

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pityriasis rosea (PR) is a common, self-limiting papulosquamous disease that typically begins with a herald patch followed by the distinctive ‘Christmas tree’ like secondary eruptions on the trunk and proximal extremities.123 The etiology of PR is generally unknown but viral reactivation has been known as one of the etiologic factors.12
The coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) rapidly spread from February 2020 in South Korea.456 This devastating pandemic has changed almost all aspects of an individual’s everyday life, including mandatory social distancing, face mask use, and frequent hand washing or disinfection.57 The drastic and stronger changes in these personal preventive measures may cause significant alterations in the clinicopathological aspects of several non-COVID-19 infectious diseases with viral etiologies.89101112
PR or PR-like eruptions are one of the consistently reported cutaneous manifestations associated with the COVID-19 pandemic131415 and COVID-19 vaccination,16171819 which has been assumed to be associated with viral reactivation,1320 or alteration in the host immune response to the SARS-CoV-2 and the COVID-19 vaccination.17 In addition, the clinical characteristics and histopathologic findings of PR in the COVID-19 pandemic demonstrated coherent atypical histologic impressions compared with the patterns before the outbreak in our outpatient clinics. Therefore, this study aimed to verify the possible differences in the clinicopathological characteristics of PR before and during the COVID-19 pandemic.
METHODS
Participants
This retrospective review was performed on patients diagnosed with PR based on the clinical manifestations and skin biopsies collected between February 2018 and October 2019 and February 2020 and October 2021 at Korea University Medical Center (KUMC), Anam Hospital. The clinical photo of initially screened patients with PR were independently reviewed under the clinical diagnostic criteria which required essential features including discrete mostly scaly circular lesions with a peripheral collarette of scale with central clearance on at least two lesions.1 The exclusion criteria included multiple small vesicles at the center, localized manifestation mostly confined on hands and feet, evidence of secondary syphilis, and clinicopathological confirmation of other papulosquamous diseases including psoriasis, pityriasis lichenoides chronica.12 The equivalent months were designed to exclude seasonal effects on PR. The comparative analysis about total numbers and related features of the patients with PR was performed before and after February 2020, which was a flag-marked timing of the COVID-19 outbreak in South Korea.
Clinical characteristics of PR
The clinical characteristics required for the classification of PR were documented and analyzed from the hospital medical information system, patient files, and clinical photos. The classic and atypical forms of PR are clinically categorized by the shape and distribution of the secondary eruptions, disease duration, and associated symptoms.123 The typical morphological patterns include macular and papular lesions, and atypical patterns include erythema multiforme (EM)-like, urticarial, vesicular, purpuric, and other forms of eruptions. The classic anatomical distribution is on the trunk and extremities, whereas the atypical sites are the face, intertriginous area including the axilla and groin region, hands, and feet. PR usually lasts approximately 6 weeks; occasionally, PR can last > 12 weeks.123 The assessment grades for combined itching sensation were 0, 1, and 2 for absent, mild to moderate, and severe pruritus, respectively. The possibly related histories of medical illness, medication, and vaccination, including COVID-19 infection and vaccination during the pandemic, were investigated based on the patient medical records.
Histopathological classification of PR
The histopathological findings shared the common features of PR were additionally categorized into three distinct patterns: brisk and dense infiltration, dormant and sparse infiltration, and psoriasiform based on randomized and blinded slide reviews by the three board-certified dermatologists at KUMC. The brisk and dense dermal perivascular lymphocytic infiltration was one of the classical histopathologic patterns of PR. The degree of dermal perivascular lymphocytic infiltration was semi-quantitatively assessed into 0, 1, 2, and 3 for absent, mild, moderate, and severe, respectively. The absent to mild degree and moderate to severe degree of infiltration were classified into dormant and sparse and brisk and dense infiltration patterns, respectively. The psoriasiform pattern designated prominent features of irregular acanthosis without significant interface change.
Statistical analysis
Chi-squared test or Fisher’s exact test and Mann-Whitney test were used to verify the possible periodic association of the clinicopathological characteristics before and during the COVID-19 pandemic using the IBM SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA). Means ± standard deviation and percentages were used for the descriptive statistics. The and a P value of < 0.05 was considered statistically significant.
RESULTS
Patients
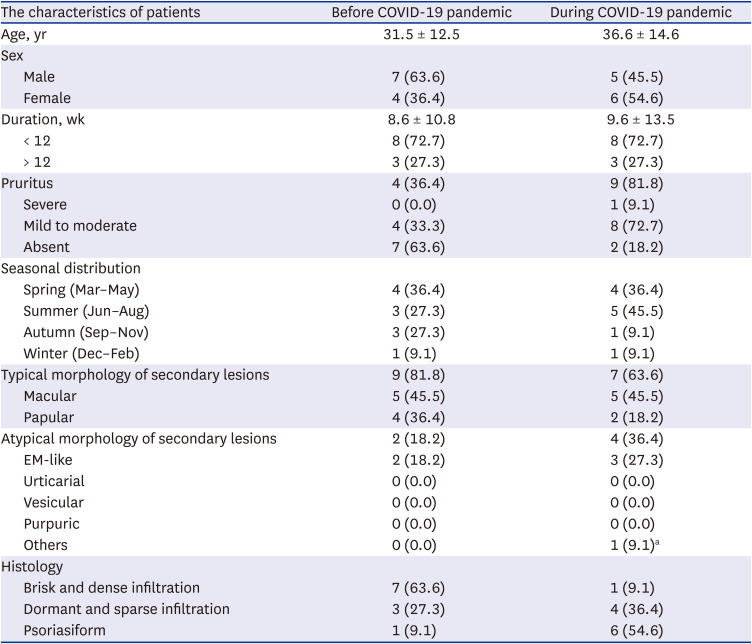
Eleven clinicopathologically diagnosed patients with PR were included between February 2018 and October 2019. Their mean age was 31.45 ± 12.51 years, with a slight male predominance (63.64%). The mean disease duration was 8.55 ± 10.80 weeks. An atypical duration of > 12 weeks was observed in 27.27% of patients. Those who complained of mild to moderate pruritus comprised 36.36%, whereas 63.64% reported no associated sensory symptoms. Eleven patients confirmed as PR were selected for the group between February 2020 and October 2021, and their mean age was 36.55 ± 14.58 years, with a slight female predominance (54.55%). The mean disease duration was 9.64 ± 13.52 weeks. Increased duration of > 12 weeks was observed in 27.27% of the patients. A relatively increased number of patients demonstrated concomitant itching sensation (81.82%), and most of them complained of mild to moderate pruritus (72.73%) except for one (9.09%) severe pruritus case. The grade of concomitant pruritus during the pandemic showed a significant increase compared with the result obtained from the period before the outbreak (P = 0.027). The seasonal predominance of PR, especially in the cold winter season from December to February, was not observed in either period before or during the COVID-19 pandemic (both seasonal distributions in winter, 9.09%) (Table 1). A total of three cases were related to the COVID-19 vaccinations. One subject was associated with the Oxford-AstraZeneca (AZD1222), and the other two patients were related to the Pfizer-BioNTech (BNT162b2) vaccinations.
Table 1
Clinical and histopathological features of patients with pityriasis rosea before and during the COVID-19 pandemic
Clinical characteristics; classic and atypical PR
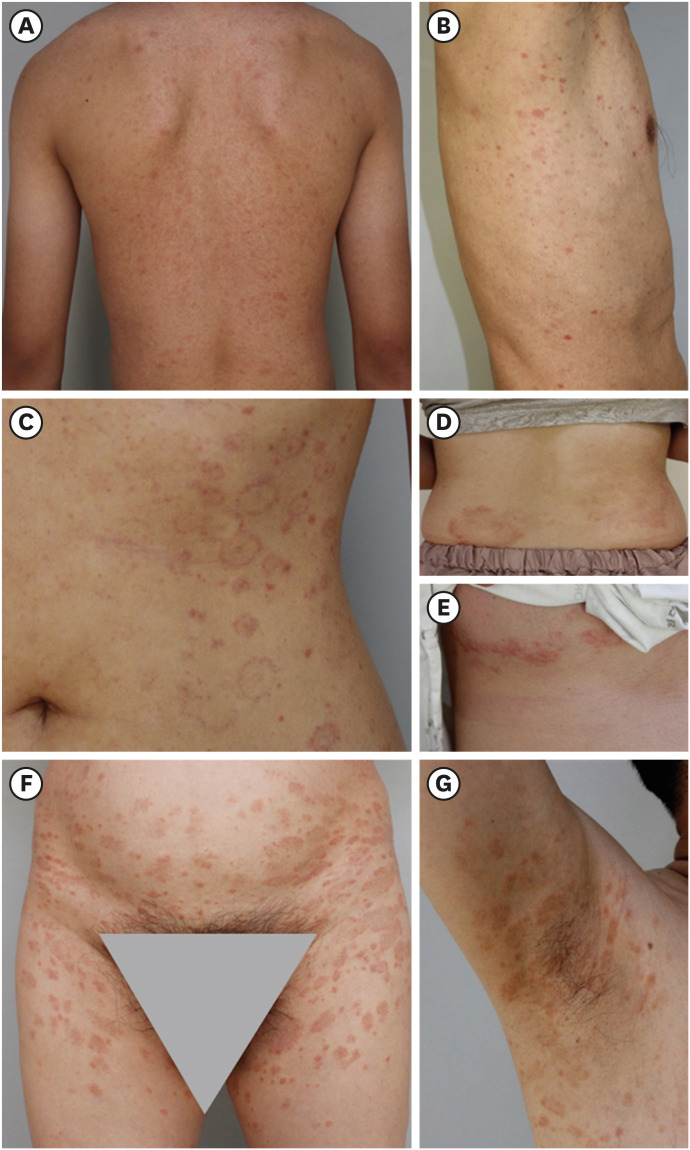
The typical macular or papular secondary eruptions of classic PR (Fig. 1A and B) comprised 81.8% and 63.6% of cases before and during the COVID-19 pandemic, respectively. The atypical morphological patterns were 18.2% and 36.4% before and during the COVID-19 pandemic, respectively. The atypical patterns included EM-like eruptions (Fig. 1C), and PR gigantea of Darier (Fig. 1D, Table 1). The atypical distribution increased from 18.2% to 45.5% of patients from before to during the COVID-19 pandemic, respectively. The documented unusual distribution included the inframammary region (Fig. 1E) and intertriginous areas such as the groin and axillae (Fig. 1F and G). Statistical significance was not observed in either morphological pattern or distribution of secondary eruption before and during the COVID-19 pandemic (P > 0.05).
Fig. 1
The morphological or regional patterns of secondary eruption observed in (A, B) typical and (C-G) atypical PR. (A) Macular and (B) papular types are commonly observed in the truncal region of patients with typical PR. The secondary lesions can also be atypically presented morphologically as (C) erythema multiforme-like eruption and (D) PR gigantea of Darier. The atypical distribution of secondary eruptions includes the (E) inframammary, (F) inguinal, and (G) axillary regions.
PR = pityriasis rosea.
Histopathological characteristics
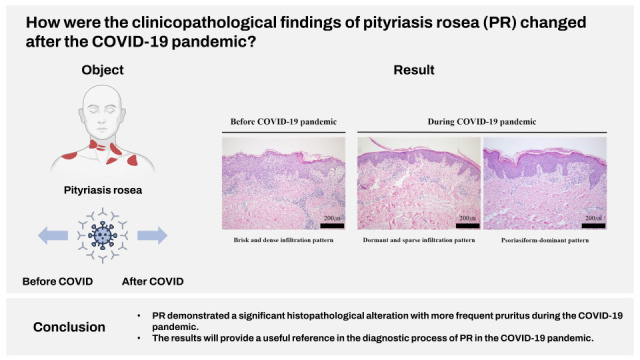
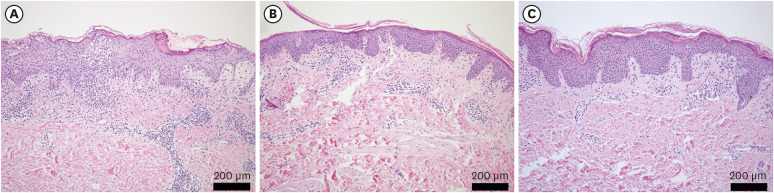
The histopathological results of patients with PR generally shared the features of mild to moderate acanthosis, mostly focal but occasionally confluent parakeratosis and dermal perivascular lymphocytic infiltration with few eosinophils. Among the three distinct histopathological categories, brisk and dense infiltration patterns demonstrated more acute inflammatory consequences, including serum crust, spongiosis, Langerhans cell abscess, papillary edema, and comparably heavy dermal lymphocytic infiltration with numerous eosinophils (Fig. 2A). Dormant and sparse infiltration demonstrated relatively less epidermal alteration and dermal lymphocytic infiltration (Fig. 2B) compared to the former category. The psoriasiform pattern demonstrated irregular acanthosis, and mounds of parakeratosis (Fig. 2C). The COVID-19 outbreak caused a statistically significant alteration in the histopathological patterns of PR (P = 0.019). Psoriasiform and dormant and sparse infiltration patterns comprised the majority of cases after the COVID-19 outbreak compared to the classic brisk and dense infiltration pattern-dominant results before the pandemic (Table 1).
DISCUSSION
The etiology of PR has been suggested to be associated with viral reactivation12132021 possibly related to SARS-CoV-2 infection131415 or COVID-19 vaccination.16171819 The atypical clinical patterns have been documented related to the case of PR diagnosed after COVID-19 infection or vaccination.22 The atypical presentations of PR include more unusual forms of secondary skin lesions, distributions, prolonged duration, and dominant sensory symptoms.222 The atypical presentation and distributions of the secondary eruptions in our study include EM-like eruptions (Fig. 1C), PR gigantea of Darier with particularly large lesions (Fig. 1D), and pityriasis marginata et circinata of Vidal, which are primarily confined to the axillae or inguinal region (Fig. 1F and G). Both cases of PR gigantea of Darier and pityriasis marginata et circinata of Vidal were documented during the COVID-19 pandemic, and the former case was related to the COVID-19 vaccination. Pruritus was absent in 25%, mild to moderate in 50%, and severe in 25% of patients with PR.12 Our results showed that significantly increased proportions of patients demonstrated mild to moderate or even severe pruritus after the COVID-19 outbreak. Interestingly, two out of three cases related to the COVID-19 vaccination complained of mild to moderate pruritus. One previously reported case with PR-like eruptions after mRNA vaccination presented with extreme pruritus.23
The representative histopathological features of PR include parakeratosis, spongiosis, and acanthosis in the epidermis, and extravasated red blood cells along with perivascular infiltration of lymphocytes, monocytes, and eosinophils in the dermis.12 All patients in our study shared common histopathologic features of PR. However, additionally classified histopathologic forms revealed a meaningful shift from a brisk and dense infiltration dominant pattern (Fig. 2A) to dormant and sparse infiltration (Fig. 2B) and psoriasiform (Fig. 2C) patterns during the COVID-19 outbreak in South Korea (P = 0.019). In addition, all three patients with PR related to the COVID-19 vaccination in our study presented dormant and sparse infiltration patterns, unlike the previously documented single case of PR-like eruption with drug reaction-like histologic features, including interface dermatitis and necrotic keratinocytes.18 The other reported case of PR-like eruption related to the COVID-19 vaccination demonstrated mild acanthosis, epidermal spongiosis,1924 and mounds of parakeratosis24 rather than interface change that were shared histopathologic findings in the psoriasiform pattern (Fig. 2C). In our study, 54.55% of patients with PR who were not associated with COVID-19 vaccination demonstrated a psoriasiform pattern. We initially assumed that the disease duration would be related to a shift in the histopathologic difference; however, it did not demonstrate any statistical difference before and during the COVID-19 pandemic (P > 0.05). Moreover, the disease duration, which could affect the degree of inflammatory cell infiltration, showed no statistically significant difference among the three histopathological classifications, especially between brisk and dense and dormant and sparse infiltration patterns (P > 0.05). The other clinical characteristics, including age, morphology, distribution, and pruritus, revealed statistically insignificant discrimination according to the histologic categories (P > 0.05).
Histopathologic features of drug eruption including interface dermatitis, dyskeratotic keratinocytes, and eosinophils are reported to be associated with PR-like eruptions after using barbiturate, captopril, clonidine, metronidazole, D-penicillamine, isotretinoin, levamisole, non-steroidal anti-inflammatory agents, omeprazole, terbinafine, hydroxychloroquine, tyrosine kinase inhibitor- imatinib, and tumor necrosis factor inhibitor- adalimumab.122526 In addition, PR-like rashes can be induced after the administration of diphtheria, smallpox, pneumococcal, hepatitis B virus, BCG, human papillomavirus, and COVID-19 vaccines.218252627 Vaccination-induced immune stimulation may cause chained viral reactivation or cell-mediated reactions associated with a molecule similar to a viral epitope.2527 The immunomodulatory effect of SARS-CoV-2 infection or COVID-19 vaccination during the COVID-19 pandemic was inferred to cause an increase in the prevalence of PR as reported in the literature.13 Our results also showed a slight increase in the prevalence of PR from 0.37% to 0.49% before and during the COVID-19 pandemic, respectively. ‘New normal’ lifestyle in COVID-19 pandemic, including social distancing, face mask use, and frequent hand washing,57 could also contribute to the alterations in the clinicopathological spectrum of PR by adjusting the etiologic proportions of opportunistic viral upper respiratory infection.89 However, further large-scale studies are required to confirm the true underlying causes of alterations. The limitations of the study were the small number of subjects for the confirmative statistical comparison and the lack of complete data about COVID-19 infection and/or vaccination history during the COVID-19 pandemic period due to the characteristics of the retrospective study proceeded based on documented medical records.
In conclusion, our comparative results demonstrated that the histopathological features of PR were meaningfully changed from the classic brisk and dense infiltration pattern before the COVID-19 outbreak to dormant and sparse and psoriasiform patterns during the COVID-19 pandemic. The more frequent concurrent pruritus could be an additional change in PR during the pandemic period.
 XML Download
XML Download