

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Crossmatching is the assessment of the immune compatibility of a particular donor and the recipient. The association between positive crossmatches and hyperacute rejection was first demonstrated in the 1960s with renal transplantation.1 Over the following decades, a positive crossmatch result began to be considered a contraindication to transplantation because of its devastating postoperative effects.23 In particular, complement-dependent cytotoxicity (CDC) results against T lymphocytes are considered an absolute contraindication.34 However, the meaning of positive crossmatches has changed with the development of crossmatching methodology and immunosuppression strategies.56 Early research suggested that it was crucial to avoid the impact of positive T cell crossmatches on renal transplantation; however, because of their low specificity and sensitivity, recent analyses have found that avoidance is not mandatory.2 A combination of different crossmatching techniques has recently been recommended for solid organ transplantations.7
In lung transplantation, considering the limited number of available donors, persistent demand for required organs, and risk of increasing incidences of wait-list mortality and morbidity, immunological “mismatches” have to be accepted despite the potential for the development of donor-specific antibodies (DSAs), which can trigger antibody-mediated rejection (AMR).8910 A pretransplant crossmatch is not mandatory in the lung allocation system suggested by the International Society of Heart and Lung Transplantation (ISHLT); interpretation and decisions are left to local protocols of each center and no definitive guidelines are available.7810
According to the Korea donor allocation system, pretransplant crossmatching is only considered mandatory for renal and pancreas transplantation; the system does not play a role in nonrenal transplantation, including lung transplantation. According to a report from Korean Network for Organ Sharing, there was no lung transplantation with positive crossmatching between March 2014 to February 2015.11 However, the total number of nationwide lung transplantations has almost tripled since 2014 (55 cases in 2014; 64 cases in 2015; 89 cases in 2016; 93 cases in 2017; 92 cases in 2018; 157 cases in 2019)12; thus, the incidences and outcomes of positive crossmatching are worthy of analysis. In this study, we aimed to investigate the positive crossmatch rate in lung transplantation and their posttransplant outcomes using a multicenter nationwide cohort. In addition, we analyzed the impact of each crossmatch technique on the crossmatching results to clarify the meaning of positive crossmatching.
Go to : 
METHODS
Lung transplant cohort
Clinical lung transplantation data were derived from patients who received lung transplantation from deceased donors at one of five tertiary centers which performed more than 10 cases annually between 2010 to 2012 in South Korea via the Korean Organ Transplant Registry (KOTRY). The KOTRY was established in 2014 and began to organize the lung transplantation registry in 2015.13 We analyzed the data on registered lung transplantations performed between March 2015 and December 2019. Among these patients, ten patients who did not undergo crossmatching were excluded. Finally, 210 patients were included in the study.
Clinical data, including the general demographic characteristics, primary diagnosis, and pretransplant status of the recipients and donors, were prospectively collected. The details of desensitization protocols, transplant operations, and postoperative follow-up results were also prospectively collected. All clinical data were collected and registered using a web-based report form by the attending physician.
Because of donor shortage, transplantation was performed regardless of the status of DSA screening. Moreover, according to a medical urgency-based allocation system in Korea, the results of human leukocyte antigen (HLA) crossmatching were not regarded as mandatory considerations.14 Most patients received induction therapy with high-dose steroids (methylprednisolone, 500 mg) or interleukin-2 antagonist followed by a standard triple immunosuppressant regimen consisting of prednisolone, mycophenolate, and tacrolimus, except when there were contraindications to these medications. Pretransplant immunological results did not affect the choice of immunosuppressant regimen. Desensitization protocols, including plasma exchange and intravenous infusion of immunoglobulin, were considered after transplantation in patients with pretransplant DSA and high mean fluorescence intensity (MFI).
HLA crossmatching and other immunologic evaluation
The Korean Organ Donation Agency (KODA) laboratory performed crossmatching of registered lung transplantations. Both CDC crossmatch (CDC-XM) and flow cytometric crossmatch (flow-XM) were performed. Although virtual crossmatch techniques have gained influence in many countries, they are currently unavailable in Korea.
For the CDC crossmatch, both T and B lymphocytes were isolated by negative selection methods using the EasySep HLA Total Lymphocyte Enrichment kit (STEMCELL Technologies Inc., Tukwila, WA, USA). Both the National Institutes of Health and antihuman globulin augmented methods were performed using standard protocols with some minor modifications.11 Cells and duplicate serum dilutions of 1:1 to 1:4, respectively, were incubated at 25°C for 30 minutes for complement reaction. Cells were stained with commercial staining reagent (FluoroQuench Stain; One Lambda, Canoga Park, CA, USA) and observed under an inverted fluorescent microscope. The positive crossmatch results were recorded when the cytotoxic reaction resulted in more than 11% cell lysis.
For flow-XM, both T and B lymphocytes were stained using three-color immunofluorescence staining in a single tube as previously described,1415 with minor modifications. After the incubation of cells and serum at 25°C for 15 minutes, a fluorescent conjugate reaction was performed at 25°C for 20 minutes using titrated goat F(ab’)2 antihuman immunoglobulin G fluorescein isothiocyanate (Jackson Immunoresearch Laboratories, West Grove, PA, USA), anti-CD3 PerCP (Becton Dickinson, San Jose, CA, USA), and anti-CD19 allophycocyanin conjugates (Becton Dickinson). Fluorescence was analyzed using a FACSCalibur Flow Cytometer with an HTS microplate acquisition system (Becton Dickinson). Fluorescence was considered positive when the MFI ratio to negative reference test was over 2.0 for both T and B lymphocytes.
Panel reactive antibody (PRA) class I and II identifications were performed before transplantation with the identification kit (One Lambda, Inc., West Hills, CA, USA or Gen-Probe Inc., San Diego, CA, USA). PRA over 10% was considered positive, and over 50% was considered highly sensitized.16 Antibodies against donor HLA-A, B, DR, and DQ were defined DSAs, and the strength of each DSA was quantified based on MFI.
Clinical outcomes
Clinical outcomes, including acute rejection, primary graft dysfunction (PGD), chronic lung allograft dysfunction (CLAD), and mortality, were analyzed. Acute cellular rejection (ACR) was diagnosed according to the ISHLT grading system with a transbronchial biopsy specimen.17 However, not all treated recipients with acute rejection were available for transbronchial biopsies for histopathologic confirmation. As such, clinical diagnosis of acute rejection was also assumed when allograft dysfunction without definite entities was responsive to steroid pulse therapy. Though there is no distinct definition of AMR in lung transplantation, AMR was diagnosed as per a proposal published by the ISHLT in 2016, including allograft dysfunction, lung histology, C4d+, and DSA without other explainable causes.818
PGD in lung transplantation was defined as an allograft dysfunction of the transplanted lung within the first 72 hours after the procedure. PGD was diagnosed and graded according to the ISHLT criteria.19 Bronchiolitis obliterans syndrome (BOS) and restrictive allograft syndrome (RAS) were the two main phenotypes of CLAD, which represented the irreversible loss of lung function and a major cause of limiting long-term survival. BOS was identified by the sustained and irreversible reduction in forced expiratory volume in 1 second (FEV1) compared with the post-lung transplant baseline FEV1 in the absence of any other etiologies.20 RAS is defined by restrictive physiology according to a pulmonary function test, positive findings of a radiologic study, the presence of ground-glass opacity, and interstitial fibrosis.21
Statistical analysis
Descriptive statistics were used to demonstrate baseline clinical characteristics of the study cohort. For categorical variables, data are shown as numbers and percentages, and chi-squared or Fisher’s exact tests were used where appropriate. For continuous variables, data were analyzed using Student’s t-test or Mann-Whitney U test and presented as the mean ± standard deviation or the median, interquartile range (IQR). Univariable and multivariable regression analysis was used to evaluate the factors associated with clinical outcomes. To confirm the independent association between variables, linear regression was applied for confounders. Survival analysis was performed by the Kaplan-Meier method with log-rank tests. All statistical analysis was performed with SPSS (version 25.0; SPSS Inc., Chicago, IL, USA), and a P value < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of the Severance Hospital of Yonsei University (IRB No. 4-2021-0673). The IRB waived the requirement for obtaining informed consent from the patients.
Go to :
RESULTS
Baseline characteristics
The baseline characteristics of the patients according to the results of crossmatches are shown in Table 1. Among the included 210 recipients, nine patients showed positive crossmatches. The median age was 56.4 years, and 134 patients (63.8%) were male. Only one patient was male in the positive crossmatch group. There was no RH− blood type within the study cohort. The most common primary diagnosis was idiopathic pulmonary fibrosis (114 patients, 54.3%), followed by connective tissue-related interstitial lung disease (CTD-ILD) (34 patients, 16.2%). The median number of days on the waiting list was 71.0, and 63 patients (30.0%) had undergone pretransplant extracorporeal membrane oxygenation support. The baseline characteristics were not significantly different between the positive and negative crossmatch groups.
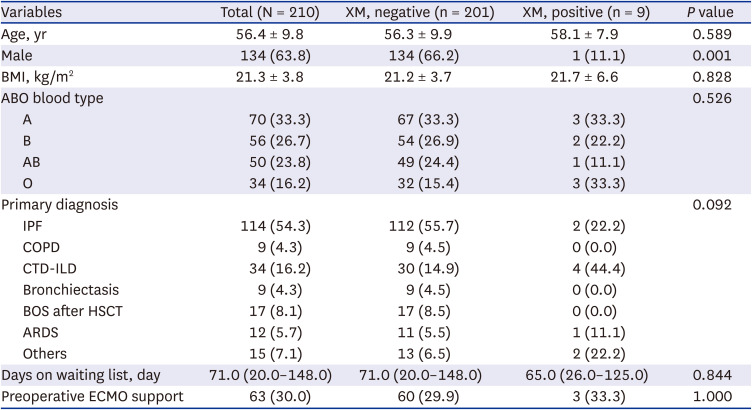
Table 1
Baseline characteristics
Values are presented as mean ± standard deviation or number (%).
XM = crossmatch, BMI = body mass index, COPD = chronic obstructive pulmonary disease, CTD-ILD = connective tissue-related interstitial lung disease, BOS = bronchiolitis obliterans syndrome, ECMO = extracorporeal membrane oxygenation, ARDS = acute respiratory distress syndrome, IPF = idiopathic pulmonary fibrosis, HSCT = hematopoietic stem cell transplantation.
![]()
Table 2 shows the results of immunological evaluations, including crossmatching. CDC-XM was performed in 208 patients (99.0%) and flow-XM was performed in 125 patients (59.5%). PRA was identified in 208 patients (99.0%). Among these patients, high levels of class I or class II PRA (> 50%) were detected in 18 patients (8.7%). The proportion of patients with high PRA was higher in the positive crossmatch group than in the negative crossmatch group (37.5% vs. 10.7%, P = 0.026).
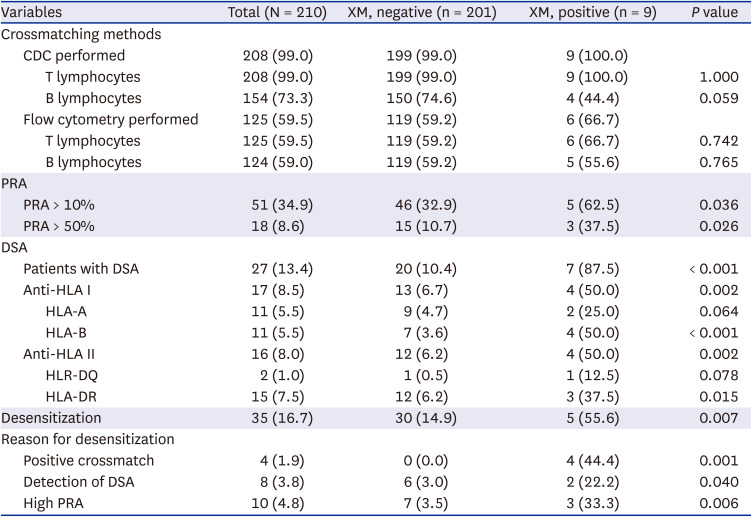
Table 2
Immunologic evaluation for transplantation
Values are presented as number (%).
XM = crossmatch, CDC = complement-dependent cytotoxicity, PRA = panel-reactive antibody, DSA = donor specific antibody, HLA = human leukocyte antigen.
![]()
At the time of lung transplantation, most patients (201 patients, 95.7%) had undergone the DSA screening test. Twenty-seven patients (13.4%) were revealed to have DSA. A higher proportion of the patients in the positive crossmatch group had DSA (7 patients, 87.5%, vs. 20 patients, 10.4%, P < 0.001) compared with that in the negative crossmatch group. Desensitization was performed in 35 patients (16.7%), and four patients in the positive crossmatch group underwent desensitization.
The characteristics of nine patients with positive crossmatch are shown in Table 3. Among these patients, the most common etiology for lung transplantation was CTD-ILD. CDC-XM and flow-XM revealed positive crossmatches in five and six patients, respectively. DSA was detected in six patients, and three patients (patient numbers 5, 6, and 7) had an MFI higher than 5,000. Five patients underwent desensitization before lung transplantation. Acute rejection was diagnosed in three patients (patient numbers 3, 4, and 6), and two patients underwent transbronchial lung biopsy (patient numbers 3 and 4). Patient number 6 was positively crossmatched to the donor as observed using CDC-XM with both T land B lymphocytes, and class I DSA was detected with MFI over 5,000. The patient was clinically diagnosed with AMR and received aggressive treatments for rejection, including steroid pulse, plasmapheresis, and intravenous infusion of immunoglobulin. However, the patient received retransplantation on postoperative day 15 due to rejection.
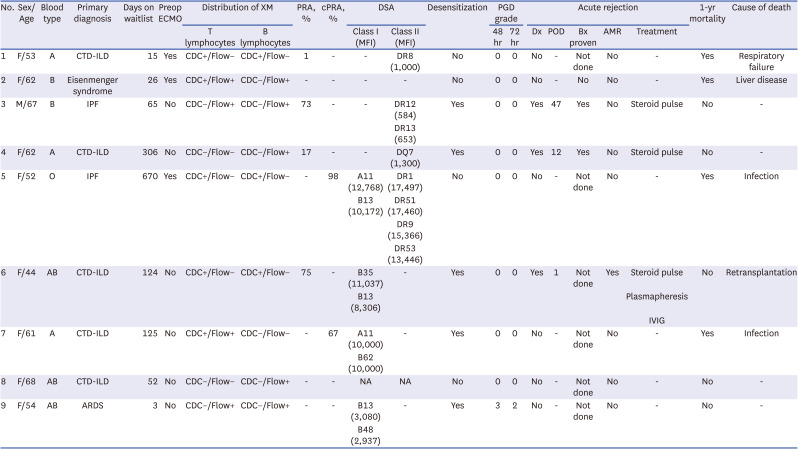
Table 3
Characteristics of patients with positive crossmatch
XM = crossmatch, CTD-ILD = connective tissue-related interstitial lung disease, ECMO = extracorporeal membrane oxygenation, CDC = complement-dependent cytotoxicity, PRA = panel-reactive antibody, DSA = donor specific antibodies, PGD = primary graft dysfunction, MFI = mean fluorescence intensity, AMR = antibody-mediated rejection, ARDS = acute respiratory distress syndrome, IPF = idiopathic pulmonary fibrosis, IVIG = intravenous immunoglobulin.
![]()
Operative details and postoperative outcomes
Most patients underwent bilateral lung transplantation (202 patients, 96.2%). According to the PGD grade, patients presenting with grade 3 at postoperative 48 hours or 72 hours were regarded as high-grade PGD. Forty-four patients showed high-grade PGD, and no statistical difference was observed between the groups. The incidences of other postoperative complications, including postoperative bleeding, anastomosis dehiscence, pulmonary thromboembolism, pneumonia, and acute kidney injury, were not statistically distinguishable between the groups (Table 4).
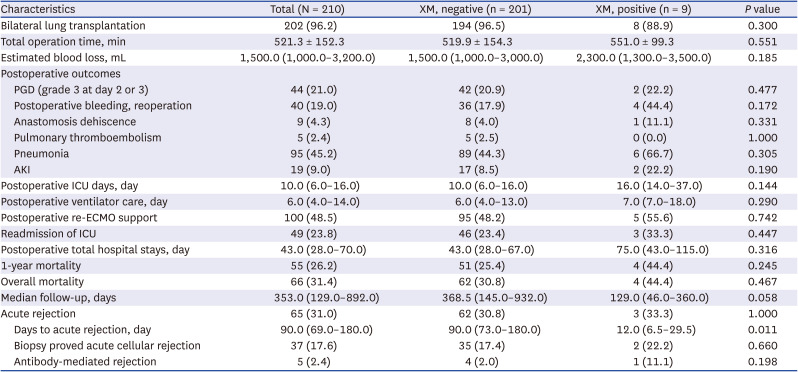
Table 4
Operative and postoperative outcomes
Values are presented as number (%), mean ± standard deviation or number (interquartile range).
XM = crossmatch, PGD = primary graft dysfunction, ECMO = extracorporeal membrane oxygenation, ICU = intensive care unit, AKI = acute kidney injury.
![]()
Acute rejection was diagnosed in 65 patients. Transbronchial lung biopsy-proven ACR was diagnosed in 37 patients, and other patients were diagnosed clinically. Though the incidence of acute rejection with regard to crossmatching results was not statistically different between the groups, the positive crossmatch group showed shorter intervals between transplantation and diagnosis of rejection. Five patients had clinical presentations that were compatible with AMR. However, none of these patients were diagnosed using the biopsy specimen or capillary C4d composition. Seven patients (3.3%) showed physiologic changes that were considered as CLAD. BOS was diagnosed in five patients (2.4%), and RAS was diagnosed in three patients (1.4%). The median number of days from transplant to CLAD diagnosis was 648 (IQR, 488.0–759.0). All of the patients showed CLAD were in the negative crossmatch group.
Survival analysis
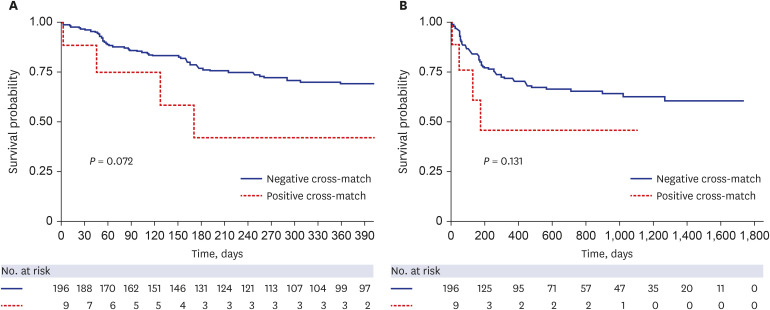
As shown in Table 4, 55 patients (26.2%) showed 1-year mortality. The 1-year and overall mortality rates were not statistically different between the groups (Table 4). Fig. 1 shows the Kaplan-Meier curves of 1-year and overall mortality rates of the patients. According to Kaplan-Meier analysis, there were no significant differences in the survival rates, regardless of crossmatching status.
We also performed a regression analysis to identify the risk factors for poor 1-year survival. Positive CDC crossmatching was the only significant risk factor for poor 1-year survival in the univariable analysis (odds ratio, 11.922, 95% confidence interval, 1.302–19.125, P = 0.018).
We further divided the patients based on crossmatching methods and performed survival analysis for the subgroups. When positive crossmatching was confirmed by CDC-XM, the post-transplant 1-year and overall mortality rates were poorer than the negative crossmatching results (P < 0.001 and P < 0.001, respectively) (Fig. 2A and B). According to the Kaplan-Meier method, positive crossmatching by the flow-XM method did not significantly differ in the 1-year and overall morality (Fig. 2C and D). When considering the detection of T and B lymphocytes individually, only positive crossmatching by T lymphocytes was related to mortality within 1-year after transplantation (P = 0.002) and overall mortality (P = 0.006) (Fig. 3).
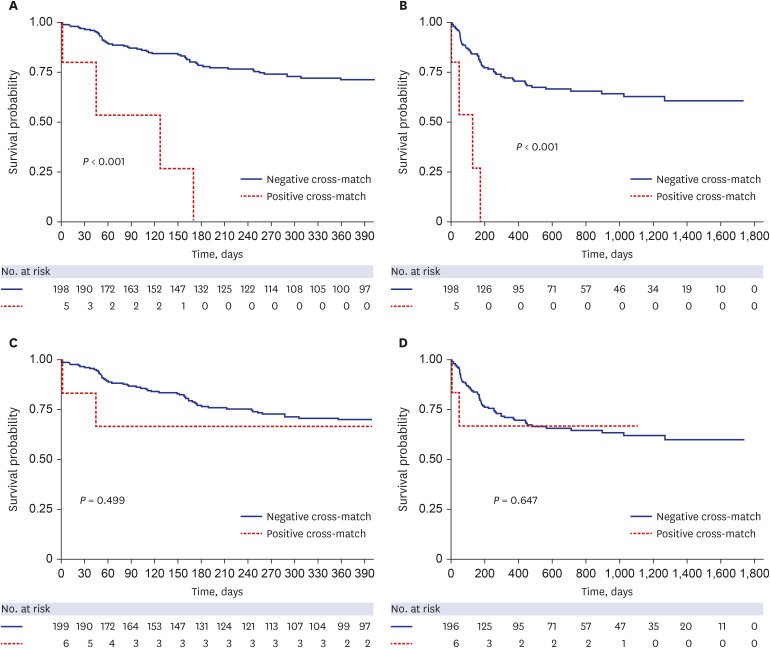 | Fig. 2Impact of positive CDC and flow crossmatches on survival of lung transplant patients. (A) The 1-year survival according to the results of CDC crossmatch. (B) Overall survival according to the results of CDC crossmatch. (C) The 1-year survival according to the results of flow cytometric crossmatch. (D) Overall survival according to the results of flow cytometric crossmatch.CDC = complement-dependent cytotoxicity.
|
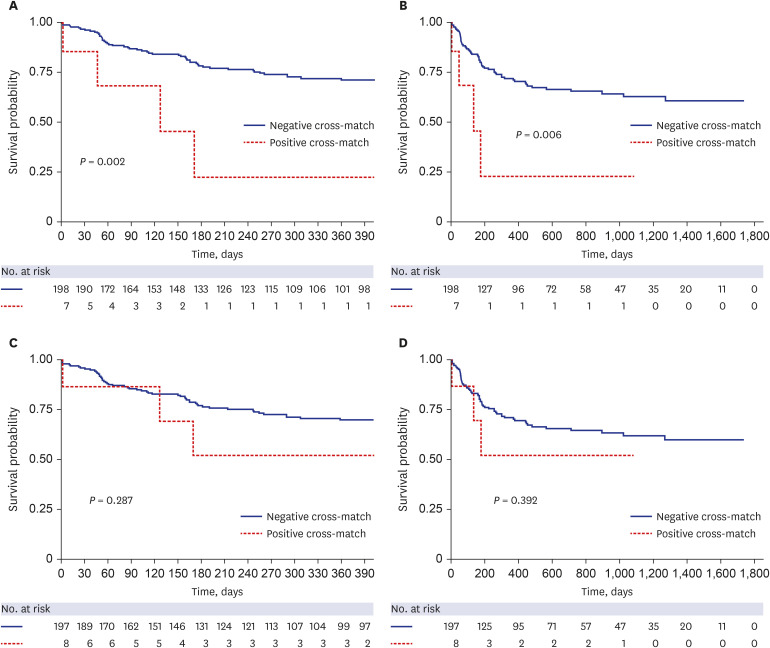 | Fig. 3Survival analysis of positive T and B lymphocyte crossmatches in lung transplantation. (A) The 1-year survival according to the results of T lymphocyte crossmatching. (B) Overall survival according to the results of T lymphocyte crossmatching. (C) The 1-year survival according to the results of B lymphocyte crossmatching. (D) Overall survival according to the results of B lymphocyte crossmatching.
|
Go to :
DISCUSSION
We conducted a multicenter nationwide study to analyze the prevalence of positive crossmatching and the outcomes of positively crossmatched patients in lung transplantation. Although the incidence of positive crossmatching was low (4.3%), positive CDC-XM and T lymphocyte crossmatching results were related to poor 1-year and overall survival.
It is controversial to consider HLA matching as an allocation factor. ISHLT introduced the lung allocation score (LAS) in 2005 and revised it in 2015 and 2020.22 The LAS includes factors related to waiting list mortality and post-transplant 1-year survival. HLA matching is not considered in the LAS system for several reasons. First, as lung transplantation is mostly performed under emergency settings, it is not always possible to conduct donor HLA typing prior to allocation. Furthermore, there is also a possibility of prolonging allograft ischemic time while waiting for crossmatching results.810 Brugière et al.23 analyzed the relative impact of mismatching and graft ischemic time; an allograft ischemic time of over 330 minutes worsened patient survival, even with well-matched donor and recipient pairs. Second, because of the shortage of possible donor organs and the extensive complexity of the HLA system, the probability of finding a matched recipient is extremely low.10 Furthermore, nonimmunologic factors are considered more important for 1-year survival. Early mortality resulting from the ischemia and reperfusion injury has been shown to decrease after introducing low-potassium dextran lung preservation solution.24 Advances in immunosuppressive regimens and enhanced combinations of antibiotics may also be responsible for improved unstable hemodynamics during the early post-transplant period.25 After alleviating these nonimmunological factors for early graft dysfunction and mortality in lung transplantation, the effect of HLA compatibility between the donor and recipient becomes more important for early outcomes. In addition, an improved methodology for HLA crossmatching has facilitated more accurate and rapid access to crossmatching results, leading to increased awareness of the importance of HLA crossmatching in lung transplantation.
Several studies analyzed the impact of HLA mismatching on lung transplantation. It is well known that HLA mismatching can trigger graft damage or even mortality.10 Donor HLA molecules are recognized by the immune system of the recipient. Immunogenetic discrepancies can lead to ACR and AMR, which play major roles in graft dysfunction and loss.
In 2003, the Eurotransplant Foundation analyzed 590 patients who underwent cadaveric lung transplantation between January 1997 and December 1999. In this study, patients with more than four mismatches of HLA loci showed poorer 1-year survival than the others.26 A retrospective study by the United Network for Organ Sharing/ISHLT also confirmed HLA mismatches as a risk factor for 1-year mortality in lung transplantation.27 As routine pretransplant crossmatching is not considered feasible in lung transplantation; these studies did not analyze prospective crossmatching; however, the results confirmed that HLA mismatching is related to graft dysfunction and survival.
In our study, the incidence of rejection or 1-year survival was not statistically different according to the crossmatching results. This result may be because of the low incidence of positive crossmatching in the cohort (4.3%) and the relatively short-term follow-up period of the positive group (median 129.0 vs. 386.5 days). Moreover, most centers involved in the registry tended to decline the allocation when positive crossmatching had been verified not only by the KODA lab but also by the center’s study. However, the relationship between 1-year survival and positive crossmatching was observed when the cohort was subdivided according to the crossmatching method.
Flow-XM is reportedly more sensitive for detecting anti-HLA antibodies than CDC-XM.28 Several studies have shown the relationship between positive flow-XM results and a higher risk of graft dysfunction and poor survival.237 However, as flow-XM is sometimes too sensitive, denying the allocation because of a positive flow crossmatch is still controversial.29 Moreover, flow-XM is not a functional test, and the binding of antibodies to lymphocytes may not always reflect complement system activation.6 Thus, transplantation across a positive flow crossmatch and negative CDC crossmatch is acceptable, whereas transplantation across a positive CDC result is not typically recommended. In our study, the Kaplan-Meier analysis also supported this principle. The patients with positive CDC crossmatch showed significantly lower 1-year and overall survival, whereas positive flow crossmatch did not significantly affect the outcome.
The impact of positive T cell crossmatches on poor graft outcomes was apparent in renal, cardiac, and liver transplantation.230 A negative lymphocytotoxic T cell result is generally considered as grounds to proceed with transplantation. Here, the results of Kaplan-Meier analysis also demonstrated significantly poor 1-year and overall survival in positive T-cell crossmatched patients, whereas positive B-cell crossmatching did not show a significant difference in graft survival. Positive T-cell crossmatching indicates the presence of DSAs against class I antigens, which can lead to antibody-mediated damages to the graft.378 This damage can cause hyperacute rejection or graft loss.
This study has certain limitations. First, although this study analyzed a nationwide cohort, this is a retrospective study with a relatively small number of patients and a short follow-up period. CLAD was not observed in the positively crossmatched patients, probably because of the short follow-up time (median 129.0 days). Thus, further follow-up for the CLAD is needed for the positive crossmath group. Second, the incidence of positive crossmatching was too low to perform further statistical analyses. As mentioned above, we performed regression analysis to identify the risk factors of poor survival, and positive CDC crossmatching was the only meaningful risk factor for poor 1-year survival. Third, a nationwide multicenter study with registry data does not reflect detailed information on each case. In particular, it is difficult to determine the actual immunologic consequences on graft survival.
In conclusion, this study analyzed the outcomes of positively crossmatched patients in lung transplantation and revealed the importance of crossmatching methods in lung transplantation using nationwide data. Positive results of CDC and T lymphocyte crossmatching may lead to devastating outcomes in lung transplantation. Although crossmatching is not part of the allocation system, the results of crossmatching should be considered with caution during postoperative management after lung transplantation.
Go to :
 XML Download
XML Download