

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Computed tomography (CT) plays a leading role in the identification and categorization of pneumonia in patients with coronavirus disease 2019 (COVID19). Typical and atypical CT features of COVID-19 pneumonia, including peripheral, bilateral, lower lobe, and posterior dominant distribution of ground-glass opacities (GGOs) with or without consolidations in lung regions, have been recently described.1234 Interlobular septal thickening, crazy-paving pattern, reversed halo sign, or other findings of organizing pneumonia have been reported depending on the time course of disease.45 In addition to the quantitative extent of pneumonia, CT features, including consolidation, linear opacities, and crazy-paving pattern, have been reported as factors that reflect the severity of COVID-19 and may have a potential role in prognostication.67
Among the CT features of COVID-19 pneumonia, mediastinal lymphadenopathy is rare and has a prevalence of 3-5% according to systematic meta-analyses.89 However, in one study conducted in France, mediastinal lymphadenopathy was observed in 66% of COVID-19 patients admitted to the intensive care unit (ICU).10 Similarly, other studies have reported that mediastinal lymphadenopathy was significantly more frequent in critically ill patients and those who died during hospitalization.71112 These studies suggest that there may be a potential link between the presence of mediastinal lymphadenopathy and COVID-19 severity; however, the association of mediastinal lymphadenopathy with disease severity and prognosis has not been clearly established.
This study aimed to determine whether the presence of mediastinal lymphadenopathy and specific clinical or CT characteristics are associated with COVID-19 disease severity and prognosis.
Go to : 
METHODS
Patients
The participants of this study included 522 patients enrolled in the Korean Imaging Cohort for COVID-19 (KICC-19), which was established by the Korean Society of Thoracic Radiology (KSTR) in July 202013 and 90 patients enrolled in two tertiary center cohorts (Chungbuk National University Hospital and Chonnam National University Hospital). From February 2020 to May 2020, 612 adult patients aged ≥ 18 years who were diagnosed with COVID-19 by real-time reverse transcriptase-polymerase chain reaction (RT-PCR) using nasal and oropharyngeal swabs were enrolled. Other respiratory pathogens capable of causing similar symptoms were excluded by RT-PCR and sputum cultures. Of these patients (n = 612), 344 underwent chest CT within 10 days of COVID-19 diagnosis and were included in the analysis. Patients with other causes of mediastinal lymphadenopathy, such as active cancer, sarcoidosis, or heart failure, were excluded.
Clinical data collection and definitions of clinical outcomes
Demographics, clinical symptoms, comorbidities, initial laboratory findings, and clinical outcomes of the 344 patients were evaluated. Laboratory analyses included neutrophil, lymphocyte, and thrombocyte counts and measurements of serum C-reactive protein (CRP) and blood urea nitrogen (BUN) levels. Clinical outcomes included the requirement for supplemental oxygen, ICU admission, acute respiratory distress syndrome (ARDS), and in-hospital death. ARDS was diagnosed based on the Berlin 2012 ARDS diagnostic criteria.14 In-hospital death was defined as deaths resulting from clinically compatible illnesses in patients with COVID-19 during hospitalization.15
CT imaging protocol and reconstruction profiles
All CT examinations were performed using multi-detector CT scanners with > 16 channels. Scans were obtained from the base to apex of each lung. Intravenous contrast medium was injected in 15 patients (4%). Of the 344 scans, 188 (55%) and 144 (42%) were obtained using slice thicknesses of ≤ 1.5 mm and 1.5-3 mm, respectively; only 12 CT scans (3%) were performed using a slice thickness of 5 mm. After anonymization, all images were transferred to the Asan Image Metrics Clinical Trial Center, a cloud-based data storage platform for research supported by the KSTR and the Korean Society of Radiology. In this system, a dedicated web viewer was provided for CT image analysis.
CT image analysis
Two thoracic radiologists (J.E.L. and Y.J.Y. with 7 and 13 years of chest CT experience, respectively) reviewed the CT images by consensus. If consensus was not achieved, the senior reader’s interpretation was accepted. The radiologists were blinded to patient clinical outcomes. Only the initial CT scan was analyzed if a patient underwent multiple CT examinations within 10 days of COVID-19 diagnosis. The time between symptom onset and CT scan was recorded for each patient.
Mediastinal lymphadenopathy was defined as one or more enlarged lymph nodes with a short-axis diameter of > 10 mm. Calcified enlarged mediastinal lymph nodes or anthracotic pigmented lymph nodes resulting from prior inflammation were excluded. Anthracotic pigmented lymph nodes were defined as those with > 70 HU according to the region-of-interest–based measurement, which indicates histopathologically internal fibrotic micronodule formation.16 The numbers and distribution of enlarged mediastinal lymph nodes were assessed according to the lymph node map of the International Association for the Study of Lung Cancer.17 Representative CT images of a COVID-19 patient with and without mediastinal lymphadenopathy are shown in Figs. 1 and 2.
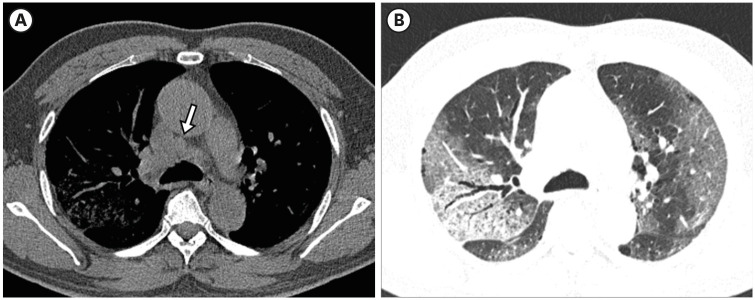 | Fig. 1Representative case of a coronavirus disease 2019 patient with mediastinal lymphadenopathy in a 71-year-old man. (A) Axial mediastinal-widow CT image shows an enlarged mediastinal lymph node in station 4R (white arrow). (B) Axial lung-window CT image obtained at the same level shows multifocal areas of ground-glass opacity with diffuse alveolar damage pattern in bilateral lungs.CT = computed tomography.
|
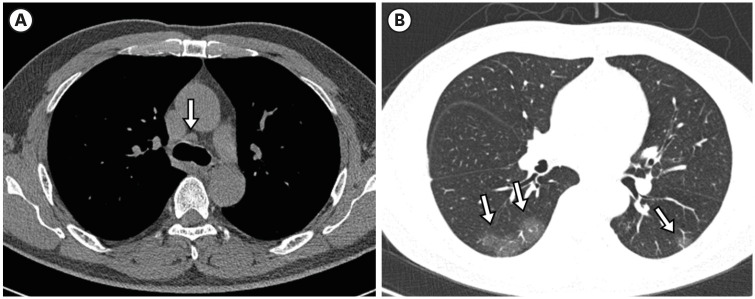 | Fig. 2Representative case of a coronavirus disease 2019 patient without mediastinal lymphadenopathy in a 75-year-old woman. (A) Axial mediastinal-widow CT image shows a small lymph node measuring less than 1 cm in short axis diameter at station 4R (white arrow). (B) Axial lung-window CT image shows small areas of ground-glass opacity in bilateral lower lobes (white arrows).CT = computed tomography.
|
CT findings of parenchymal abnormalities, including GGO, consolidation, reversed halo sign, reticulation, subpleural lines, crazy-paving patterns, traction bronchiectasis, and centrilobular nodules, were recorded. A reversed halo sign was defined as a focally rounded area of GGO surrounded by a complete or nearly complete ring of consolidation. A crazy-paving pattern was defined as a thickened interlobular septum and intralobular lines superimposed on a background of GGO.18 The presence of pleural effusion was also recorded. Distributions of parenchymal abnormalities in the axial (peripheral, peribronchovascular, and diffuse) and craniocaudal (upper to mid zone, lower zone, and random) planes were evaluated.
Bilateral involvement and diffuse alveolar damage (DAD) patterns were also recorded. A DAD pattern was defined as patchy or extensive air-space consolidation or GGO without zonal predominance. CT patterns of COVID-19 pneumonia were classified into typical, indeterminate, and atypical according to the Radiological Society of North America expert consensus document.4 The extent of each parenchymal lesion was assessed using a visual CT scoring system. Each lung lobe was visually scored from 0 to 5 as follows: 0, no involvement; 1, < 5%; 2, 5–24%; 3, 25–49%; 4, 50–74%; and 5, ≥ 75% involvement.19 Visual CT scores were the sum of the individual lobar scores and ranged from 0–25.
Statistical analysis
All statistical analyses were performed using SPSS software, version 25.0 (IBM, Armonk, NY, USA). The Pearson’s chi-square test for categorical variables and the independent t-test for continuous variables were used to determine the differences between clinical characteristics and CT findings in patients with and without mediastinal lymphadenopathy.
Inter-reader agreement for the presence or absence of mediastinal lymphadenopathy was calculated as κ of agreement. κ < 0.40 was interpreted as poor agreement, 0.41–0.60 as moderate, 0.61-0.80 as substantial, and 0.81–1 as almost perfect agreement according to Cohen’s kappa coefficient.20
To evaluate the correlation between the number of enlarged lymph nodes and the extent of pneumonia, Spearman’s correlation analysis was performed. Factors associated with ICU admission were identified by univariate and multivariate logistic regression analysis. Those associated with in-hospital death was identified by univariate and multivariate Cox proportional-hazard model. Differences were considered statistically significant at P < 0.05.
Ethics statement
This retrospective study was approved by the Institutional Review Board of our institutions (approval numbers CBNUH 2020-04-003 and CNUH-2020-123), and the requirement for informed consent was waived owing to the retrospective nature of the study.
Go to :
RESULTS
Baseline characteristics of COVID-19 patients
The mean time between symptom onset and chest CT examination was 5.8 ± 4.6 days (range: 0-10). The baseline clinical characteristics of the 344 patients, all of whom underwent a chest CT scan, are presented in Table 1. A total of 127 (39.0%) patients had at least one comorbidity, such as hypertension, diabetes, cardiovascular disease, history of cancer, chronic obstructive pulmonary disease (COPD), chronic kidney disease, dyslipidemia, chronic liver disease, asthma, and dementia, and 275 (79.9%) patients had at least one COVID-19 symptom. Of the 344 patients included in this study, 82 (23.8%) required supplemental oxygen, 34 (9.9%) were admitted to the ICU, 16 (4.7%) developed ARDS, and 10 (2.9%) died during their hospital stay. The mean length of hospitalization was 27.99 ± 14.7 days.
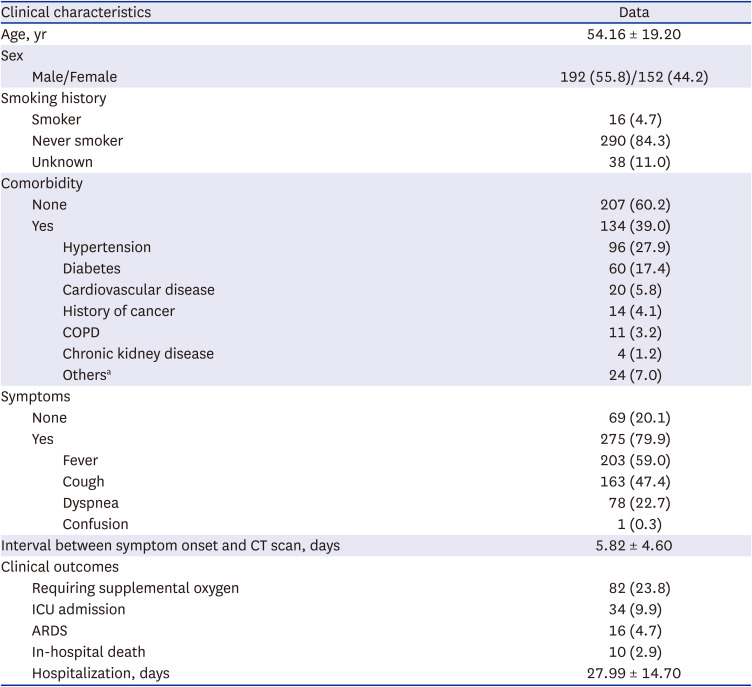
Table 1
Baseline clinical characteristics of patients with COVID-19 at hospital admission (N = 344)
Values are number (%) of cases. Values are presented as mean ± standard deviation, where applicable.
COVID-19 = coronavirus disease 2019, COPD = chronic obstructive pulmonary disease, CT = computed tomography = ICU = intensive care unit, ARDS = acute respiratory distress syndrome.
aOthers included dyslipidemia (n = 10), chronic liver disease (n = 5), hypothyroidism (n = 3), asthma (n = 3), and dementia (n = 1).
![]()
Clinical characteristics of patients with and without mediastinal lymphadenopathy
The clinical characteristics of the patients with and without mediastinal lymphadenopathy are summarized in Table 2. Of the 344 patients included in this study, 53 (15.4%) had mediastinal lymphadenopathy, with a higher mean age than patients without mediastinal lymphadenopathy. Having at least one comorbidity and COVID-19 symptoms were significantly more common in patients with mediastinal lymphadenopathy than in those without (P < 0.001, P < 0.001, and P = 0.004, respectively). The CRP level was significantly higher in patients with mediastinal lymphadenopathy than in those without (P < 0.001); however, no significant differences between the two groups were observed in terms of neutrophil, lymphocyte, and thrombocyte counts and BUN levels. The number of patients with mediastinal lymphadenopathy requiring oxygen supply, ICU admission, and ARDS were significantly higher than those without (P < 0.001).
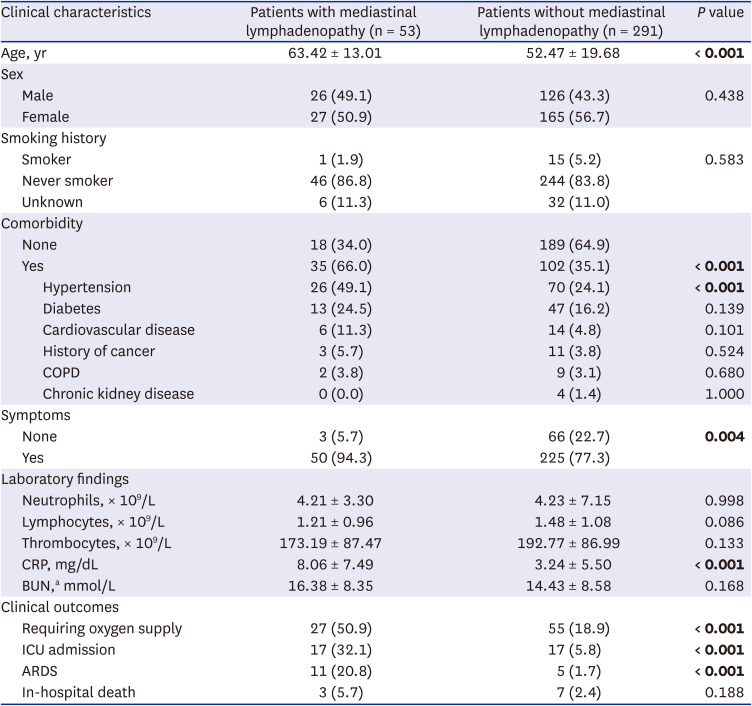
Table 2
Clinical characteristic of patients with and without mediastinal lymphadenopathy
Values are number (%) of cases. Values are presented as mean ± standard deviation, where applicable. Significant P values are shown in bold.
COPD = chronic obstructive pulmonary disease, CRP = C-reactive protein, BUN = blood urea nitrogen, ICU = intensive care unit, ARDS = acute respiratory distress syndrome.
aBUN result was available for 294 patients.
![]()
CT findings in patients with and without mediastinal lymphadenopathy
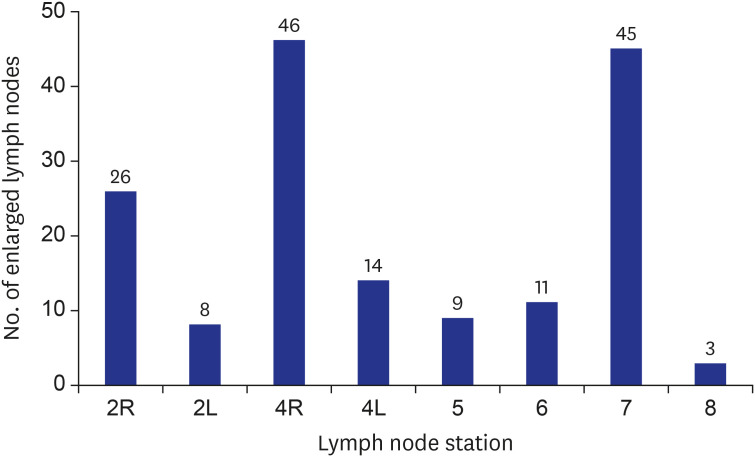
The number and distribution of enlarged mediastinal lymph nodes in patients with mediastinal lymphadenopathy are summarized in Fig. 3. The most common regions for mediastinal lymphadenopathy were stations 4R, 7, and 2R in this order. The degree of agreement in identifying the presence or absence of mediastinal lymphadenopathy between the two readers was almost perfect (κ = 0.890).
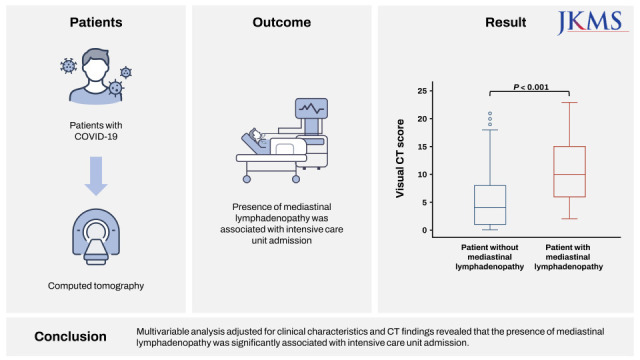
Visual CT scores were significantly higher in patients with mediastinal lymphadenopathy than in those without (P < 0.05) (Fig. 4). The number of enlarged mediastinal lymph nodes was positively correlated with visual CT scores (Spearman’s ρ = 0.334, P < 0.001) (Fig. 5A) and CRP level (ρ = 0.307, P = 0.025) (Fig. 5B).
 | Fig. 4Mean visual CT score of coronavirus disease 2019 patients with or without mediastinal lymphadenopathy. The mean visual CT score was significantly higher in those with mediastinal lymphadenopathy than those without (P < 0.001).CT = computed tomography.
|
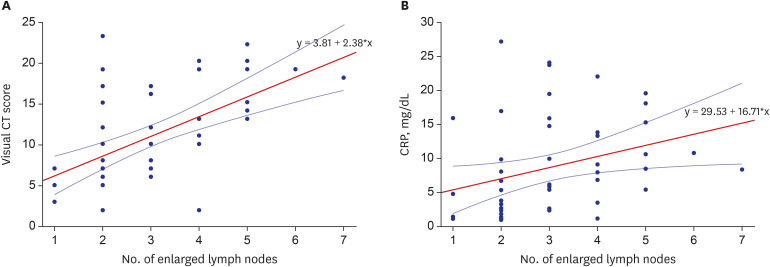 | Fig. 5Correlation of the number of enlarged lymph nodes with visual CT scores and CRP level. (A) Scatter plot of the number of enlarged lymph nodes with visual CT scores and the CRP level. There was a positive correlation between the number of enlarged lymph nodes and the visual CT scores (Spearman’s ρ = 0.334, P < 0.001). (B) There was a positive correlation between the number of enlarged lymph nodes and the CRP levels (Spearman’s ρ = 0.307, P = 0.025).CT = computed tomography, CRP = C-reactive protein.
|
The CT findings of COVID-19 pneumonia patients with and without mediastinal lymphadenopathy are summarized in Table 3. Of the 344 patients, 58 (16.8%) had normal chest CT findings. The rate of any parenchymal abnormalities detected on chest CT scan was significantly higher in patients with mediastinal lymphadenopathy than those without. Parenchymal abnormalities, including consolidation, crazy-paving pattern, reversed halo, reticulation, subpleural line, and traction bronchiectasis, and pleural effusion were more common in patients with than without mediastinal lymphadenopathy (Table 3). The frequencies of diffuse axial distribution and random craniocaudal distribution were higher in patients with mediastinal lymphadenopathy than in those without. Similarly, patterns of bilateral involvement and DAD pattern were significantly more common patients with mediastinal lymphadenopathy. The frequency of CT pattern was not significantly different between the two groups.
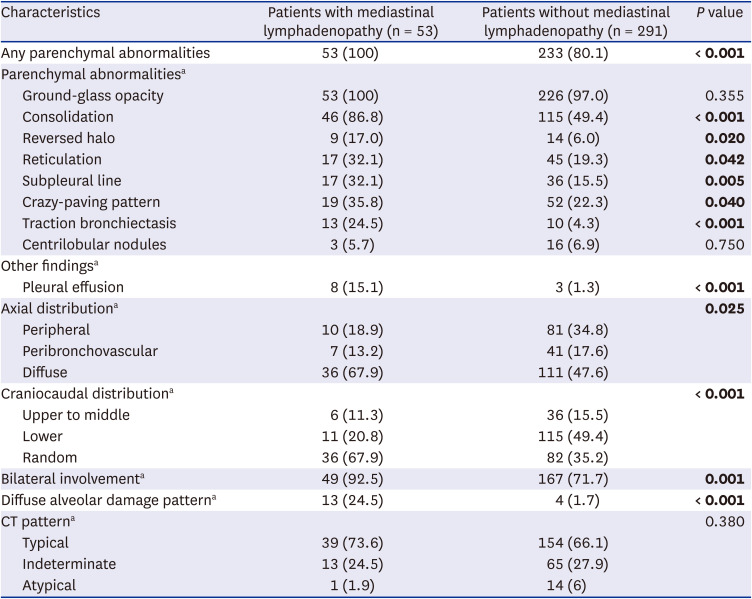
Table 3
CT findings of COVID-19 pneumonia in patients with and without mediastinal lymphadenopathy
Values in parentheses are percentages. Significant P values are shown in bold.
CT = computed tomography, COVID-19 = coronavirus disease 2019.
aResults from 286 patients.
![]()
Risk factors related to ICU admission of COVID-19 patients
Univariate and multivariate logistic regression analyses for risk factors related to ICU admission of patients with COVID-19 are summarized in Table 4. Univariate analysis revealed the following as significant factors related to ICU admission of patients with COVID-19 pneumonia: older age; male sex; hypertension, diabetes, and cardiovascular disease; higher neutrophil count; higher CRP level; presence of mediastinal lymphadenopathy; presence of DAD pattern pneumonia; and higher visual CT scores. Multivariate logistic regression analysis adjusted for clinical characteristics and CT findings revealed that male sex (odds ratio [OR], 3.76; 95% confidence interval (CI), 1.25–11.31), higher level of CRP (OR, 1.11; 95% CI, 1.03–1.21), presence of mediastinal lymphadenopathy (OR, 3.25; 95% CI, 1.06–9.95), and higher visual CT scores (OR, 1.25; 95% CI, 1.10–1.44) were independent significant factors related to ICU admission of COVID-19 patients.
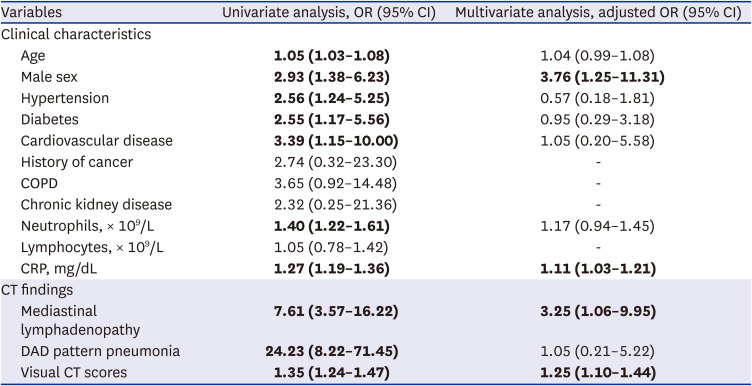
Table 4
Odds ratiosa for ICU admission among COVID-19 patients
aSignificant ORs are shown in bold.
ICU = intensive care unit, COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, COPD = chronic obstructive pulmonary disease, CRP = C-reactive protein, CT = computed tomography, DAD = diffuse alveolar damage.
![]()
Risk factors related to in-hospital death of patients with COVID-19
Univariate and multivariate Cox proportional-hazards models for risk factors related to in-hospital death of patients with COVID-19 are summarized in Table 5. Univariate analysis revealed that older age, male sex, hypertension, diabetes, cardiovascular disease, and COPD, higher neutrophil count, higher CRP level, presence of DAD pattern pneumonia, and higher visual CT scores were significant factors related to in-hospital death of COVID-19 patients. Multivariate analysis adjusted for clinical characteristics and CT findings revealed that diabetes (hazard ratio [HR], 26.58; 95% CI, 3.08–229.58), COPD (HR, 32.00; 95% CI, 2.13–482.01), chronic kidney disease (HR, 27.08; 95% CI, 1.53–479.94), and higher level of CRP (HR, 1.19; 95% CI, 1.04–1.37) were independent significant factors related to in-hospital death of COVID-19 patients.
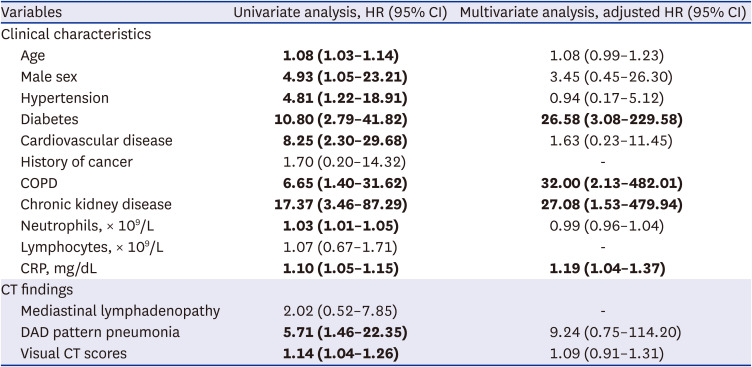
Table 5
Hazard ratiosa for in-hospital death among COVID-19 patients
COVID-19 = coronavirus disease 2019, HR = hazard ratio, CI = confidence interval, COPD = chronic obstructive pulmonary disease, CRP = C-reactive protein, CT = computed tomography, DAD = diffuse alveolar damage.
aSignificant HRs are shown in bold.
![]()
Go to :
DISCUSSION
This study evaluated the clinical implication and prognostic role of mediastinal lymphadenopathy in patients with COVID-19 pneumonia. Mediastinal lymphadenopathy was observed in 15.4% of the study cohort. Our results suggest that the frequency of any parenchymal abnormalities on chest CT scans and visual CT scores were significantly higher in patients with mediastinal lymphadenopathy than in those without. Among the patient with presence of pneumonia on chest CT scans, the rate of DAD pattern was significantly higher in patients with mediastinal lymphadenopathy than in those without. Adjusted multivariate logistic regression analysis showed male gender, higher level of CRP, higher visual CT score, and presence of mediastinal lymphadenopathy were independently associated with a higher risk of ICU admission in patients with COVID-19 pneumonia. Adjusted multivariate Cox proportional-hazards model showed diabetes, COPD, and higher level of CRP were independently associated with a higher risk of in-hospital death in our study.
Parenchymal abnormalities, including consolidation, crazy-paving patterns, reversed halo sign, reticulation, subpleural line, traction bronchiectasis, and pleural effusion, were more frequently observed in patients with mediastinal lymphadenopathy. We found that all patients with mediastinal lymphadenopathy had at least one parenchymal abnormality. These parenchymal abnormalities indicate disease progression and severity in patients with COVID-19 as reported by previous studies.721 Moreover, the visual CT score, which reflects the overall burden of parenchymal abnormalities in our study, was significantly higher in patients with mediastinal lymphadenopathy than those without. This quantitative burden of pneumonia has been previously demonstrated as a significant predictive factor for adverse outcomes, such as ICU admission, mechanical ventilation, vasopressor therapy, or death, of COVID-19 pneumonia patients.22 Additionally, the presence of mediastinal lymphadenopathy and the more extensive parenchymal involvement of pneumonia have been more commonly observed in COVID-19 pneumonia than other types of viral pneumonia,23 indicating that COVID-19 pneumonia induces a stronger immune response than other viral pneumonias. Furthermore, we found that not only the visual CT score but also the CRP level was significantly higher in patients with mediastinal lymphadenopathy than in those without, and that the number of enlarged lymph nodes was significantly correlated with both visual CT scores and CRP level. Therefore, the presence of mediastinal LAP may reflect active inflammation and host immune response of the lung in patients with COVID-19 and may have a significant association with severe COVID-19 pneumonia.
We found that DAD pattern, as well as bilateral and diffuse involvement, of COVID-19 pneumonia was more frequently observed in patients with mediastinal lymphadenopathy than in those without. DAD is a histologic hallmark of ARDS in patients with COVID-19.24 Jeong et al.25 identified extensive parenchymal abnormalities and DAD patterns of COVID-19 pneumonia as independent factors associated with clinical severity and poor clinical outcome, regardless of clinical risk factors. Jin et al.26 found that the DAD pattern of COVID-19 pneumonia was significantly correlated with adverse outcomes, including ICU admission, use of mechanical ventilation, or death, as well as pulmonary residual sequelae. The higher frequency of DAD pattern pneumonia we noted in patients with mediastinal lymphadenopathy may be associated with worse clinical outcomes in these patients.
In our study, mediastinal lymphadenopathy was significantly associated with ICU admission in patients with COVID-19 but not with in-hospital deaths. These findings are inconsistent with a previous study on the relationship between mediastinal lymphadenopathy and 30-day mortality in patients with COVID-19.12 The mortality rate reported in this previous study was 8.4%, whereas that in our study was 2.9%. Moreover, in the previous study, the mean age of the patients was 56.9 years, and the rate of comorbidity was 53.5%. In our study, the mean age was 54.1 years, and the comorbidity rate was 37.2%. Differences in the prevalence rates of COVID-19 may have influenced the distribution of hospitalized patients, which may have resulted in differences in comorbidity and in-hospital death rates between these two studies.
Our study showed associations between the risk of poor clinical outcomes, such as ICU admission and in-hospital death, and clinical characteristics. Among the clinical characteristics, we found that male sex and higher level of CRP were significantly associated with increased risk of ICU admission and that older age, diabetes, COPD, chronic kidney disease, and higher CRP level were significantly associated with increased risk of in-hospital death in patients with COVID-19. According to data adopted by the Centers for Disease Control and Prevention, older age, diabetes, COPD, and chronic kidney disease are risk factors for severe COVID-19.27 In a previous study analyzing the risk factors for poor clinical outcome of COVID-19 patients in Korea, older age, male sex, and higher number of comorbidities (including diabetes, COPD, and chronic kidney disease) were similarly identified as risk factors associated with in-hospital death and severe cases requiring oxygen therapy.28 Elevated CRP level, indicative of an inflammatory condition, was also reported as a risk factor for severe disease course and in-hospital death in patients with COVID-19.2930 These findings are consistent with our results.
This study had some limitations that warrant consideration. First, there may have been a selection bias owing to the retrospective study design and the inclusion of COVID-19 patients who underwent chest CT. Second, the timing between symptom onset and CT scan varied, which may have affected CT results. However, to address this limitation, we included patients who underwent chest CT within 10 days of RT-PCR-based diagnosis. Third, as most CT images were non-enhanced CT, there was a limitation in the evaluation of lymph nodes; therefore, evaluation of hilar lymph node was not performed. Fourth, serial CT scans over time were not evaluated in our study; thus, it was difficult to evaluate the association between long-term prognosis and the presence of mediastinal lymphadenopathy. Further studies that include long-term follow-up CT scans are required.
In conclusion, COVID-19 patients with mediastinal lymphadenopathy had a larger extent of pneumonia than those without. Multivariate analysis adjusted for clinical characteristics and CT findings revealed that the presence of mediastinal lymphadenopathy was independently associated with ICU admission. Thus, mediastinal lymphadenopathy should not be overlooked and may be considered as reflective of COVID-19 pneumonia severity.
Go to :
 XML Download
XML Download