

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Spiraling costs of health care are a cause of concern to patients, medical professionals and governments worldwide. Although the harms caused by increasing health care costs due to low value services have been pointed out for a long time, in clinical practice, it is not always possible to distinguish and eliminate low value service.1 This resulted in failure to increase efficacy in health care resource utilization. Unnecessary and inappropriate laboratory testing accounts for a significant portion of waste in health care utilization,2 however, because these tests are relatively inexpensive compared to other high cost tests, such as radiologic imaging, waste arising from low value laboratory tests has been under the radar of scrutiny by health care policy stakeholders. As a result, laboratory tests have become the highest growing portion of health care costs.3 A study of all patients registered to UK General Practices from 2000 to 2015 showed that age and sex adjusted use of tests increased by 8.5% annually in both sexes and across all age groups and test types, with the highest increase for laboratory tests.3 An Australian study reported a 54% increase in laboratory tests ordered between 2000–2007, the usefulness of which remains uncertain.4 In a study of advanced breast cancer patients in Finland, it was shown that the number of diagnostic tests per patient per month increased continually during the last 6 months until death, such that 46.9% of all laboratory tests were made during the last 2 months of life.5 This suggests that a large number of laboratory tests are used without avoiding the worst health outcome, death. A case-control study of Italian residents aged 55 and above, matched by age and gender, showed that laboratory tests were used more than 3 times more among subjects who died after 1 year than those who survived. This again implies that increased use of laboratory tests is not associated with better outcome, and reducing its use would lead to more effective use of health care resources with a consequent cost containment.6
Screening tests that have high false positive rate are especially problematic. When requested without appropriate clinical context, tests that screen for uncommon diseases but have a high rate of false positivity can lead to multiple unfavorable consequences, including misdiagnosis, unnecessary or potentially harmful follow-up testing, and even inappropriate treatment.7 The detection of anti-nuclear antibodies (ANAs) has been established as an important adjunct to the diagnosis and classification of connective tissue diseases (CTDs) such as systemic lupus erythematosus (SLE) and Sjögren’s syndrome (SjS). However, ANA has been criticized as an exemplar of a low-value test because of its high false positivity rate.8 In addition, the reading of the anti-nuclear antibody test is very labor-intensive. Therefore, efforts are being made for automation, but there are still many restrictions.9 Particularly, the referral to rheumatology for the sole reason of positive ANA tests has been frequently criticized as an unnecessary waste of health care resources.710 In response to these issues, a “Choosing wisely” campaign has recently emerged worldwide.11 In a study of healthy individuals from the 15 international centers including US, Europe, and Japan, ANA was positive in 31.7% of individuals at 1:40 serum dilution, and even at as high titer as 1:320, 3.3% were positive.12 Another study in the general public who donated blood showed a ANA positivity rate of 22.6% at the titer of 1:40.13 In an administrative database study using a Central Referral and Triage (CReATe) service in the Calgary Health Region, only 24% of ANA positive patients referred to specialists because of ANA positivity were provided a diagnosis of an ANA associated rheumatic disease (AARD).10 A study from a single US institute reported that positive predictive value (PPV) of ANA test was 11% for SLE and 11% for other rheumatic diseases, concluding that positive ANA test results are poorly predictive of CTD.14
Practice patterns differ widely between US or Europe and Asia, and the pattern of ANA use and its value has not been reported in Asian clinical setting. The aim of this study was to assess: 1) the rate of AARD diagnosis among ANA tested and ANA positive subjects overall and according to the requesting department and 2) PPV of ANA test leading to AARD diagnosis in different ANA titers and different subsets of patients in 5 hospitals affiliated with a university during the last 10 years.
Go to : 
METHODS
We retrospectively extracted data from all subjects who were tested for ANA at five hospitals affiliated with Hallym University Medical Center from year 2010 to 2019. Then, clinical data including ANA result (positive at titer ≥ 1:40 or not), requesting department, and whether these patients were given AARD diagnosis were extracted. SLE, SjS, scleroderma, mixed CTD, dermatomyositis, polymyositis, and undifferentiated CTD were included as AARD. Patients diagnosed with AARD before ANA test were excluded. Those who were tested multiple times and who had discrepant results were considered positive if tested positive once.
Next, those who were first evaluated at or referred to rheumatology were further evaluated with extraction of data including ANA titer and ultimate diagnosis. In these cases, diagnoses were made by rheumatologists according to American College of Rheumatology criteria.15161718 PPVs were determined as the number of patients with an AARD divided by the number of total patients positive for ANA within the group. PPVs for ANA test were evaluated after stratification according to clinically relevant key parameters, such as patient age (younger < 65 years vs older), sex, and requesting department. All samples were tested using HEp-2 cell based assay and except for 7.5% of samples, tested with the same kit (Kallestad; Bio-Rad Laboratories, Hercules, CA, USA).
Statistical analysis
We calculated % ANA positivity as the number of ANA positive among all ANA tested patients.
PPVs were determined as the number of patients with an AARD divided by the number of total patients positive for ANA. PPVs for ANA test were evaluated after stratification according to clinically relevant key parameters, such as patient age (younger [< 65 years] vs. older), sex, and requesting department. The differences in categorical variables such as gender, age, and requesting department were calculated with the use of χ2 test. The statistical analyses were conducted using Microsoft Excel 2016. Statistical significance was defined as a P value < 0.05.
Ethics statement
Since this is a retrospective study, we received an expedited approval through the Institutional Review Board (IRB) of Hallym University Sacred Heart Hospital (IRB number: HALLYM 2020-02-002). All data were obtained through the clinical data warehouse of Hallym University affiliated hospitals with encrypted personal information.
Go to :
RESULTS
ANA tests were requested in a total of 94,153 patients from 2010 to 2019 at Hallym University Medical Center (Table 1). Of the total 94,153 patients, 63,843 (67.8% of total) received only qualitative antibody tests. The remaining 30,310 patients underwent both qualitative and quantitative tests or only quantitative tests. ANA positivity rate was 14.4% and varied according to the requesting department, with the highest rate for rheumatology (19.9%). AARD was diagnosed in 645 (0.69%) among all ANA tested patients, and diagnosis rate varied according to requesting department with the highest for rheumatology and hemato-oncology (1.73% and 1.23%, respectively). However, for all other departments, diagnosis of AARD was made in less than 1% of ANA tested subjects. AARD was diagnosed in 4.74% among all ANA positive patients. AARD diagnosis rate among ANA positive patients was the highest for rheumatology, followed by nephrology and hemato-oncology (8.7%, 6.95%, and 6.86%, respectively). AARD diagnosis rate was the lowest among both ANA tested and ANA positive patients when requested by orthopedics (0.14% and 1.23%, respectively). Among 13,600 ANA positive patients, 7,312 patients were evaluated by rheumatologists.

Table 1
The number of ANA tests, rate of ANA positivity and AARD diagnosis among ANA tested subjects according to the requesting department
![]()
By using a cutoff titer for test positivity of 1:40, the PPV of ANA test was 6.5% for any AARD and 3.2% for SLE (Table 2). Using higher-titer cutoffs yielded higher PPVs, with the threshold value for positivity at 1:320 yielding a PPV of 15.6% and 7.8% for any AARD and SLE. About two-thirds of patients showed titer < 1:320. Even the highest titer (≥ 1:1,280) had PPV of only 24.8% for any AARD. Two hundred thirty-five patients were diagnosed with SLE, and although it is the most common differential diagnosis for screening ANA test, PPV was only 12.2% for the highest ANA titer.
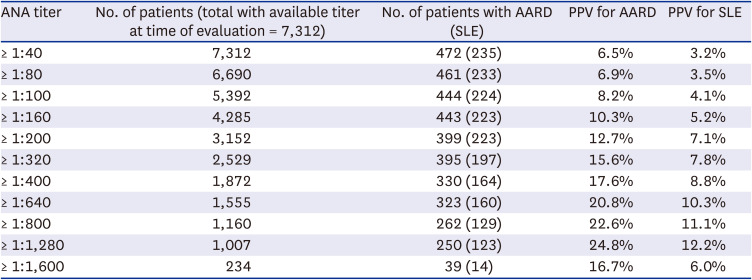
Table 2
PPV of ANA by titer
PPV = positive predictive value, ANA = anti-nuclear antibody, AARD = anti-nuclear antibody-associated rheumatic disease, SLE = systemic lupus erythematosus.
![]()
Table 3 shows the specific AARD diagnosed in each category of ANA titer.
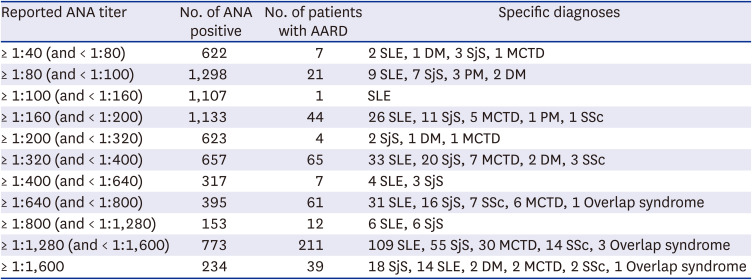
Table 3
AARD diagnosed by ANA titer
AARD = anti-nuclear antibody-associated rheumatic disease, ANA = anti-nuclear antibody, SLE = systemic lupus erythematosus, DM = dermatomyositis, SjS = Sjögren’s syndrome, MCTD = mixed connective tissue disease, PM = polymyositis, SSc = systemic sclerosis.
![]()
Although AARDs were more common in the higher titer group (≥ 1:320), it is of note that some AARD including SLE patients also exhibited low titer ANA.
Next, PPV of ANA test was compared according to sex, age and department that requested ANA (Table 4). In line with the increase in the rate of false positive ANA in older populations, the PPV of ANA test was higher among the younger subjects (< 65 years) in our cohort. In addition, PPV was more than 3 times higher in women than men. PPV was significantly higher when ANA was requested by a rheumatologist vs. other departments, or when it was requested by internal medicine departments vs. other departments.
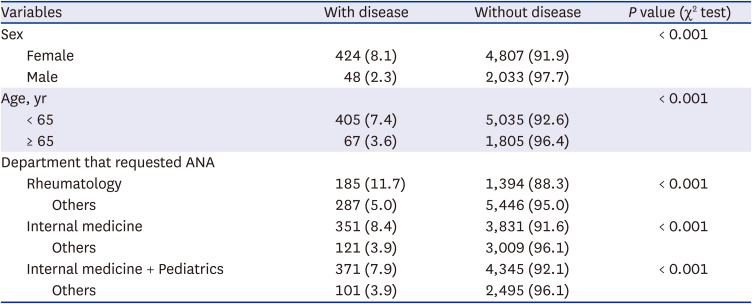
Table 4
PPV of ANA by sex, age, and requesting department
Values are presented as number of patients (%).
PPV = positive predictive value, ANA = anti-nuclear antibody.
![]()
Go to :
DISCUSSION
It is widely reported that low-value health care services, most commonly laboratory tests and procedural treatments providing minimal benefit relative to cost, are prevalent and costly all over the world. In this study, we examined the diagnostic value of ANA test, one of the typical low value tests, leading to AARD diagnosis in 5 university affiliated hospitals during the last 10 years. The result shows that ANA positivity rate was 14.4% and AARD was diagnosed in less than 1% among all ANA tested subjects. This is similar to the recently reported positive rate of ANA test in healthy Chinese.19 Especially, AARD was diagnosed in only 4.74% even among ANA positive patients. Diagnosis rate varied significantly according to the department requesting the test. Our study is in line with previous reports from Western countries and China which revealed low value of ANA screening test.20
PPV of ANA test for AARD may vary depending not only on the population tested, but also on the pattern of health care utilization and reimbursement pattern. In previous reports from US and Canada, PPV of ANA positivity for AARD in patients referred to rheumatology ranged from 9.1 to 24%10 for any AARD. PPV of 6.5% for any AARD and 3.2% for SLE of our study is even lower than the lowest value of previous reports, and even at high threshold value for positivity (1:320), PPVs were only 15.6% and 7.8% for any AARD and SLE, respectively. This is a cause of concern considering that this study was performed in a university affiliated hospital setting, because poor predictive value of a positive ANA is usually attributable to unnecessary testing in patients with low pretest probabilities for AARD. Both AARD diagnosis rate among ANA tested and ANA positive subjects were the lowest when it was requested by orthopedic surgery, and because the most common reason for ordering ANA testing is musculoskeletal pain,6 it is possible that many patients with non-AARD, such as degenerative joint disease would have been tested. ANA test requested from dermatology also had low PPV, suggesting that ANA testing among non-specific skin symptoms is prevalent. This pattern may shed light on the strategy of reducing low value ANA test, because these 2 departments were those that requested the most and the 3rd most number of ANA tests, respectively. Not surprisingly, AARD diagnosis rate was higher when it was requested by internal medicine, especially rheumatology, however, AARD diagnosis was made in only 1.73% of ANA tested patients even when it was requested from rheumatology, leaving room for improvement.
Contrary to reports from Western countries, where AARD was rarely identified in patients with an ANA < 1:160, 15% of patients in our study were diagnosed with various AARD, most commonly with SLE and SjS at such low titer. This discrepancy might have stemmed from differences in ethnicity or test methods used. Still, this is another finding corroborating the low diagnostic value of ANA test since low titer does not help exclude the disease, either. PPV was higher among females and younger subjects, which is explained by higher prevalence of AARD among females and higher ANA false positivity rate among the elderly, respectively.
Although the problem of low value tests is well known, it is not well studied why its use does not decrease over time and whether it depends on the health care policy, particularly on the reimbursement system. A study compared changes in the use of low-value vitamin D level test, either after the release of Choosing Wisely Recommendations across health care jurisdictions or after a related policy change.11 The result showed that the use of low value vitamin D test decreased only marginally with the release of Choosing Wisely Recommendations (4.5–14.0%), however, policy eliminating reimbursement for low-value vitamin D screening was associated with a 92.7% relative reduction, suggesting that pairing recommendations with policy changes is more effective than recommendation alone.11 Imbalance of re-imbursement for clinician time and laboratory test would be another cause of over-use of laboratory tests in Korea. For example, the ratio between hemoglobin A1C test fee and consultation fee was much lower in Korea compared to US, Canada or France (0.58 vs. 0.09, 0.07 and 0.27, respectively, manuscript in submission), suggesting under-compensation for physician time compared to laboratory tests in Korea. Furthermore, the fee for ANA increased almost 100% while consultation fee increased less than 50% from year 2005–2019 in Korea, aggravating such imbalance (unpublished data). In a fee-for service reimbursement system, this imbalance in fee system would only exacerbate the overzealous use of lab tests. Abrupt change in reimbursement policy for ANA test without backing up for high quality clinician consultation, however, would lead to the more serious problem of missing the diagnosis of AARD in patients. Since it has been reported that autoantibodies are detected in the absence of AARD at the time of testing, and predating it by decades,2122 how to use ANA test prudently is never a simple issue.
Our study has limitations. It was a retrospective study using a patient database from five hospitals affiliated with a single university, thus it may not be generalizable in other clinical settings. However, the low AARD diagnosis rate among ANA tested patients even in a university hospital setting is a finding that raises cause of concern. Some patients were not tested with a quantitative test, thus, ANA titer was missing in some. It would be very important to investigate the ANA pattern and its diagnostic value. However, we could not analyze this point in this study. This is a subject for our future study.
In conclusion, we showed that AARD was diagnosed in less than 1% among all ANA tested patients in university-affiliated hospitals. This result shows that careful consideration before ordering the screening ANA, especially for musculoskeletal pain or skin symptoms is needed to improve the utility of the test for providers and patients and to reduce health costs spurred by unnecessary testing and its consequences.
Go to :
 XML Download
XML Download