

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first coronavirus disease 2019 (COVID-19) case in December 2019,1 the virus has spread rapidly worldwide. By mid-December 2021, there were 270,153,117 confirmed cases and 5,321,825 deaths globally.2 Subsequently, healthcare workers in divergent clinical units have experienced a variety of mental health challenges. A meta-analysis of the psychological impact of COVID-19 on healthcare workers showed a prevalence of 23.2–26% for anxiety and 22.8–25% for depression.3 Physical distancing can be one of most effective measures against spreading the disease, but it may impose substantial costs on society. Consequently, the Korean government announced a policy of living with COVID-19 (“with corona”)4 from November 1, 2021. However, after the policy introduction, confirmed cases per day rapidly increased to 7,000 in South Korea.5 Healthcare workers were required to work in conditions that were “uncertain” with regard to the safety of patients or themselves.
Intolerance of uncertainty is defined as “a dispositional incapacity to endure the aversive response triggered by the perceived absence of salient, key, or sufficient information, and sustained by the associated perception of uncertainty.”6 It is considered to play a role as a risk factor or cognitive vulnerability in the development and maintenance of anxiety and problematic worry.78 In the COVID-19 pandemic, intolerance of uncertainty was reported as predicting anxiety, sleep problems, and depression,9101112 and as influencing behavioral changes in procrastination13 or emotional eating.14 We can speculate that viral anxiety (an anxiety response specifically to the viral epidemic)15 can also be affected by intolerance of uncertainty in this pandemic. Therefore, reducing intolerance of uncertainty is important to curb viral anxiety by increasing predictability or controllability.16
Frontline healthcare workers have suffered psychological distress in the wake of the pandemic.17 They are required to play a major role in preventing the spread of COVID-19 and to take care of infected or high-risk patients in the hospital. They have experienced increased workloads, reluctance to work, perceived stigmatization, coping by avoiding crowds and colleagues, and feelings of being scrutinized.18 They have also experienced severe emotional stress, such as anxiety, worrying, burnout, insomnia, or depressive symptoms. Intolerance of uncertainty can be one of the factors that aggravates the psychological distress of healthcare workers. Unlike catastrophes in which the victims do not transfer the consequences to others, the victims of a viral catastrophe can contaminate healthcare workers in the hospital. Healthcare workers have had to take care of patients in the face of a lack of personal protective equipment, work overload, poor infection control, and pre-existing medical conditions; they were identified as risk factors for the disease.19 Consequently, they have had to anticipate risks and tolerate uncertainty. Greater difficulties in tolerating uncertainty have been reported among high-risk healthcare workers than among a low-burnout group,20 and uncertainty can increase the ruminative thinking style of healthcare workers in a pandemic.21
Illness anxiety disorder (formerly known as hypochondriasis) is characterized by a preoccupation with fear of serious illness despite medical reassurance.22 A cognitive-behavioral model of illness anxiety has been proposed, according to which fears of being sick make an individual anxious, which leads them to try to avoid the problem or seek reassurance.2324 The short-term relief from reassurance makes the original fear stronger and will induce preoccupation with the illness.22 In the context of COVID-19, this process may entail checks on bodily sensation, hand hygiene, visits to the doctor, and repeated media research. Nearly everyone experiences health anxiety to some degree; these behaviors help identify and protect early signs of health problems. However, recurrent engagement in reassurance-seeking behaviors paradoxically increases anxiety.25 Anxiety and uncertainty can drive excessive media consumption and distress, creating a cycle that can be difficult to break.26 Studies have reported that cyberchondria involves excessive internet use associated with increasing levels of health anxiety or distress.27282930 This situation can lead to increased susceptibility to physical symptoms and promotion of behaviors that negatively impact the healthcare systems, such as frequent screening clinic visits and panic buying of masks, with downstream mental and physical health consequences.29 People with high health anxiety have an ongoing need for reassurance, a sign of which may be resorting to the reassurance-seeking behavior as a compulsion.31
For healthcare workers who are in the frontline of the COVID-19 battle, factors influencing psychological burden are being female, being a nurse, having a high risk of contracting COVID-19, a lower socioeconomic status, social isolation, and spending longer time watching COVID-19-related news. Protective factors are having sufficient medical resources, having up-to-date and accurate health information, and taking precautionary measures (e.g., hand hygiene and wearing masks).3 Healthcare workers try to anticipate and control the spread of the virus for the safety of patients, themselves, and their family or friends, which encourages excessive reassurance-seeking as a protective behavior.
The specific purpose of this study is to further understand when intolerance of uncertainty prompts viral anxiety by examining the mediating role of reassurance-seeking behavior and obsession among healthcare workers. The hypotheses in this study are: 1) intolerance of uncertainty will be positively related to viral anxiety, 2) reassurance-seeking behavior will mediate the relationship between intolerance of uncertainty and virtual anxiety, and 3) obsession with COVID-19 will mediate the relationship between intolerance of uncertainty and virtual anxiety. The findings offer insights into the psychological factors that require intervention to regulate the viral anxiety response in the high-risk healthcare worker group with an intolerance of uncertainty.
Go to : 
METHODS
Participants and procedure
On November 29, 2021, an online survey was conducted among healthcare workers at the Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. It was anonymous and we did not collect any identifiable personal information. The participants voluntarily completed the survey and a reward coupon of about 5 US dollars was provided for participation.
The survey form was developed using Google Forms. It included questions on healthcare workers’ age, sex, years of employment, and marital status, and responses to COVID-19-related questions, such as “Have you experienced taking care of confirmed COVID-19 patients?” “Did you experience being quarantined due to infection with COVID-19?” “Did you experience being infected with COVID-19?” and “Did you get vaccinated?” The past psychiatric history of the participants was checked by the question “Did you have experience of or were you treated for depression, anxiety, or insomnia?” Their current psychiatric distress was checked by the question “Do you think you are currently depressed or anxious, or do you need help for your mood state?” We developed the survey form according to the Checklist for Reporting Results of Internet e-Surveys (CHERRIES) guidelines32 and investigators tested the usability and technical functionality before its implementation.
Measures
Stress and Anxiety to Viral Epidemics-9 (SAVE-9)
The SAVE-9 scale is a self-report rating scale that can measure the work-related stress and anxiety response of healthcare workers to viral epidemics.15 It consists of 9 items rated on a 5-point Likert scale ranging from 0 (never) to 4 (always). A higher total score reflects a more severe degree of work-related stress and anxiety response to viral epidemics. In this study, we applied the original Korean version of SAVE-9, and Cronbach’s alpha among this sample was 0.805.
Coronavirus Reassurance-Seeking Behaviors Scale (CRBS)
The CRBS is a self-report scale that can measure excessive reassurance-seeking behaviors, which can lead to increased anxiety related to concerns about coronavirus infection.33 It consists of 5 items that can be rated from 0 (not at all) to 4 (nearly every day). A high total score reflects an excessive preoccupation with COVID-19 information. In this study, we applied the Korean version of CRBS,34 and Cronbach’s alpha among this sample was 0.872.
Obsession with COVID-19 Scale (OCS)
The OCS is a self-report scale that can measure persistent disturbing thinking related to COVID-19.35 It consists of 4 items that can be rated on a 5-point scale from 0 (not at all) to 4 (nearly every day over the last 2 weeks). A high total score reflects a high level of obsession with COVID-19. In this study, we applied the Korean version of the OCS,35 and Cronbach’s alpha in this sample was 0.804.
Insomnia Severity Scale (ISI)
The ISI is a self-rated scale developed to measure the severity of insomnia.38 The 7 items of ISI can be rated on a 0–4 Likert scale, and a high total score reflects a severe degree of insomnia. In this study, we applied the Korean version of the ISI,38 and Cronbach’s alpha was 0.834 among this sample.
Intolerance of Uncertainty-12 (IUS-12)
The IUS-12 is a shortened version of the original IUS,39 which was developed to measure intolerance of uncertainty. Each of the 12 items can be rated according to degree of agreement (1 to 7), and a high total score represents greater intolerance of uncertainty. In this study, we applied the Korean version of the IUS-12 scale,40 and Cronbach’s alpha among this sample was 0.842.
Statistical analysis
The participants’ clinical characteristics and rating scale scores are summarized as mean ± standard deviation. Pearson’s correlation analysis was performed to explore the association among age, years of employment, and rating scale scores. Linear regression analysis was conducted to determine which variables could predict the viral anxiety of healthcare workers. The mediating effect of reassurance-seeking behavior or obsession with COVID-19 on the association between intolerance of uncertainty and viral anxiety was examined by implementing the bootstrap method with 2,000 resamples. The level of significance for the analyses was defined as two-tailed at values of P < 0.05. The SPSS version 21.0, AMOS version 27 for Windows (IBM Corp., Armonk, NY, USA), and Jamovi version 1.6.18.0 were used to perform the statistical analysis.
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of the Asan Medical Center (2021-1682), and the need to obtain written informed consent was waived by the IRB.
Go to :
RESULTS
Of the 330 responses from the healthcare workers, 329 were used for the statistical analysis, excluding one that lacked agreement for use in the study. Of the participants, 264 (81.4%) were female, 194 (59.0%) were nursing professionals, 157 (47.7%) were single, and 73 (22.3%) were shift workers (Table 1). For the questions on COVID-19, 45 (13.7%) had experienced being quarantined, 2 (0.6%) had experienced being infected, and 327 (99.4%) had been vaccinated. In addition, 46 (13.9%) had a prior psychiatric history, and 24 (7.3%) reported currently experiencing psychological distress or needing help for their symptoms.
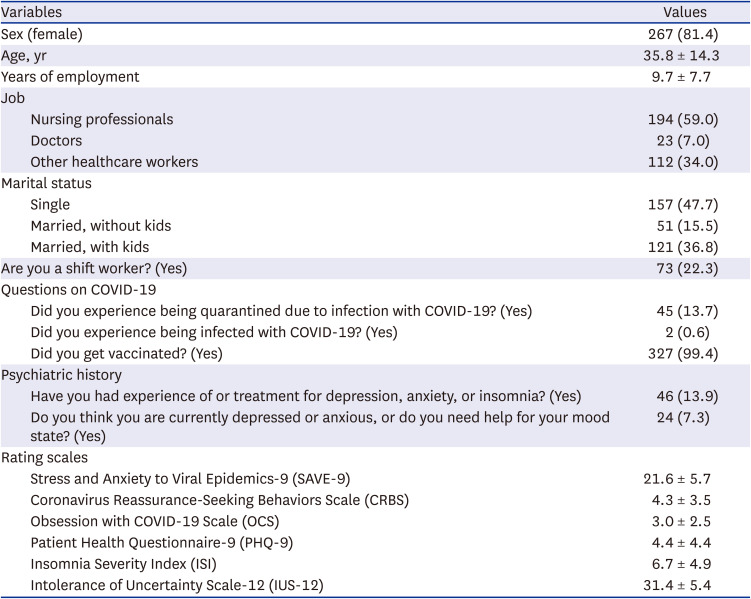
Table 1
Clinical characteristics of participants (N = 329)
Values are presented as mean ± standard deviation or number (%).
COVID-19 = coronavirus disease 2019.
![]()
The SAVE-9 score was positively correlated with the CRBS (r = 0.57, P < 0.001), OCS (r = 0.58, P < 0.01), PHQ-9 (r = 0.34, P < 0.001), ISI (r = 0.30, P < 0.001), and IUS-12 scores (r = 0.31, P < 0.001). The CRBS score was significantly correlated with the OCS (r = 0.71, P < 0.001), PHQ-9 (r = 0.41, P < 0.001), ISI (r = 0.39, P < 0.001), and IUS-12 scores (r = 0.25, P < 0.001). The OCS score was significantly correlated with the PHQ-9 (r = 0.49, P < 0.001), ISI (r = 0.35, P < 0.001) and IUS-12 scores (r = 0.20, P < 0.001). The PHQ-9 score was correlated with the ISI (r = 0.56, P < 0.001) and IUS-12 scores (r = 0.36, P < 0.001), and the ISI score was correlated with the IUS-12 score (r = 0.27, P < 0.001) (Table 2).

Table 2
Correlation coefficients of each variables in all participants
COVID-19 = coronavirus disease 2019, SAVE-6 = Stress and Anxiety to Viral Epidemics-9 (6 items), CRBS = Coronavirus Reassurance-Seeking Behaviors Scale, OCS = Obsession with COVID-19 Scale, PHQ-9 = Patient Health Questionnaire-9, ISI = Insomnia Severity Scale, IUS-12 = Intolerance of Uncertainty Scale-12.
***P < 0.001.
![]()
Linear regression analysis, conducted to identify the factors predicting the viral anxiety of healthcare workers, revealed that being female (β = 0.14, P = 0.002) and the CRBS (β = 0.30, P < 0.001), OCS (β = 0.32, P < 0.001), and IUS-12 scores (β = 0.15, P = 0.002) were significant predicting factors for viral anxiety (adjusted R2 = 0.43, F = 31.1, P < 0.001) (Table 3).

Table 3
Linear regression analysis to explore the predicting factors for viral anxiety of healthcare workers
COVID-19 = coronavirus disease 2019, SAVE-9 = Stress and Anxiety to Viral Epidemics-9, CRBS = Coronavirus Reassurance-Seeking Behaviors Scale, OCS = Obsession with COVID-19 Scale, PHQ-9 = Patient Health Questionnair-9, ISI = Insomnia Severity Index, IUS-12 = Intolerance of Uncertainty Scale-12.
![]()
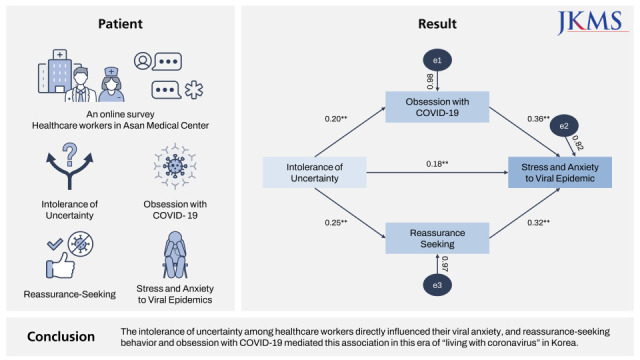
Mediation analysis showed that the complete pathway from intolerance of uncertainty (independent variable) to reassurance-seeking behavior or obsession with COVID-19 (mediator) to viral anxiety (dependent variable) was significant (Table 4). It also indicates that reassurance-seeking behavior and obsession with COVID-19 partially mediate the effects of intolerance of uncertainty on the viral anxiety of healthcare workers (Fig. 1).

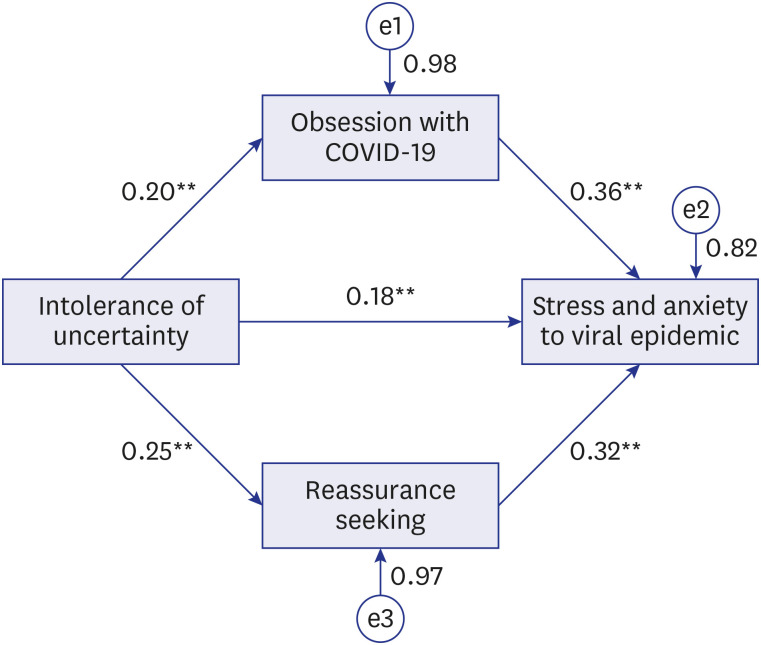 | Fig. 1Mediation model showing the influence of intolerance of uncertainty (independent variables) on viral anxiety (outcome) is mediated by reassurance-seeking behavior and obsession with COVID-19 (mediator).COVID-19 = coronavirus disease 2019.
**P < 0.01.
|
Table 4
The results of direct, indirect, and total effects on mediation analysis
CI = confidence interval, COVID-19 = coronavirus disease 2019, SAVE-6 = Stress and Anxiety to Viral Epidemics-6, CRBS = Coronavirus Reassurance-Seeking Behavior Scale, OCS = Obsession with COVID-19 Scale, IUS-12 = Intolerance of Uncertainty Scale-12.
![]()
Go to :
DISCUSSION
In this study, we observed that reassurance-seeking behavior, obsession with COVID-19, and intolerance of uncertainty were significant factors that predicted healthcare workers’ viral anxiety in this “with corona” era. In addition, healthcare workers’ reassurance-seeking behavior or obsession with COVID-19 mediated the association between intolerance of uncertainty and viral anxiety.
Among the general population in the H1N1 pandemic, viral threat was reported as being accompanied by high levels of anxiety among individuals with high intolerance of uncertainty.41 During the COVID-19 pandemic, intolerance of uncertainty has been reported as having a significant effect on anxiety symptoms.42 However, it is not easy to find previous literature on the relationship between intolerance of uncertainty and viral anxiety that was assessed using a viral epidemic–specific rating scale, especially among healthcare workers. In this study, we observed that intolerance of uncertainty among healthcare workers directly influenced their viral anxiety. Healthcare workers have already adjusted to 2 years of the pandemic, which means that predictability and controllability might have increased in terms of anxiety management. However, after the announcement of the “living with coronavirus” policy of the Korean government, the number of confirmed cases rapidly increased to 7,000 cases per day, which could have worsened the uncertainty of infectivity among the public.5 The uncertainty of infectivity will emotionally influence healthcare workers’ concerns about the safety of their patients, of themselves, or of their family members and friends. Thus, we can assume that their concerns about uncertain conditions will make it hard for healthcare workers, with their intolerance of uncertainty influencing their viral anxiety in a vicious cycle.
Reassurance-seeking behavior mediated the association between intolerance of uncertainty and viral anxiety in this study. It was believed that the fear of getting sick generated anxiety and that such anxiety would result in reassurance seeking, thus inducing a preoccupation with the illness.222324 During COVID-19, the influence of healthcare workers’ intolerance of uncertainty on their viral anxiety can be mediated by their reassurance-seeking behavior, such as checking bodily sensations, hand hygiene, or repeated media research. Healthcare workers who cannot tolerate uncertainty well might seek reassurance by checking for fever, repetitive hand washing, or excessive information gathering, which might increase their viral anxiety.
Obsession with COVID-19 also mediated the association between intolerance of uncertainty and viral anxiety among this sample. The OCS is a self-report rating scale that can screen persistent and disturbed thinking about COVID-19.43 This persistent thinking about or preoccupation with COVID-19 can influence the viral anxiety of healthcare workers. With regard to generalized anxiety disorder, intolerance of uncertainty may lead to a preoccupation with the minor details of a problem.44 In Obsessive Compulsive Disorder, cognitive models propose a preoccupation with thoughts or beliefs that lead to biased interpretations of intrusions or intolerance of uncertainty.45 During the pandemic, healthcare workers who cannot tolerate uncertain conditions may have a preoccupation with COVID-19, which can increase their viral anxiety.
Based on a cognitive-behavioral model of illness anxiety, we observed that the intolerance of uncertainty led to reassurance seeking and preoccupation with COVID-19, with this behavior increasing viral anxiety among healthcare workers. The strength of this study lies, first, in the application of the SAVE-6 anxiety scale, which is specific to viral epidemics. In previous research, anxiety scales that can be used in general were applied. Viral epidemic–specific anxiety scales enable us to acquire information about viral anxiety rather than non-specific general anxiety. Second, we conducted a survey among healthcare workers. We expect that healthcare workers might experience viral anxiety or engage in excessive reassurance-seeking behavior. However, in these 2 years of the pandemic, healthcare workers might already have adjusted to the pandemic situation. We can confirm that they also manifest reassurance-seeking behavior or exhibit a preoccupation with COVID-19, which can augment their viral anxiety. Third, this study was conducted after the announcement of the “living with coronavirus” policy by the Korean government and during a subsequent larger wave of the outbreak. It may be the first of its kind in South Korea, which explored the meaning of intolerance of uncertainty among healthcare workers.
This study has several limitations. First, the online survey design of this study may have led to bias. Recently, the number of confirmed cases rapidly increased inside the hospital, and face-to-face interviews were not possible. Therefore, we decided to conduct the survey online despite the possible lack of reliability of the responses. Second, the results from the small number of participants, 329 workers (3.6%) among a total of 9,216 workers, including 1,759 medical doctors, 4,526 nursing professionals, and 2,931 other workers in the hospital, cannot be generalized to other groups. Third, 13.7% of participants experienced being quarantined, and only 2 (0.6%) workers were infected, but the high proportion of those vaccinated (99.4%) might have influenced the results. Being vaccinated can be regarded as reducing uncertainty. However, the number of confirmed cases rapidly rose in this period and might have increased the uncertainty.
We concluded that intolerance of uncertainty among healthcare workers directly influenced their viral anxiety, and reassurance-seeking behavior and obsession with COVID-19 mediated this association in this era of “living with coronavirus” in Korea. To reduce healthcare workers’ viral anxiety, we need to develop a program in which we can apply the concept of illness anxiety disorder during the pandemic.
Go to :
 XML Download
XML Download