

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) is known to be a cause of chronic liver disease, and its prevalence is 20%–30% in the total population [1]. The prevalence of 20%–30% is mainly in Western countries, but the prevalence in Asian countries is increasing too, due to westernized lifestyles [234]. There are some discrepancies in the prevalence of NAFLD in the general Korean population. In 4,967 young healthy Koreans who participated in a health screening program, the age-adjusted NAFLD prevalence rates were 21.6% (male), 11.2% (female), and 16.1% (total) [5]. Another cross-sectional study included 140,000 participants in a health screening program, and the prevalence of NAFLD was 25.2%, with some differences based on where the participants lived [6].
The prevalence of NAFLD is related to the rising obesity rates. The prevalence of NAFLD in the general population is around 25%, but it escalates to more than 90% in highly obese persons undergoing weight-loss procedures [7]. Furthermore, NAFLD, like obesity, has varied features among ethnic groups and between countries [8].
Weight reduction has been proven in several studies to be the most effective therapy for NAFLD [910]. For patients with morbid obesity, bariatric surgery is now recognized as the only therapeutic option that achieves persistent and effective long-term weight reduction and improvement of associated comorbidities. Furthermore, it contributes to significant improvements in health-related quality of life [1112].
In Korea, there are few studies on the effects of NAFLD treatment after such weight-loss procedures. The purpose of this study was to examine the therapeutic role of bariatric surgery on NAFLD using quantified transient elastography (TE) and laboratory-based panels in morbidly obese patients in Korea.
METHODS
This study was approved by the Institutional Review Board of Kosin University Gospel Hospital (No. 2021-11-028). It was performed in accordance with the Declaration of Helsinki and written informed consent was obtained from all the patients.
A study was conducted on patients with NAFLD among patients who underwent metabolic surgery between 2019 and 2020. Only patients who underwent TE preoperatively and 6 months postoperatively were analyzed. Patients with alcoholic, autoimmune, or viral liver diseases were excluded. Notably, only Korean patients were included.
Bariatric surgery was performed according to the Korean insurance standards. Patients with a body mass index (BMI) of 30 kg/m2 or higher and those with complications were included. NAFLD is a general term that encompasses the spectrum of liver diseases, including nonalcoholic fatty liver, nonalcoholic steatohepatitis (NASH), and NASH cirrhosis. In this study, TE and serum panel were used to apply whether patients conform to NAFLD diagnosis. The patients underwent laparoscopic sleeve gastrectomy (LSG) or laparoscopic Roux-en-Y gastric bypass (RYGB) after a multidisciplinary team consultation. Preoperative and postoperative body weight and laboratory parameters were measured, and the results were analyzed at 6 months postoperatively.
Transient elastography
Liver stiffness (LS) and hepatic steatosis were measured using a FibroScan (Echosens, Paris, France) according to the manufacturer’s instructions before bariatric surgery and within 6 months after surgery. All examinations were performed after overnight fasting by experienced examiners (>100 examinations). TE was performed on the right lobe of the liver in the intercostal position according to established protocols using an XL probe. LS was expressed in kilopascals (kPa), and hepatic steatosis was expressed as a controlled attenuation parameter (CAP). CAP is a feature of TE that can quantify the degree of fat deposition in the liver parenchyma by measuring ultrasound attenuation [13]. According to a recent Korean study enrolling people who received regular health checkups, the normal CAP cutoff is 276 dB/m [14]. To obtain reliable results, at least 12 valid measurements were required, with a success rate greater than 60% and an interquartile range <30%.
Assessment of hepatic steatosis and liver fibrosis
The hepatic steatosis index (HSI) was proposed by Lee et al. [15] in a Korean cohort study of 10,724 subjects (5,462 with ultrasonography-defined NAFLD). The HSI was calculated based on sex, BMI, AST, ALT, and type 2 diabetes mellitus (T2DM). If the HSI was less than 30, NAFLD was excluded (negative likelihood ratio of 0.2, sensitivity of 93.1%), and if it was more than 36, NAFLD was diagnosed with high predictive accuracy (positive likelihood ratio of 6.1, specificity of 92.4%). The area under the receiver operating characteristic curve (AUC) of the HSI was 0.81. HSI showed acceptable accuracy in the Korean population [16].
Several serum marker scores were assessed, such as the De Ritis ratio (AST:ALT ratio) [17] and the AST to platelet ratio index (APRI), to determine NAFLD activity or fibrosis [18]. A normal AST:ALT ratio should be <1. In patients with alcoholic liver disease, the AST:ALT ratio is >1 in 92% of patients, and >2 in 70%. AST:ALT scores of >2 are, therefore, strongly suggestive of alcoholic liver disease, and scores of <1 are more suggestive of NAFLD [19]. APRI values of ≤0.3 and ≤0.5 rule out significant fibrosis and cirrhosis, and a value of ≥1.5 rules in significant fibrosis [20]. The fibrosis-4 index (FIB-4) was calculated using platelet count, age, AST, and ALT levels. The AUC of FIB-4 for advanced liver fibrosis was 0.765. When the FIB-4 score was less than 1.30, advanced liver fibrosis was excluded (accuracy, 90%), and when the FIB-4 score was more than 2.67, advanced liver fibrosis was diagnosed (accuracy, 80%) [21].
Statistical analysis
Data are expressed as numbers (percentages) or mean ± standard deviation. A chi-square test was performed to compare the clinical characteristics. Comparison of the changes in the parameters was made between different time points using the Wilcoxon signed-rank test. Comparison of the number of NAFLD patients using paired t-test. IBM SPSS Statistics ver. 25.0 (IBM Corp., Armonk, NY, USA) was used. Statistical significance was set at a P-value of <0.05.
RESULTS
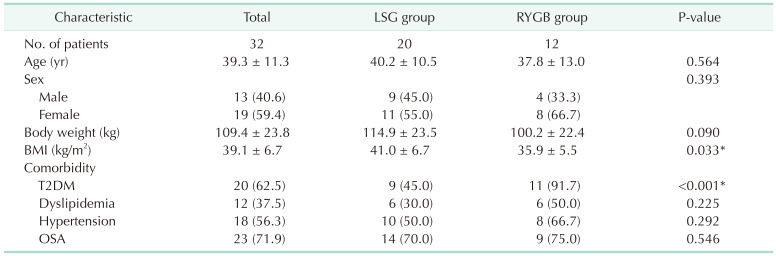
A total of 32 patients were enrolled, with a mean age of 39.3 ± 11.3 years. They were divided into the LSG (20 people) and the RYGB (12 people) groups. The LSG group had a higher BMI than the RYGB group (41.0 ± 6.7 vs. 35.9 ± 5.5, P = 0.033). As for comorbidities, the RYGB group had more T2DM patients (45% vs. 91.7%, P < 0.001) (Table 1).
Changes in hepatic steatosis and liver fibrosis
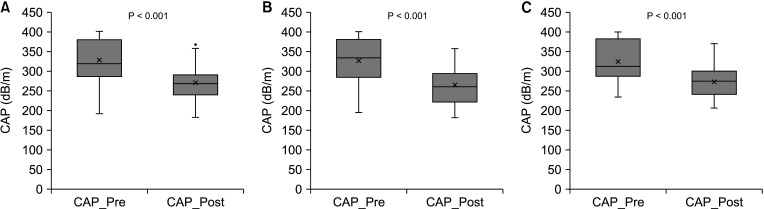
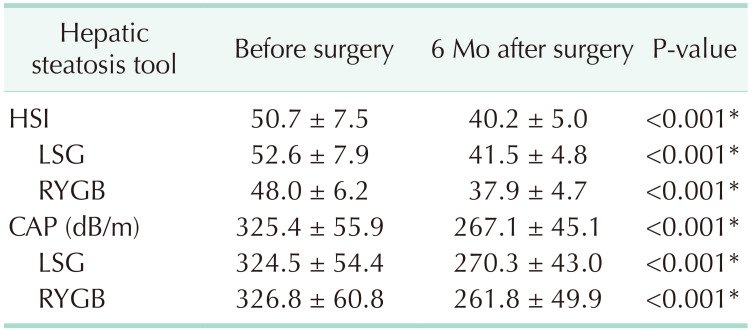
Table 2 shows the changes in hepatic steatosis. In all patients, there was a significant decrease in the HSI (P < 0.001). Significant changes were also observed in the LSG and RYGB groups after 6 months (P < 0.001). In addition, the results of the CAP were the same as those of the HSI. The change in the CAP is shown in Fig. 1.
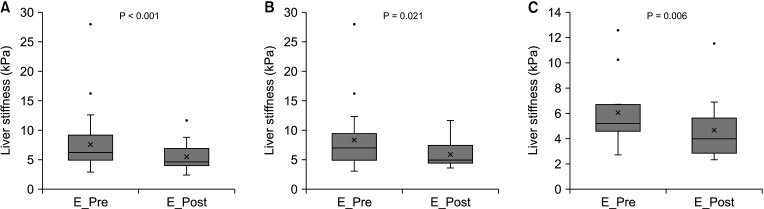
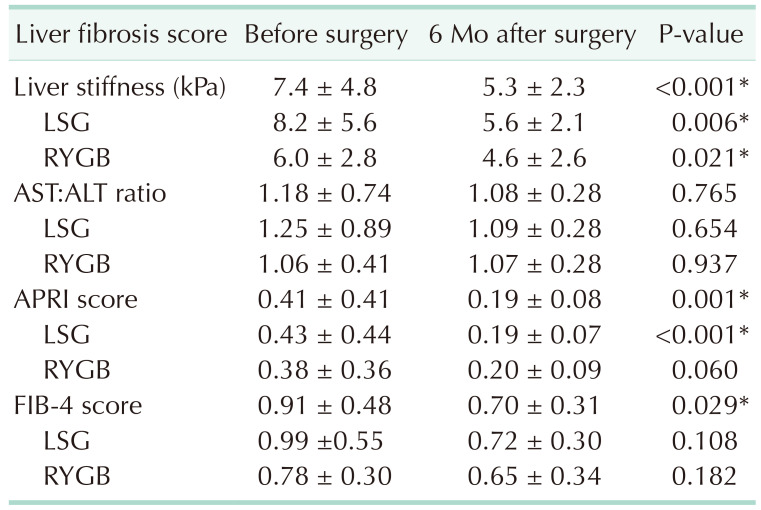
Table 3 shows the changes in liver fibrosis. There was a significant decrease in LS (measured using TE) in all patients (P < 0.001). The LSG (P = 0.006) and RYGB groups (P = 0.021) also showed statistically significant changes. These data are shown in Fig. 2. However, the results of the serological tests were significant only in the APRI and FIB-4 indices in all patients. In the APRI score, only the LSG group showed significant changes. There were no significant changes in the AST:ALT ratio.
Changes in the laboratory parameters
The changes in the laboratory parameters are shown in Table 4. There were statistically significant changes in hemoglobin A1C (HbA1C), AST, ALT, HDL, and TG levels.
Change in the number of nonalcoholic fatty liver disease patients
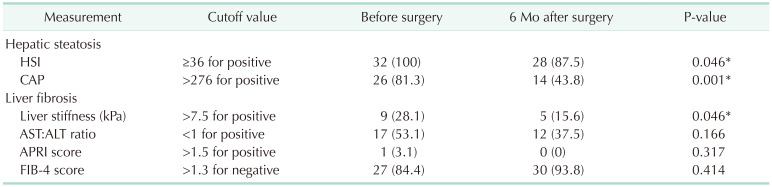
Table 5 shows the changes in NAFLD patients according to the measurement method. For hepatic steatosis, the number of patients diagnosed with NAFLD decreased in both HSI and CAP methods. Liver fibrosis measurement showed a statistically significant decrease in the number of patients in LS (kPa) measurement using TE. There was no significant difference in AST:ALT ratio, APRI score, and FIB-4 score, but improvement was found within the NAFLD diagnostic criteria.
DISCUSSION
In Korea, there is a growing interest in NAFLD, and updated Korean guidelines have been published [22]. Although the therapeutic role of bariatric surgery for Korean patients in the guidelines has not been confirmed yet, this study is expected to supplement the evidence for surgical treatment of patients with NAFLD. This study is the first to confirm the therapeutic effect of bariatric surgery in patients with NAFLD in Korea, and it showed good clinical results. In this study, NAFLD improved 6 months after bariatric surgery using validated noninvasive instruments. Both RYGB and LSG were associated with improvement in hepatic steatosis and liver fibrosis in terms of TE results.
Hepatic steatosis was evaluated using HSI and CAP using TE. This method has been validated in Korean patients, and the CAP diagnostic ability of moderate to severe degree of steatosis was 0.88 (sensitivity, 83.3%; specificity, 81.6%), and the cutoff value was 276 dB/m in a Korean study [13]. Twenty-six patients had CAP higher than 276 dB/m preoperatively. Six months after surgery, 31 patients showed improvement, and only 14 patients showed a result of 276 dB/m or higher. Thiry-one patients showed improvement in the CAP. Both the LSG and RYGB groups showed a decrease. An HSI of 36 or higher can be used to diagnose NAFLD with a specificity of 92.4% [16]. All patients in this study had a preoperative HSI of 36 or higher. Six months after surgery, the HSI decreased in all patients, but 28 patients still showed more than 36. Hepatic steatosis was observed in most patients, and even in Korean patients with a low BMI for the surgery. It is recommended that patients with a BMI of 30 kg/m2 or higher be closely monitored for hepatic steatosis. Notably, in our study, 6 months after bariatric surgery, hepatic steatosis improved regardless of the surgical method. Long-term observation results will be necessary.
Liver fibrosis scores improved after surgery in the present study. Nascimento et al. [23] also found an improved NAFLD fibrosis score 12 months after bariatric surgery. Several studies have shown good validity for APRI and FIB-4 scores in detecting liver fibrosis [1824].
In the case of liver fibrosis, 26 patients in this study showed improvement in the measurement results using TE. In the serologic panel, liver fibrosis showed improvement in the APRI and FIB-4 indices. In TE, both surgical groups improved, but only the LSG group in the APRI score showed a significant decrease in the results using the serologic panel. The diagnostic accuracy of FIB-4 does not appear to be high in Korean patients [25], and since there are not much data that have been validated for serological surrogates for liver fibrosis in Korea, more studies are needed in this area. The objective improvement of liver fibrosis after 6 months of surgery through TE was confirmed, but the serologic panel is considered to be insufficient for Korean people [22], so suitable models are needed. Among the laboratory parameters, HbA1C, AST, and ALT decreased, and HDL increased the T levels, which showed a positive change in the lipid composition.
Postoperative improvements after bariatric surgery have been reported in previous studies. A meta-analysis reported a positive effect of bariatric surgery on NAFLD. Significant clinical improvement or resolution of NAFLD was found in 50%–80% of patients 12–24 months after RYGB [26]. Another meta-analysis also showed improvements or resolution of liver steatosis, liver fibrosis, and steatohepatitis in 91.6%, 65.5%, and 81.3% of patients who had undergone bariatric surgery for up to 5 years, respectively [27]. The average BMI of NAFLD patients who underwent bariatric surgery in the meta-analysis is 48.68 ± 2.92 kg/m2 [28]. The BMI of Korean patients in this study was 39.3 ± 11.3 kg/m2, which is relatively lower than that of Western studies. In this study, short-term improvement in NAFLD findings was also observed in Koreans with relatively low BMI.
Although it was a short-term study, hepatic steatosis and liver fibrosis showed improvement in Korean patients even 6 months after bariatric surgery. The initial improvement is thought to be mainly due to metabolic changes and weight loss [29]. Since bariatric surgery is the most effective treatment for weight loss, NAFLD should also be considered an indication for bariatric surgery [30], and more detailed studies according to the surgical method and characteristics of the patient group are needed. In Korea, a country with a high rate of gastric cancer, it is difficult to screen the remnant stomach for gastric cancer; therefore, RYGB is strictly implemented. The weight of the LSG group before surgery was higher than that of the RYGB group, indicating a difference in these surgical indications. In this study, RYGB was the preferred procedure for those who did not have Helicobacter pylori infection or a family history of gastric cancer, and its indication was slightly different from that of the West. Therefore, further research and long-term research are required.
This study had several limitations. First, there are no liver biopsy data, which is the gold standard for the diagnosis of NAFLD. However, because TE also shows good performance, its potential as a useful tool is suggested in this study. In addition, the relatively short period of time and small number of patients was a potential limitation. If long-term follow-up results of more than 1 year can be obtained as well as 6 months, it could help in understanding the course of the disease. Since there are limited indications for RYGB in Korea, it is likely that research in this field is also needed. Research on NAFLD patients in countries with a high incidence of gastric cancer should be continued, and long-term follow-up is required.
In conclusion, the TE and serologic panel showed improvement in NAFLD 6 months after bariatric surgery in Korean patients with morbid obesity. Although long-term studies are needed, bariatric surgery can be considered as a treatment option to improve NAFLD in Asians, especially Koreans.

 XML Download
XML Download