

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Healthcare workers (HCWs) are at higher risk of Mycobacterium tuberculosis infection due to their risk of occupational exposure to patients with active pulmonary tuberculosis (TB). A high prevalence of latent TB infection (LTBI) among HCWs is an obstacle for TB elimination.12 Although there were several controversies including cost-effectiveness,34 TB screening and preventive therapy among HCWs have been regularly conducted in various settings. The recent World Health Organization (WHO) guideline states that systematic LTBI testing and treatment are considered for HCWs based on local TB epidemiology, healthcare infrastructure, and overall health priorities in countries with both high and low TB prevalence.56
Korea, an intermediate TB burden country, has the highest TB incidence among high-income countries. Despite recent nationwide decrement of TB incidence, TB outbreaks in the neonatal intensive care unit and postpartum care center became social issues.78910 Thus, the Korean government revised the TB Prevention Act to require TB examination for employees in the medical institutions in 2016.1112 Since 2017, screening and treatment of TB infection have become mandatory for HCWs.
TB preventive therapy (TPT) is one of the core interventions for TB elimination. However, its lengthy treatment duration and risk of potential hepatotoxicity reduce uptake, acceptance, and completion of therapy, which are the major obstacles to scale up the programmatic LTBI management.13 Korean government implemented a nationwide LTBI screening among HCWs with a strong political will, however, its performance has not been properly evaluated. Hereafter, we aimed to assess each step of programmatic LTBI management in HCWs using the cascade of care model.
METHODS
Study design and data source
We constructed a prospective observational cohort study14 based on data that were systematically collected from participants of the nationwide screening project for LTBI in congregate settings who underwent interferon-gamma release assay (IGRA) between March 2017 and December 2018 in Korea.15 In order to generate a ‘TB FREE COREA (latent TuBerculosis inFection scREEning and treatment in COngREgAte settings)’ database, we used and cross-linked four databases: the LTBI screening database from the government program, the national health information database, the public healthcare information system database, and the national TB surveillance system.14 Anonymised joint keys, which are replacements for personal identification numbers, were used to link the LTBI screening database with the other three databases through deterministic matching.
Study setting and participants
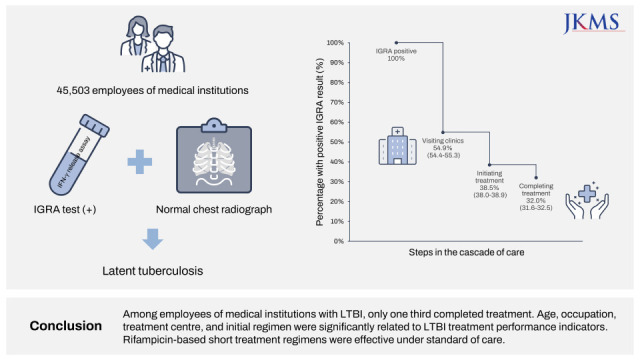
Employees of hospitals and healthcare centers were enrolled for our study. Major types of occupations were doctors, nurses, nurse assistance, radiology technologists, laboratory technologists, and physiotherapists. Other occupations included paramedics, clerical staffs, and food service workers. The eligibility criteria included: 1) having undergone IGRA and 2) absence of a prior TB treatment history. Those who received TPT previously because of close contacts with infectious TB patient were excluded. Among 294,131 people who had LTBI test, 284,077 participants had screened with IGRA test (Supplementary Fig. 1). Of them, 45,503 (16.0%) participants with positive IGRA result were enrolled in this study.
Systematic TB and LTBI screening process
IGRA was performed using QuantiFERON-TB Gold In-Tube (Qiagen, Hilden, Germany) and the results were interpreted according to the manufacturer’s instructions. Those with positive IGRA results received free LTBI screening and treatment from the government. On visiting a treatment center, they were clinically assessed and underwent chest radiography according to the national TB guideline. After the exclusion of active TB infection, TPT was offered.
LTBI cascade of care
The specific outcomes of interest were: 1) the number of participants with positive IGRA results, who visited clinic to initiate further LTBI management, 2) the number who those in whom TPT were initiated, and 3) the number of participants who completed treatment. Each step in the cascade of care were identified using the national health information database. We identified individuals who visited clinics for further care if they had a code of R76.80 (latent TB), based on the seventh edition of the Korean Classification of Disease. Performance of chest radiography between visiting clinics and initiating treatment was identified in the claims data. Three types of TPT regimens were recommend based on the Korean guideline: isoniazid (INH) monotherapy for 9 months (9INH), rifampin (RIF) monotherapy for 4 months (4RIF), and INH and RIF combination therapy for 3 months (3HR).16 We defined individuals as being under TPT if they were prescribed INH, RIF or a combination of INH and RIF with a R76.80 code. Individuals were considered to have completed the treatment course if they were prescribed more than 80% of the total dose within 12 months for INH therapy, 6 months for RIF therapy or 4 months for INH and RIF combination therapy.1718 “Still-on-treatment” was defined when the treatment completion date calculated according to the regimen was on or after January 1, 2020. Individuals with active TB disease before and during TPT were identified using the national TB surveillance system and were excluded from the appropriate stages.
Independent variables
We collected data on factors that may influence the LTBI cascade of care, such as sex, age, income level, place of residence, comorbidities, treatment center, and initial treatment regimen from a cross-linked database. Income level was described using ventiles, with each income ventile comprising 5% of the population, and was then categorised into four groups: low (ventiles 1 to 5), lower-middle (6 to 10), upper-middle (11 to 15) and high (16 to 20). Medicaid subscribers were added as a low-income titer. Place of residence was categorised into: rural area, small to medium-sized city and metropolitan city. The Charlson comorbidity index, assigned based on the severity of each disease, was used to measure comorbidity degree.19 Treatment center that individuals with positive IGRA results initially visited for LTBI management were categorised into public health centers and private hospitals. The implications of each independent variable and its data source has been described in the Supplementary Table 1.
Statistical analyses
Discrete variables are presented as frequencies and percentages. Periods of each step in the cascade of care were calculated and presented as median and range. We determined the relationship between our exposures of interest and a priori determined three specific outcomes of interest—i.e., ‘not-visiting clinic for further care,’ ‘not-initiating treatment,’ and ‘not-completing treatment.’ We used the multivariable Poisson regression with a robust variance estimator to estimate the relative risk (SAS proc genmod/R package geepack). Multivariable analysis was adjusted by sex, age, place of residence, income level, Charlson comorbidity index, and types of occupation. Unknown data were regarded as missing values. Statistical analyses were conducted with R v.3.5.2 (R Foundation for Statistical Computing, Vienna, Austria) and SAS statistical software (version 9.4; SAS Institute, Cary, NC, USA).
In the model for analysis of factors associated with ‘not-completing treatment,’ we calculated stratum-specific relative risk to evaluate interaction between treatment center and initial regimen on ‘not-completing treatment.’ We combined variables of treatment center and initial regimen into a single variable and chose 3HR at the private hospitals as the reference group, because this combination is the most effective.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board (IRB) of Incheon St. Mary’s Hospital, The Catholic University of Korea approved the study protocol (IRB No. OC19ZESE0023) and waived the need for informed consent as none of the patients were at risk.
RESULTS
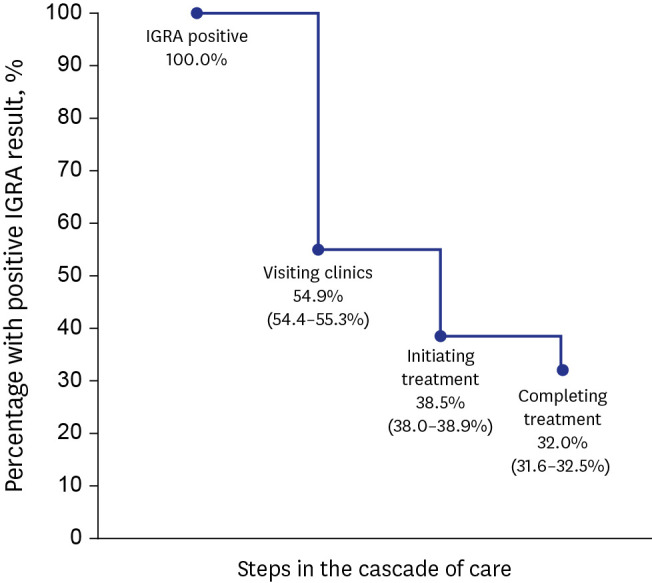
Among participants with positive IGRA result, 32,048 (70.4%) were female and 26,253 (57.7%) were less than 50 years (Table 1). Nurse (28.5%) was the most common type of occupation. Among participants with positive IGRA result, 24,962/45,503 (54.9%) visited clinics for further care (Fig. 1). Of them, 17,947 (70.2%) visited private hospital. After excluding 18 patients with concurrent active TB during initial assessment, 17,500/45,485 (38.5%) of the enrolled participants initiated LTBI treatment. Of them, 3HR (80.3%) was the most frequently prescribed regimen. After excluding seven patients who developed active TB after initiation, 14,572/45,478 (32.0%) completed treatment.
Table 1
Baseline characteristics of enrolled 45,503 participants with positive result of interferon-gamma release assay
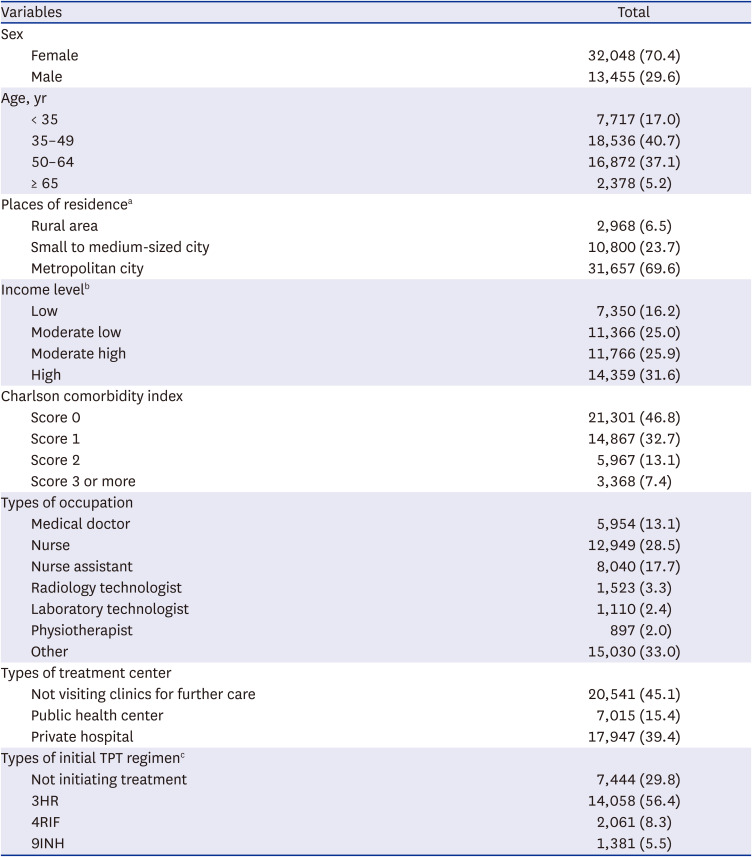
Data were expressed as number and percentage.
TPT = tuberculosis preventive therapy, 3HR = 3 months of rifampin and isoniazid combination therapy, 4RIF = 4 months of rifampin monotherapy, 9INH = 9 months of isoniazid monotherapy.
aNumber of missing value was 78.
bNumber of missing value was 662.
cDenominator was total number of candidates of LTBI treatment which was 24,944.
Fig. 1
Losses and drop-outs at each stage of the latent TB cascade of care among all enrolled participants with positive result of IGRA.
Eligible participants for the first step, visiting clinics for further care, are all participants with positive IGRA results. Eligible participants for the second step, initiating treatment, are participants with positive IGRA result, who did not have concurrent active TB. Eligible participants for the third step, completing treatment, are participants with positive IGRA result, who did not have concurrent active TB and who did not develop active TB during TB preventive therapy. The 95% confidence interval of proportions were calculated using the Wilson procedure without a correction for continuity.
IGRA = interferon-gamma release assay, TB = tuberculosis.
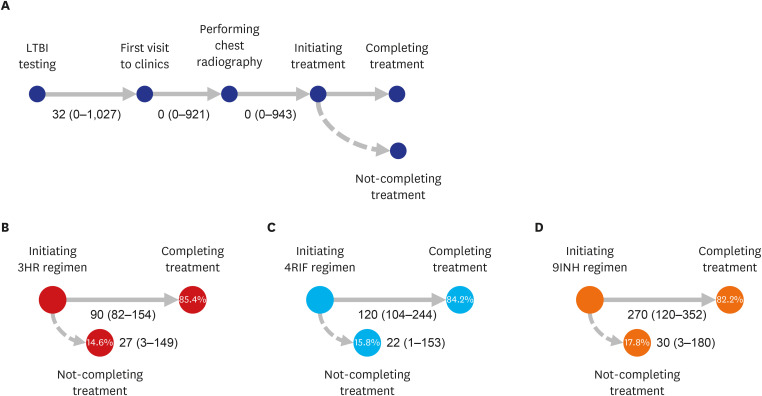
The period taken between LTBI testing and visiting clinics for further care was a median of 32 days (range 0–1,027) (Fig. 2). All the participants who visited clinics had chest radiography performed within a median of 0 day (range 0–921) after visiting clinics. Among the 24,944 participants who were candidates of TPT, 17,500 (70.2%) initiated treatment within a median of 0 day (range 0–943) after undergoing chest radiography. Among 17,493 participants who initiated treatment without developing active TB, the overall proportions of completing treatment, not-completing treatment, and still-on treatment were 83.3%, 14.7%, and 2.0%, respectively. The median times between treatment initiation and not-completing treatment among 3HR, 4RIF, and 9INH were 27, 22, and 30 days, respectively.
Fig. 2
Intervals of days at each stage of cascade of care in LTBI. (A) Intervals from LTBI testing to initiating tuberculosis preventive therapy, (B) Intervals from initiating treatment to completing and non-completing treatment for 3HR, (C) for 4RIF, and (D) for 9INH.
Data were expressed as mean and lowest and highest values. Numbers in circles indicated proportions of completing and non-completing treatment for each regimen.
LTBI = latent tuberculosis infection, 9INH = 9-month isoniazid monotherapy, 4RIF = 4-month rifampin monotherapy, 3HR = 3-month rifampin and isoniazid combination therapy.
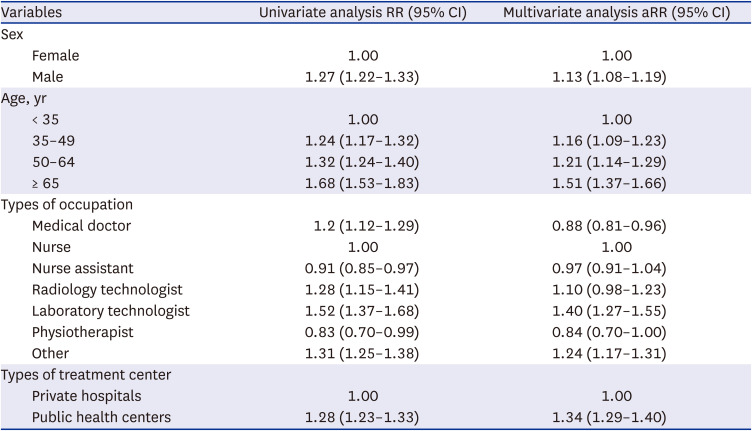
Compared to young age < 35 years, older age ≥ 65 years was associated with not-visiting clinics (adjusted relative risk [aRR], 1.47; 95% confidence interval [CI], 1.40–1.55) and not-initiating treatment (aRR, 1.47; 95% CI, 1.40–1.55) in multivariable analysis (Tables 2 and 3). Compared to nurse, doctor (aRR, 1.23; 95% CI, 1.18–1.28) was less likely to visit clinics, however, was more likely to initiate treatment (aRR, 0.88; 95% CI, 0.81–0.96). Those visited public health centers (aRR, 1.34; 95% CI, 1.29–1.40) were associated with not-initiating treatment.
Table 2
Multivariate analysis of factors for not-visiting clinics for further care among participants with positive result of interferon-gamma release assay
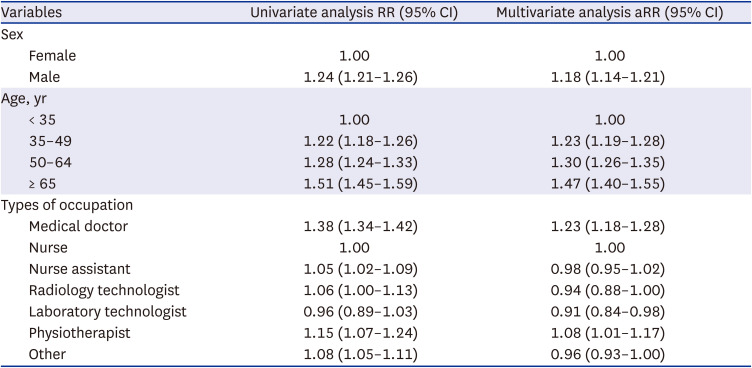
Table 3
Multivariate analysis of factors for not-initiating treatment among participants who were candidates of latent tuberculosis infection treatment
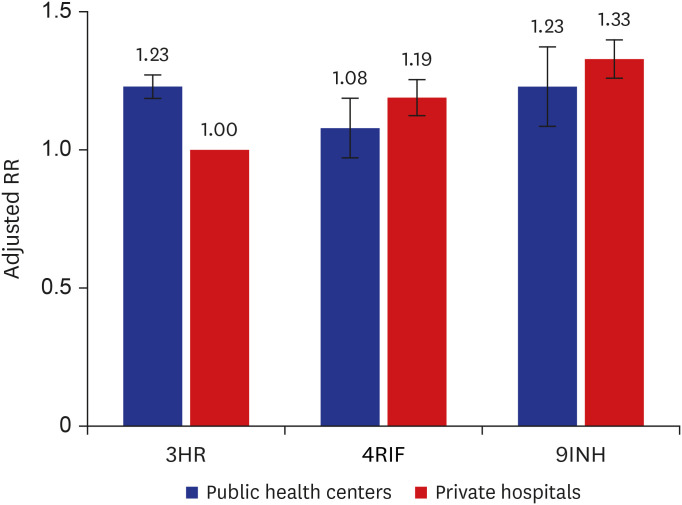
In multivariable analysis, those who visited public health center (aRR, 1.17; 95% CI, 1.08–1.26) was associated with not-completing treatment (Table 4). Compared to 3HR, 9INH (aRR, 1.25; 95% CI, 1.10–1.41) was associated with not-completing treatment. Compared to nurse, radiology technologist was less likely to complete treatment (aRR, 1.40; 95% CI, 1.15–1.70). Compared to 3HR at the private hospitals, 9INH at the private hospitals (aRR, 1.33; 95% CI, 1.16–1.53) and 3HR at the public health center (aRR, 1.23; 95% CI, 1.13–1.34) had higher risks of not-completing treatment (Fig. 3 and Supplementary Table 2).
Table 4
Multivariate analysis of factors for not-completing treatment among participants whose treatment outcome was reported
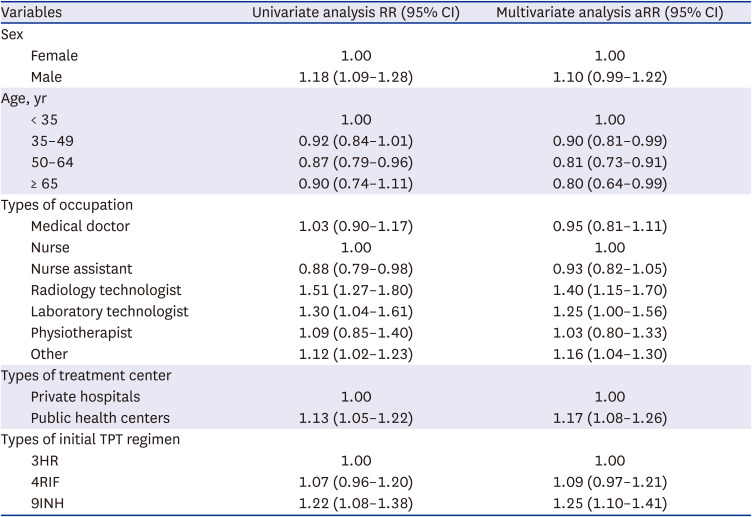
Multivariate analysis was adjusted by sex, age, place of residence, income level, Charlson comorbidity index, types of occupation, types of treatment center, and types of initial TPT regimen.
RR = relative risk, aRR = adjusted relative risk, CI = confidence interval, TPT = tuberculosis preventive therapy, 3HR = 3 months of isoniazid and rifampin combination therapy, 4RIF = 4 months of rifampin monotherapy, 9INH = 9 months of isoniazid monotherapy.
Fig. 3
Barplots presenting stratum-specific RR of not-completing treatment and effect of interaction between types of treatment center and initial treatment regimen.
Multivariate analysis was adjusted by sex, age, place of residence, income level, and Charlson comorbidity index, types of treatment center, and types of initial regimen. The RR (Y axis) was calculated with reference of 3HR ate the private hospital. The error bar represents standard error of each RR.
RR = relative risk, 9INH = 9-month of isoniazid monotherapy, 4RIF = 4-month of rifampin monotherapy, 3HR = 3-month of rifampin and isoniazid combination therapy.
DISCUSSION
To the best of our knowledge, this is the first and largest to evaluate LTBI management among the entire HCW population in a single country. The current study evaluated the nationwide LTBI project using the cascade of care model to identify patient retention across the sequential stages of care required for achieving successful outcomes.20 Only about one third of participants eligible for LTBI treatment were able to complete all the stages, which was lower than anticipated. Other hospital-based studies during the same period in Korea reported various rates of completing LTBI treatment from 7.8% to 71.7%.2122232425 To maximize the impact of LTBI project, we need identify and evaluate the largest gaps its associated factors.
In our study, the largest gap of participant loss was not-visiting clinics for initial assessment of TB infection, which are consistent with findings from other settings.1326 One of the key factors associated with not-visiting clinics was age. Increasing age was also associated with not-initiating treatment. The current guidelines do not offer definite recommendation for TPT in patient aged ≥ 65 years, because of low evidence of its role to prevent active TB and high risks of adverse drug reaction, such as hepatotoxicity. However, the WHO’s End TB strategy prioritizes TPT among persons at high risk. Its expansion of target population including elderly aged ≥ 65 years is also highlighted.27 Similar to recent evidence supporting safety and tolerability of LTBI treatment among elderly population,282930 our study revealed that treatment completion rates tended to increase with increasing age. To increase engagement of LTBI care among elderly populations, strengthening of LTBI education programmes for HCWs should be considered.
The completion rates of each stage from visiting clinics for further care to completing treatment were differed according to types of occupation in our study. Overall completing rate of LTBI care and treatment was the highest for nurses and nurse assistants. Despite high proportions of initiating and completing treatment, doctors had the lowest proportion of visiting clinics, which are similar to previous studies.3132 The doctors’ busier schedules might have contributed to the lower outpatient clinic visit rate. In contrast, doctors are likely more knowledgeable about LTBI than other HCWs, which might have led to a relatively higher acceptance rate of treatment. Because we did not have additional information on whether medical institutions have high exposure to TB, or whether HCWs work in TB-related departments, it was difficult to determine causes of different participation rates by types of occupation. It is necessary to consider different strategies of TB screening and preventive therapy according to degree of TB exposures. For examples, proactive testing and treatment for LTBI would be beneficial to any HCWs who works in departments of pulmonology and infectious diseases, bronchoscopy unit, spirometry unit, and mycobacterial laboratory.
In our study, those who visited public health centers were less likely to start and complete LTBI treatment, compared to those who visited private hospitals. The major difference between public health centers and private hospitals in Korea is a doctor who oversees TB treatment. Specialists of respiratory medicine are in charge of TPT at private hospitals, whereas public health officers, who are mostly primary care physicians, are responsible for LTBI treatment. Thus, private hospitals are more aptly to provide standard of care regarding TB infection. Most of public health officers are busy to deal with other primary healthcare services and administrative works, and lack of expert knowledge and interest of TB infection. Although the Korean government offered a LTBI education to provide information on LTBI guidance before implementation,12 public health officers might not understand importance of TPT or have difficulties to manage adverse events during treatment, which hinder them to start and complete TPT. It is important to assess and understand physician’s hardship regarding to LTBI and identify challenges in clinical practice. The recent qualitative study which explored views of Australian TB physicians on LTBI treatment revealed complexities of communicating about LTBI with patients and making clinical decisions.33 Further research is necessary to fill these gaps to improve LTBI engagement.
Using the large real-world data, we described patterns and efficiency of LTBI treatment regimens. The most frequently prescribed regimen was the 3HR, which are supported by the WHO’s guideline. 9INH was offered to less than 10% of eligible participants and more likely not to complete treatment, which might be ascribed to its lengthy treatment duration.34 Overall treatment completion rates were similar between 3HR and 4RIF. RIF-containing preventive therapy is widely used in the TB programs owning to high completion rates and safety profiles with comparable efficacy.3536 Among those who received 3HR, public health center was more likely associated with not-completing treatment, compared to private hospital. In the public health centers, primary care physicians might not properly manage flu-like symptoms, which are major adverse event of RIF-based therapy.24 The most frequent timing of stopping LTBI treatment was within about one month after starting treatment in our study. These phenomena could be related to incidence of adverse events during the early phase of LTBI treatment. Stratified approach based on risk factors of adverse events would be beneficial during TPT. In addition, preparation of guidance on adverse event management, such as monitoring schedule, are necessary.
Compared with other general populations requiring LTBI screening, HCWs in our study shared similar factors related to acceptance and completion of LTBI treatment. For example, male and increasing age were associated with not-initiating treatment. Pease et al.37 reported that older age was associated with not-initiating treatment among Inuit in Canada, which was ascribed to increasing risk of adverse events, such as hepatotoxicity. Park et al.38 showed that female was prone to initiate treatment among Korean close contacts of active pulmonary TB patients, because they were more concerned about having an infection. The most important determinant of completing treatment was type of LTBI treatment regimen. Compared to INH monotherapy, shorter regimen composed of RIF was associated with higher completion rate according to our and previous studies.1339 Because of ripple effect of HCWs having infectious TB, the Korean government set a policy to conduct mandatory annual LTBI screening among HCWs. All HCWs, regardless of age and sex, should begin LTBI treatment as soon as they are diagnosed, which should be accompanied by development of an efficacious treatment regimen.
This cohort study has several strengths. First, data-linkage between the unique electronic nationwide databases allowed us to perform a comprehensive analysis of the cascade of care among the entire HCWs in Korea. All the participants enrolled in the cohort can be scrutinised during the follow-up period, thereby minimising the rate of follow-up loss. Our cohort study design was planned in advanced and prospectively constructed. Second, the large sample size provided adequate power for the detection of clinically meaningful factors associated with each step of the LTBI cascade of care. Third, the numbers of missing values for the independent variables were very low with the use of the database-linkage system.
Despite these strengths, a major limitation is that specific causes of drop-out for each stage of LTBI cascade of care could not be identified. There are various reasons associated losses at different steps.13 For example, details on adverse drug reactions during preventive therapy were not collected. Further qualitative research assessing perspective of both patients and physicians are necessary for planning different strategies and public health interventions for each step of the LTBI cascade of care.4041 Second, the completeness of LTBI treatment is defined by the number of prescribed anti-TB drugs, based on insurance claims. Since adherence to the treatment cannot be assessed during the follow-up period, we hypothesised that all the prescribed anti-TB drugs were taken.
Given the potentially high level of occupation exposure and the risk of further transmission to patients, HCW is one of the risk groups which the WHO recommends to consider for systematic screening for TB disease.5 Our finding showed that proportion of completing LTBI treatment was high among elderly participants, which indicates that target group of TPT could be expanded. Public health center was an important determinant for not-initiating and not-completing treatment, which implies the role of physician-in-charge is important when participants with LTBI first meet in the clinic. Compared to 9INH, RIF-based short treatment regimens were efficient in terms of completion rate, which provides more evidence for selecting appropriate shorter and better-tolerated TB preventive treatment regimen. We need to provide better interventions and develop uptake supports, which minimise gaps of LTBI care. Such efforts are only possible with obtainment of a larger body of scientific evidence for the target population and cooperation among the government, the public and various stakeholders.
 XML Download
XML Download