESCC are not organ-specific. Even though we excluded concurrent malignancies via endoscopy, laboratory tests, and imaging studies using chest and abdominal CT and/or positron-emission tomography with CT, there is still a possibility that undetected malignancies present in other organs were a source of plasma miRNAs.56 Therefore, plasma miRNAs cannot substitute endoscopy with forceps biopsy for ESCC diagnosis. However, they may be a good diagnostic method in population with a high risk of ESCC. Nevertheless, our results regarding plasma miRNAs should be validated in other studies prior to clinical application.
In conclusion, we identified a higher expression of plasma miR-21 and lower expression of plasma miR-31 and miR-375 in ESCC patients than in healthy controls. The validation of these findings in a large-scale case-control study could lead to these plasma miRNAs serving as potential non-invasive biomarkers for the detection of ESCC. The additional role of these miRNAs as predictive biomarkers for prognosis and response to chemotherapy should be explored in large, prospective, long-term follow-up studies.
 XML Download
XML Download