

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The world is becoming increasingly interconnected and heavily dependent on the efficient functioning of the social infrastructure.123 Health issues in any corner of the world are no longer of local or regional concern; they may have global impact and are now subjected to global health analyses. As a prime example, the effective preventive measures and surveillance even in remote and geographically isolated areas may help avoid spread of infections and worsening ecology and improve global health.45
The term global health is relatively new. It implies the right to “improving health and achieving equity in health for all people” (introduced as a Medical Subject Heading [MeSH] term in 2015 [originally in 1978]; https://www.ncbi.nlm.nih.gov/mesh/?term=global+health). The definition of global health has been crystallized in historic declarations endorsed by the World Health Organization (WHO) as strategies for healthcare development in an increasingly interconnected and interdependent world.
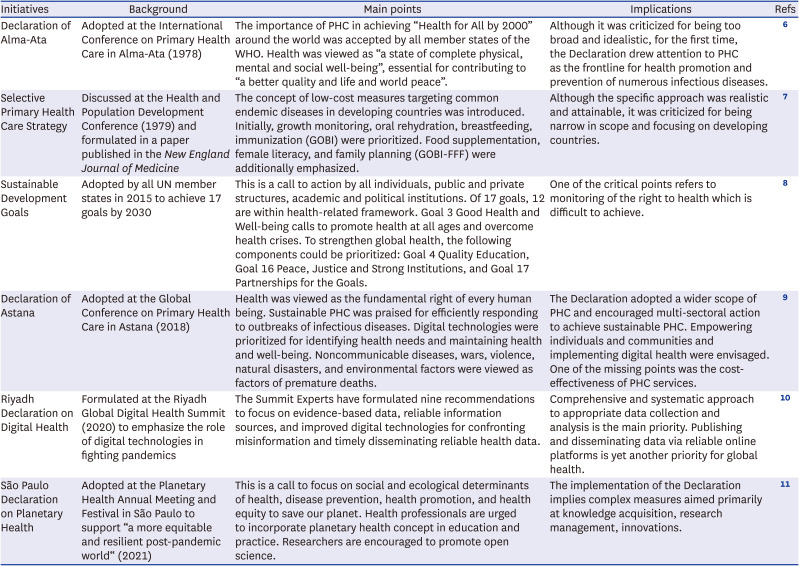
The aim of this article is to overview major initiatives and declarations and highlight essential strategies developed by public health experts and adopted at conferences of global importance in the last four decades. Increasing awareness of global health initiatives may enable enforcing strategies for improving health, well-being, and safety of all people facing unprecedented existential threats (Table 1).67891011
Table 1
Main declarations and initiatives in global health
| Initiatives | Background | Main points | Implications | Refs |
|---|---|---|---|---|
| Declaration of Alma-Ata | Adopted at the International Conference on Primary Health Care in Alma-Ata (1978) | The importance of PHC in achieving “Health for All by 2000” around the world was accepted by all member states of the WHO. Health was viewed as “a state of complete physical, mental and social well-being”, essential for contributing to “a better quality and life and world peace”. | Although it was criticized for being too broad and idealistic, for the first time, the Declaration drew attention to PHC as the frontline for health promotion and prevention of numerous infectious diseases. | 6 |
| Selective Primary Health Care Strategy | Discussed at the Health and Population Development Conference (1979) and formulated in a paper published in the New England Journal of Medicine | The concept of low-cost measures targeting common endemic diseases in developing countries was introduced. Initially, growth monitoring, oral rehydration, breastfeeding, immunization (GOBI) were prioritized. Food supplementation, female literacy, and family planning (GOBI-FFF) were additionally emphasized. | Although the specific approach was realistic and attainable, it was criticized for being narrow in scope and focusing on developing countries. | 7 |
| Sustainable Development Goals | Adopted by all UN member states in 2015 to achieve 17 goals by 2030 | This is a call to action by all individuals, public and private structures, academic and political institutions. Of 17 goals, 12 are within health-related framework. Goal 3 Good Health and Well-being calls to promote health at all ages and overcome health crises. To strengthen global health, the following components could be prioritized: Goal 4 Quality Education, Goal 16 Peace, Justice and Strong Institutions, and Goal 17 Partnerships for the Goals. | One of the critical points refers to monitoring of the right to health which is difficult to achieve. | 8 |
| Declaration of Astana | Adopted at the Global Conference on Primary Health Care in Astana (2018) | Health was viewed as the fundamental right of every human being. Sustainable PHC was praised for efficiently responding to outbreaks of infectious diseases. Digital technologies were prioritized for identifying health needs and maintaining health and well-being. Noncommunicable diseases, wars, violence, natural disasters, and environmental factors were viewed as factors of premature deaths. | The Declaration adopted a wider scope of PHC and encouraged multi-sectoral action to achieve sustainable PHC. Empowering individuals and communities and implementing digital health were envisaged. One of the missing points was the cost-effectiveness of PHC services. | 9 |
| Riyadh Declaration on Digital Health | Formulated at the Riyadh Global Digital Health Summit (2020) to emphasize the role of digital technologies in fighting pandemics | The Summit Experts have formulated nine recommendations to focus on evidence-based data, reliable information sources, and improved digital technologies for confronting misinformation and timely disseminating reliable health data. | Comprehensive and systematic approach to appropriate data collection and analysis is the main priority. Publishing and disseminating data via reliable online platforms is yet another priority for global health. | 10 |
| São Paulo Declaration on Planetary Health | Adopted at the Planetary Health Annual Meeting and Festival in São Paulo to support “a more equitable and resilient post-pandemic world“ (2021) | This is a call to focus on social and ecological determinants of health, disease prevention, health promotion, and health equity to save our planet. Health professionals are urged to incorporate planetary health concept in education and practice. Researchers are encouraged to promote open science. | The implementation of the Declaration implies complex measures aimed primarily at knowledge acquisition, research management, innovations. | 11 |
EQUITY IN HEALTH FOR ALL
The landmark 1978 Alma-Ata Declaration on primary health care (PHC) laid the foundations for exploring major health problems at the level of PHC and for ensuring social justice by providing universal access to essential health services.6 The main idea of the Alma-Ata Declaration was to utilize the prevailing concept of health as a state of complete physical, mental, and social wellbeing, and not just absence of a disease. The Declaration placed economic and social determinants of health at the core of the PHC development strategies.12 Several directions, including health promotion and education, food supply and nutrition, and immunization against major infections, were prioritized in the Alma-Ata Declaration and revisited in subsequent PHC development plans.13 At the height of the East-West confrontation in the 1970s, the then proposed “Health for All” plan was achievable with improved use of the world resources in peaceful conditions.6 Despite its idealistic and non-specific statements, opposed by the Selective PHC initiative of the Rockefeller Foundation in 1979,7 the Alma-Ata Declaration influenced PHC reforms across most developing countries and introduced the principle of improved quality of life achievable through intersectoral cooperation in peaceful conditions.1415
The Sustainable Development Goals (SDGs), a more ambitious and comprehensive plan was approved by all UN member states in 2015 as a call to joint efforts to “end poverty, protect the planet and improve the lives and prospects of everyone, everywhere by 2030”.8 The importance of the SDGs is reflected in a relevant MeSH keyword (introduced in 2019; https://www.ncbi.nlm.nih.gov/mesh/?term=sustainable+development). Notably, relevant research documents fulfilling the Goals are mapped by the Scopus database from 2021 onward.16 Goal 3 specifically covers health-related strategy. It is criticized by experts for uncertainties of the right to health and its monitoring.17 At the same time, the health-related sustainable development framework is accompanied by certain targets and indicators which can be monitored to proportionately allocate funds.18
In 2018, the WHO organized yet another conference in Astana, Kazakhstan to celebrate the 40 years of the Alma-Ata PHC Conference, overview the implications of the Alma-Ata Declaration, and explore new directions of health reforms.19 The 2018 Astana Declaration reiterated the global importance of PHC services, particularly for physical and mental health promotion and drug manufacturing and marketing regulation.2021 The PHC system satisfying the upgrading quality, safety, and accessibility standards was considered the frontline for fighting epidemics of infectious diseases such as tuberculosis and malaria and for organizing effective vaccination campaigns.22 The Astana Declaration was praised as the driver for the efficient use of public and private funds to increase health services’ quality and value, overlooked in the Alma-Ata document.2324 It was also viewed as the catalyst in the process of fulfilling the SDGs, particularly Goal 3.25 The renewed global interest toward PHC services coincided with the fast-expanding cross-country and multi-sectoral cooperation in a digitized and technologically advanced world. The Astana Declaration considered the health of people across developing and developed countries as a guarantor for peace, safety, and socioeconomic development, and not vice versa.9 The global crises, particularly the coronavirus disease 2019 (COVID-19) pandemic that followed the Astana Conference, put the adopted Declaration to the test.26
EVIDENCE FOR ACTION AND FURTHER RESEARCH
The principles of health justice which were initially adopted in the Alma-Ata Declaration, implied multi-sectoral cooperation, community involvement, employment of modernized technologies, and universal health services’ coverage.27 While the rationale for global action in this field is justifiable from the social point of view, uncertainties and discrepancies of related evidence-based studies have long frustrated healthcare decision-makers. Therefore, empowering researchers in developing countries and guiding them to conduct practice-oriented research have been emphasized.27
Traditionally, scientifically-sound and socially-acceptable health services have been based on research in developed countries with supposedly high ethical and reporting standards. Well-funded and high-quality research studies have built the traditional evidence pyramid that shaped modern medicine and public health. Over the past two decades, systematic reviews and randomized controlled studies with strict inclusion criteria and homogenous samples have been viewed as the top studies in the pyramid hierarchy. Variable quality meta-analyses and trials have been contributing to practice guidelines with immediate healthcare and societal impacts. Nonetheless, methodological limitations, inconsistencies, inclusion and exclusion biases, and other quality issues of some top studies have prompted the revision of the concept and placed lower evidence categories such as real-life observations, case series, and expert views closer to the top of the pyramid.282930
The revision of the hierarchy of evidence-based studies, initiated in the pre-pandemic era, became an urgent necessity in the early months of the COVID-19 pandemic. The lack of randomized clinical trials and relevant meta-analyses of COVID-19 primary research had prompted to search for and to rely on real-world heterogeneous cohorts, descriptive clinical reports, and individual case studies (Fig. 1).
Fig. 1
Revision of the hierarchy of evidence-based studies in view of their availability and quality as well as weight of bibliometric and altmetric values. The evidence pyramid can be accompanied by the reversed metrics pyramid. The lines between different categories of studies and metrics are blurred, pointing to their flexible placement.
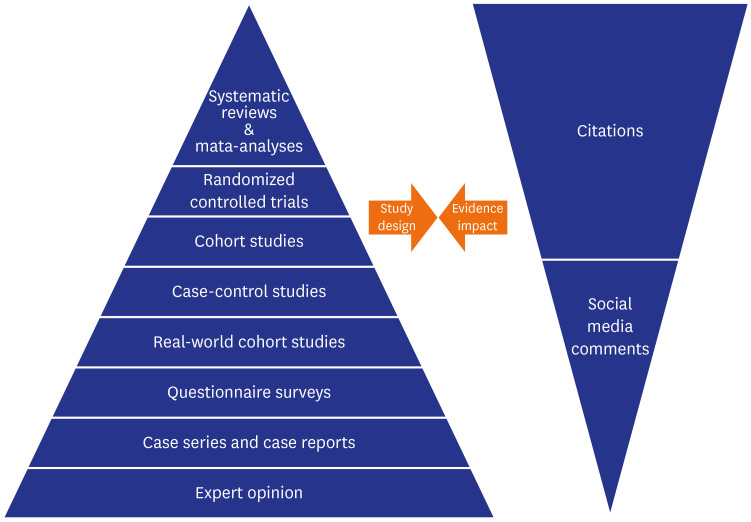
The reports of mixed (heterogeneous) cohorts, case series, and historic evidence of previous coronavirus epidemics had contributed to the emergency, or so-called rapid practice guidelines on COVID-19 diagnosis and treatment.31 Some of the COVID-19 rapid guidelines were harshly criticized because of the hasty and soft integrity checks and reliance on non-scientific and politically-motivated approaches.32 The scientific prestige of publication sources that hastily processed and accepted variable-quality COVID-19 reports and subsequently attracted numerous citations and alternative metrics inadvertently placed some COVID-19 reports in the most influential medical journals at the top of the evidence hierarchy in the field.33 Such an “evidence-based” approach resulted in dire global implications when the reports of hydroxychloroquine therapy lacking data veracity appeared in the top medical journals, attracted numerous citations and social media comments, and flawed the evidence synthesis for COVID-19 emergency practice recommendations.34
The COVID-19 pandemic has prompted the global interest toward online surveys which could provide analytical data on specialists’ and patients’ knowledge and perceptions of the disease and related vaccination campaigns. The ease of surveying and obtaining responses via numerous scholarly networking channels and the convenience sampling have made online surveys the most frequently employed studies with a potential to test a wide range of hypotheses and produce preliminary evidence.35 The increasing number of surveys during the pandemic may place these observational studies closer to the top of the evidence pyramid in the field of COVID-19. Fortunately, numerous successful surveys have explored the global preparedness and efficiency of COVID-19 vaccination and influenced relevant health policies worldwide.363738
Statistical yearbooks and national morbidity and mortality reports have long been sources for information-analytical studies in global health. The unified and dynamic data recording for long periods (years and decades), covering major disease groups, reflecting on resource allocation and population health across numerous geographic locations are some of the advantages of such studies.39 The described health trends in information-analytical studies may help generate new hypotheses for further research. Limitations include, amongst others, the lack of risk exposure-outcome analyses and oversight of rare diseases and specific clinical conditions.4041 Despite some limitations and difficulties with comprehensive coverage of population health in times of crises, statistical yearbooks have already been used in COVID-19 reports to reveal healthcare systems’ preparedness for coronavirus outbreaks and to plan emergency measures.424344
TECHNOLOGY ADVANCES AND INFORMATION DISSEMINATION
The past four decades have been marked with technological advances and digitization in healthcare worldwide. The Astana Declaration reaffirmed the role of information systems in improving health-related data recording, surveillance, and monitoring. Advanced digital technologies are employed for identifying health needs and monitoring individuals’ and communities’ wellbeing.9 Accordingly, synthesizing and disseminating reliable information, improving digital literacy, and ensuring trust in scientific information remain the main issues in global health.45
Digitization has brought about numerous online journals, search engines, databases, blogs, and social-media channels with diverse fact-checking and moderating models. The searches through well-organized databases and official sites are now often employed by skilled users (researchers) who seek reliable health information.46 While the most prestigious databases such as MEDLINE and Scopus are curated by expert librarians and health professionals, most online platforms, blogs, and social-media channels, including Twitter and Facebook, lack strict moderating tools.4748 The loopholes in the online systems are often abused by generators of misinformation and uncertain ideas.4950
The adverse impact of misinformation, or infodemic, is amply illustrated during the COVID-19 pandemic, when poorly checked reports and pseudoscientific posts on COVID-19 management and vaccination infiltrate online platforms, causing panic and irrational public actions.515253 Advancing online users’ digital literacy, learning techniques to spot fake news, and organizing online professional groups for sharing evidence-based data could be a solution in the ongoing pandemic.5455 Importantly, the Riyadh Declaration on Digital Health was adopted by global health experts in 2020 to improve digital health infrastructure, educate healthcare specialists to process information, and combat misinformation.10
MULTI-SECTORAL ACTION
The Alma-Ata Declaration, the SDGs, and the Astana Declaration have all pointed to multi-sectoral action as a requirement for implementing a “Health for All” approach.689 The Astana Declaration stressed the role of multi-sectoral action and involvement of more stakeholders in empowering communities and providing PHC services in emergencies, particularly in resource-limited developing countries.9 The specifics of multi-sectoral action in developing countries with poor research infrastructure and lack of funding have been widely debated.56 Private and public institutions in developing countries disproportionately share responsibilities for education, social services, transport and communications, sanitation, and safety. Joint actions across all these fields may transform into health-related sustainable development.57 With growing health inequalities, separate policies for multi-sectoral action are justified for rural and urban communities.58
The role of multi-sectoral action, international cooperation, and coordination has proved essential in the COVID-19 pandemic, particularly for resolving emerging mental and physical health issues in a timely manner.59 Country-based examples of successfully battling COVID-19 outbreaks in Switzerland, Georgia, and New Zealand have underscored the importance of improving health literacy and targeting vulnerable population groups.60 Sustained research, academic collaborations, and transparent reporting have also been prioritized for minimizing harm in the face of the unprecedented global crisis.61 Finally, numerous reports have demonstrated the need for implementing telehealth at the PHC level to mobilize medical personnel, communicate with patients, and respond to their mental and physical health needs.626364
GLOBAL THREATS AND UNRESOLVED ISSUES
The Astana Declaration urged all stakeholders to act immediately to avoid losing lives because of violence, epidemics, natural disasters, and other global threats.9 In line with the Declaration, stakeholders who commit to bold political choices and sustainable PHC may achieve global health goals.9 While the good intentions are understandable, social and economic developments in the period after 2018 have pointed to global inconsistencies and raised concerns over the Sustainable Development prospects. Notably, evidence from Wuhan, China suggested that PHC facilities in the early months of the COVID-19 pandemic successfully assisted in tracing contacts, screening for high-risk individuals, enabling epidemiological investigation, and quarantining patients.65 At the same time, Iranian PHC encountered decreased essential services and heath personnel shortages, negatively affecting customer satisfaction.66
Further evidence has pointed to the PHC strain elsewhere in the world with a decrease of PHC services for cancer patients and individuals seeking sexual, reproductive, and maternal health services during the pandemic.6768 Psychological, socioeconomic, and other issues have all resulted in the rise of violence that further stretched the PHC workforce and resources in the past two years.6970 The strained PHC facilities, particularly in developing countries and regions affected by mass violence, have failed to maintain the quality of care and provision of basic preventive services such as COVID-19 vaccination.717273
In the face of the COVID-19 pandemic, unprecedented crises, and emerging existential threats, the São Paulo Declaration on Planetary Health was adopted in 2021 to call all stakeholders to focus on social and ecological determinants of health and support “a more equitable and resilient post-pandemic world”.11 Improving individual health, preserving ecology, and embracing digital technologies are warranted for safer and healthier future of our planet. The success of the Declaration enforcement is believed to be dependent on improved knowledge acquisition and innovative research management.74
THE MOVE FORWARD
Global health declarations and initiatives, influenced by accumulated experience and evidence, are aimed at implementing efficient action plans and driving a continuum of healthcare strategies (Fig. 2).

Over the past half a century, several seminal documents have been drafted to reflect health priorities and highlight urgent actions by all stakeholders (Table 1). The Alma-Ata and Astana Declarations positioned PHC at the frontline for combating most healthcare issues and categorized health and well-being as the basic human right. Both documents were helpful for uniting efforts of health specialists across the world, particularly in the time of the digitization and emergence of telehealth. The Astana Declaration turned out an ambitious strategic document that supported the health component of the SDGs to make the globalized and digitized world healthier and safer.
As in all declarative documents, specifics of actions to achieve goals are missing in both the Alma-Ata and Astana Declarations. The implementation of the Astana Declaration is strongly influenced by the Internet, making the increased awareness of health issues by individuals and communities the main global issue at the current stage. Overall, digital health strategies may contribute to the much-desired comprehensiveness and continuity in healthcare by revealing health needs and value-based measures.75
The surveys exploring the awareness gaps among specialists and patients have become important tools for digital health. Better organizing people involved in surveys by launching online groups on social media and supplying them with evidence-based and easily-understandable materials such as infographics seem useful strategies at all healthcare levels.7677 Of all social-media platforms, Twitter is perhaps the most promising channel for understanding the societal impact of health initiatives, disseminating reliable information, and positively influencing global health.787980 The main challenge, however, is the disproportionate use of Twitter and other social-media platforms across countries, making it difficult to achieve the same results by promoting health initiatives globally. The issue is complicated further by abuses of social media to promote misinformation and manipulate public opinion for non-medical purposes.81
The COVID-19 pandemic has introduced a responsible approach to disseminating information via social-media channels.82 In the time of the crisis, engaging different stakeholders in online communication and providing them with verified scientific facts are raised to the level of professional competency.83 Engaging social-media posts responsibly generated by skilled users are now increasingly used to fulfil the UN Sustainable Development Goals.84 And in line with this, highly-skilled social media editors are complementing decision-making journal editors to select potentially influential contents and ethically promote them.
To sum up, with increased awareness of health declarations and initiatives, their action points, and emerging global threats, it is the right time to engage health professionals with advanced digital skills in health communications and to explore the best models of healthcare in the globalized and digitized world.
 XML Download
XML Download