

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intravenous (IV) thrombolysis with recombinant tissue plasminogen activator (rtPA) is employed in recanalizing thrombosed intracranial vessels such as the internal carotid artery (ICA), middle cerebral artery (MCA), and its branches within 4.5 hours.123 Although the incidence and management of early recurrent ischemic stroke after IV administration of rtPA have not been extensively investigated, patients with stroke due to carotid artery atherosclerosis carry the highest risk of recurrence.4 Hence, the optimal treatment for patients with hyperacute stroke caused by stenosis or occlusion of the proximal ICA remains controversial. In addition, these patients frequently experience tandem intracranial artery occlusion. Tandem distal ICA and MCA occlusions independently predict resistance to IV rtPA therapy and are thus predictors for poor outcomes.56789 Treating acute stroke due to steno-occlusion of the corresponding proximal ICA with emergent carotid artery stenting (CAS) can lead to improvement of acute stroke symptoms, prevent further neurological deterioration, and reduce long-term recurrent stroke risk.101112131415 A combination of IV tPA and early CAS might be feasible treatment strategy.3161718 However, the risk of intracranial hemorrhage associated with early reperfusion might be increased during the first 24 hours after IV rtPA administration, and the American Stroke Association/American Heart Association advise against the use of antiplatelet agents during this time because of increased bleeding complications.1617 Nevertheless clinicians employ double antiplatelet regimen after CAS to prevent stent occlusion.31718 Therefore, the feasibility and safety of combining IV tPA and emergent CAS remains unmet need. The aim of our study was to evaluate the feasibility and safety of the combination therapy of IV rtPA and early CAS in patients with hyperacute ischemic stroke due to ICA steno-occlusion.
METHODS
Patient selection
Our study subjects were collected from the prospective CAS registry of a single stroke center at a tertiary medical institution. From November 2005 to October 2020, patients treated with IV rtPA up to 4.5 hours following ischemic stroke and who underwent urgent CAS due to high-grade proximal ICA stenosis or ICA occlusion were enrolled. Initially, treatment with IV rtPA within 3 hours of symptom onset was required, and after the European Cooperative Acute Stroke Study III published their criteria, this time window was extended to 4.5 hours.2 Patients considered for endovascular recanalization therapy met the following criteria: 1) initial National Institutes of Health Stroke Scale (NIHSS) score ≥ 4 after administration of IV rtPA, 2) computed tomography (CT) signs of ischemia that affected less than one-third of the MCA territory, 3) an angiographically documented cervical ICA occlusion or severe stenosis (≥ 90% NASCET) with or without intracranial artery occlusion. Patients were excluded if they met the following criteria: 1) pre-modified Rankin Scale (mRS) score ≥ 2; 2) dissection of the ICA; 3) chronic ICA occlusion; and 4) systemic diseases with a life expectancy of ≤ 1 year.
Acute reperfusion therapy
Before receiving IV rtPA, all patients were initially examined using CT and CT angiography to exclude hemorrhagic stroke.1920 According to clinician’s discretion, the patients were administered IV rtPA at a dose 0.6 mg/kg or 0.9 mg/kg.2122 All endovascular treatment procedures were performed via femoral access under conscious sedation. After the diagnostic angiograms, an 8- or 9 French guide catheter was advanced to the ipsilateral common carotid artery. If the ICA was completely occluded at the origin, the lesion was traversed with a microcatheter over a micro guidewire. To verify the passage into the true lumen, evaluate the length of the occlusive lesion for stent placing purposes, and assess the presence and extent of intraluminal thrombus, a microcatheter injection was performed. After confirming the lumen by injection from the microcatheter, the microguidewire was exchanged for an exchange wire. A proximal or distal embolic protection device was used in all the cases. After pre-stenting balloon angioplasty, CAS was performed with Acculink (Guidant), WALLSTENT (Boston Scientific, Natick, MA, USA), Cristallo Ideale (INVATEC), or Protege (ev3 Neurovascular). Post-stenting balloon angioplasty was performed when there was residual severe stenosis. Subsequently, an intracranial angiogram was performed to confirm intracranial occlusion. If intracranial arterial occlusion persisted after proximal revascularization, it was either treated with the Penumbra system, the Solitaire stent–based recanalization system, or a combination of mechanical recanalization and intra-arterial thrombolysis. Based on clinician’s discretion, intracranial thrombectomy was performed after angioplasty for the proximal ICA lesion, followed by CAS. After the intervention, immediate postprocedural brain CT was obtained. Unless apparent hemorrhagic transformation was detected, aspirin monotherapy or combined aspirin and clopidogrel was used to prevent stent thrombosis. Follow-up CT imaging was performed 24 hours after the procedure or whenever clinical worsening occurred. Patients were monitored in the intensive stroke care unit.
Outcome assessment
Age, sex, vascular risk factors, list of current medications, and clinical and imaging data were collected in our registry. To assess early ischemic changes, initial CT head scan before IV tPA was analyzed according to the ASPECT Score. Types of hemorrhagic transformation after reperfusion treatment were classified according to the European Cooperative Acute Stroke Study classification.23 According to the National Institute of Neurological Disorders and Stroke tPA trials, a symptomatic intracerebral hemorrhage was defined as a new-onset hemorrhage accompanied by any decline in neurologic status.21 Stroke severity was assessed using the NIHSS at the following time points: admission, end of IV rtPA infusion, at 24 hours, and at 7 days after stroke onset. The mRS was evaluated 90 days after CAS. Successful recanalization was defined as modified TICI grade ≥ 2b.24 Favorable outcome was defined as a 90-days mRS of ≤ 2. Three-month and twelve-month or longer stent patency was assessed by carotid ultrasound and/or CT angiography of neck. Stent restenosis was defined as ≥ 50% diameter, reducing stenosis or occlusion.25
RESULTS
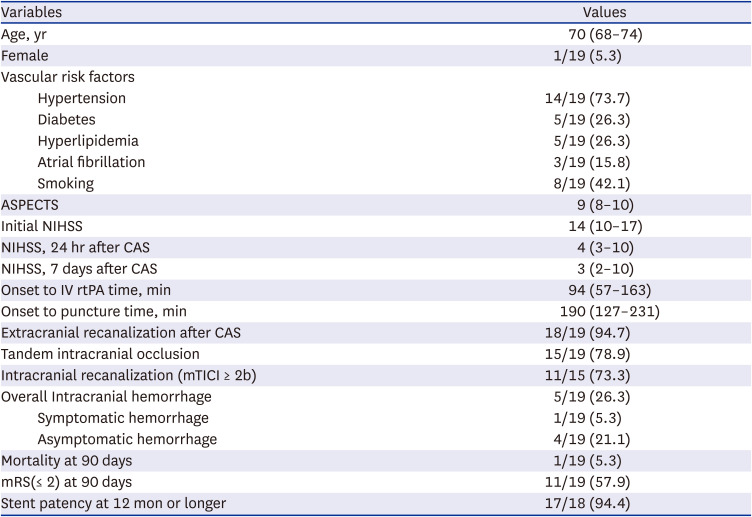
Nineteen patients with hyperacute stroke underwent emergent CAS after IV rtPA administration (Fig. 1). Patient demographics and procedure-related information are shown in Tables 1 and 2. The median age was 70 years (interquartile range 68–74). There were 18 men (94.7%) and one woman (5.3%). Vascular risk factors for stroke included hypertension (73.7%), diabetes (26.3%), hyperlipidemia (26.3%), atrial fibrillation (15.8%), and smoking (42.1%). The mean ASPECTS was 9 (8–10). Initial brain CT showed involvement of less than 1/3 of the MCA territory in all patients. The median initial NIHSS score was 14 (range, 10–17). All patients had an NIHSS score of at least 6 on admission. After 24 hours and 7 days of CAS, the median NIHSS scores were 4 (3–10) and 3 (2–10), respectively. The NIHSS score improved in 17 of 19 patients after 7 days of CAS. Patient No. 2 had no change in NIHSS score, and patient No. 9 died of sudden cardiac arrest at 3 days after CAS. The mean time from stroke onset to IV rtPA infusion and stroke onset to groin puncture were 94 (57–163) min and 190 (127–231) minutes, respectively (Table 3). Eleven patients received IV rtPA at a dose of 0.6 mg/kg, and eight patients were given 0.9 mg/kg.
Fig. 1
Patient enrollment flow diagram.
IV = intravenous, rtPA = recombinant tissue plasminogen activator, CAS = carotid artery stenting, ICA = internal carotid artery.
aInitially, treatment with IV rtPA within 3 hours of symptom onset, and after the ECASS III published their criteria, this time window was extended to 4.5 hours
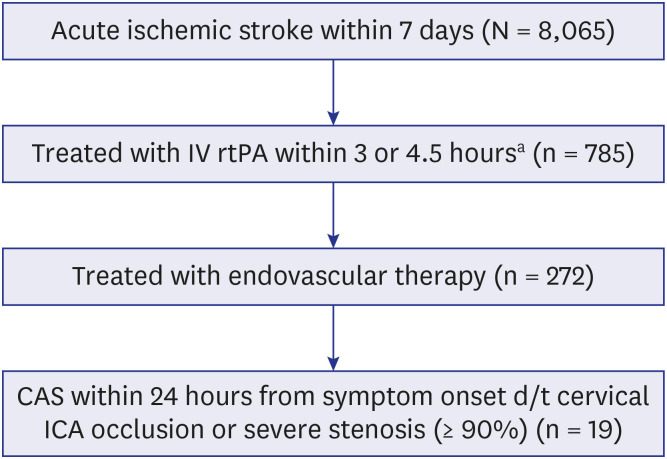
Table 1
Patient characteristics and clinical information
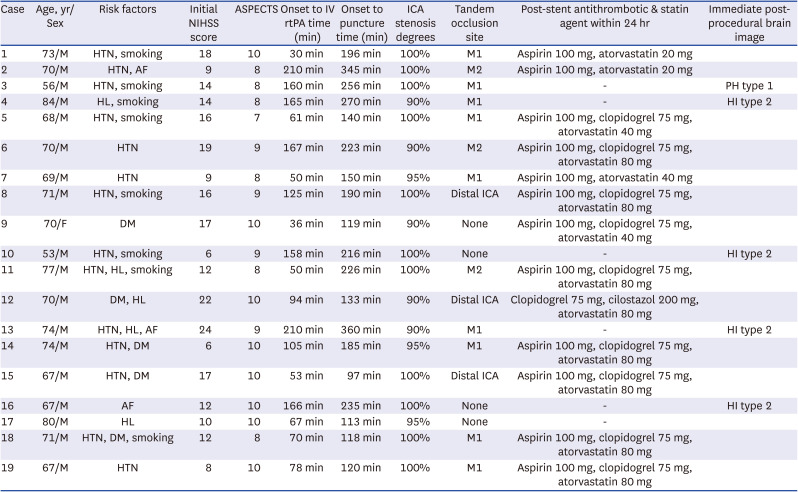
NIHSS = National Institutes of Health Stroke Scale, IV rtPA = intravenous recombinant tissue plasminogen activator, ICA = internal carotid artery, HTN = hypertension, M1 = M1 portion of the MCA, AF = atrial fibrillation, M2 = M2 portion of the MCA, PH = parenchymal hemoatoma, HL = hyperlipidemia, HI = hemorrhagic infarction, DM = diabetes mellitus.
Table 2
Recanalization procedures and outcomes
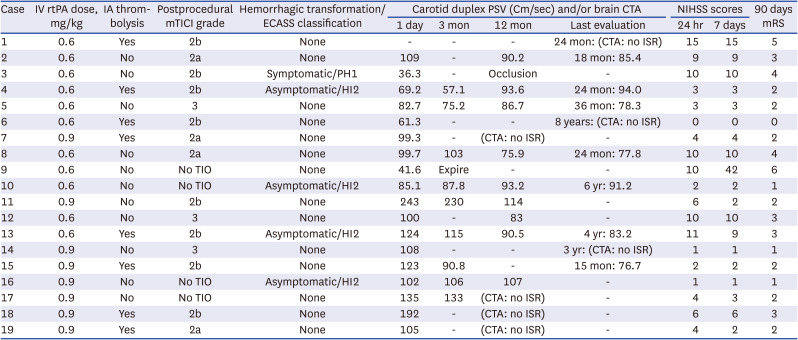
IV rtPA = intravenous recombinant tissue plasminogen activator, IA = intra-arterial, mTICI = modified TICI, ECASS = European Cooperative Acute Stroke Study, PSV = peak systolic velocity, CTA = computed tomography angiography, NIHSS = National Institutes of Health Stroke Scale, mRS = modified Rankin Scale, ISR = in stent restenosis, PH1 = Parenchymal hematoma type 1, HI2 = hemorrhage infarction type 2, TIO = tandem intracranial occlusion.
Table 3
Overview of patient population and outcomes
Of the 19 patients, 18 (94.7%) successfully underwent CAS, and the proximal ICA was recanalized. Patient No. 17 underwent a surgical procedure to remove the distal protection device that had entangled during CAS and subsequent urgent carotid endarterectomy. Fortunately, the proximal carotid artery was successfully recanalized after carotid endarterectomy. Of the 19 patients, 15 (78.9%) showed an additional intracranial occlusion after flow restoration in the proximal ICA: at the level of the distal ICA (n = 3), MCA M1 (n = 9), and MCA M2 (n = 3). In 4 patients, additional intracranial thrombectomy was not performed because of no tandem lesion (Table 1). After the procedure, modified TICI grade ≥ 2b was achieved in 11 patients (11/15, 73.3%). Of the 11 patients, 3 (27.3%) were classified as modified TICI grade 3 and 8 patients (72.7%) as grade 2b (Tables 2 and 3). During the emergency CAS, a balloon guide catheter was used in 6 cases (31.6%), and a distal protection device was used in 15 cases (78.9%). Pre-stenting balloon angioplasty was performed in 16 cases (84.2%) and post-stenting balloon angioplasty in 2 cases (10.5%).
Immediate post-procedural brain CT revealed hemorrhagic transformation in five patients (26.3%). Four patients (21.1%) were classified as having hemorrhagic infarction type 2, and one patient (5.3%) had parenchymal hematoma type 1. However, only patient No. 4 was symptomatic (Table 2). Five patients with hemorrhagic transformation and one (patient No. 17) who had undergone carotid endarterectomy were not administered antiplatelet agent within 24 hours (Table 1). Within 24 hours after the CAS, three patients were administered a single antiplatelet therapy and 10 were administered dual antiplatelet agents. Eleven patients (57.9%) had favorable outcomes at 90 days. The 90-day mortality rate was 5.3% (patient No. 9). Excluding the deceased (patient No. 9) and the carotid endarterectomy case (patient No. 17), 16 out of 17 patients (94.1%) maintained stent patency for a period of 12 months or longer (Tables 2 and 3).
DISCUSSION
Emergency revascularization for an occluded or severely stenotic proximal ICA is recognized as a challenging procedure in acute stroke interventions.101112131415 In patients with acute cerebral infarction due to severe stenosis or occlusion of the proximal ICA, IV rtPA alone has been reported to be less effective, and its morbidity and mortality rates are higher than those of conventional therapy.2627 The occluded segment of the ICA consists predominantly of atherosclerotic plaques and a superimposed thrombus; hence, it does not provide an ideal substrate for thrombolytics alone.2829 The pathophysiologic processes involved in occlusion of the proximal ICA are similar to those observed in acute occlusion of the coronary arteries. In acute myocardial infarction, primary stent placement has provided the best treatment outcomes.30 Previous studies have shown that emergent CAS is effective and relatively safe for the treatment of acute stroke caused by atherosclerotic cervical ICA stenosis or occlusions.101112131415 As far as the authors know, there is no case series about acute CAS only for patients who used IV rtPA. Compared with earlier studies, we also demonstrated successful recanalization (modified TICI ≥ 2b) rate (73.3%) and favorable clinical outcome (mRS 0–2 at 90 days, 57.9%), similar to that of the other studies with ranges from 63–86% and 29.2–72%, respectively. Our study also had lower mortality (5.3%) and incidence of ICH (5.3%) compared to other studies. In particular, the incidence of ICH was 5.3%, similar to rtPA or CAS independently. The risk of ICH with rtPA alone is 6–8%221; the risk of all ICH after CAS in patients with symptomatic carotid stenosis is typically 4.4–5%.3132 This may reflect that all patients arrived at the hospital within 4.5 hours of symptom onset and had a shorter onset to puncture time (mean 190 minutes). Moreover, our study had relatively lower NIHSS scores (Table 4).
Table 4
Previous case series for emergency carotid artery stenting
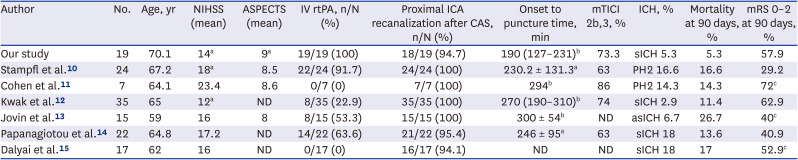
| Author | No. | Age, yr | NIHSS (mean) | ASPECTS (mean) | IV rtPA, n/N (%) | Proximal ICA recanalization after CAS, n/N (%) | Onset to puncture time, min | mTICI 2b,3, % | ICH, % | Mortality at 90 days, % | mRS 0–2 at 90 days, % |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Our study | 19 | 70.1 | 14a | 9a | 19/19 (100) | 18/19 (94.7) | 190 (127–231)b | 73.3 | sICH 5.3 | 5.3 | 57.9 |
| Stampfl et al.10 | 24 | 67.2 | 18a | 8.5 | 22/24 (91.7) | 24/24 (100) | 230.2 ± 131.3a | 63 | PH2 16.6 | 16.6 | 29.2 |
| Cohen et al.11 | 7 | 64.1 | 23.4 | 8.6 | 0/7 (0) | 7/7 (100) | 294b | 86 | PH2 14.3 | 14.3 | 72c |
| Kwak et al.12 | 35 | 65 | 12a | ND | 8/35 (22.9) | 35/35 (100) | 270 (190–310)b | 74 | sICH 2.9 | 11.4 | 62.9 |
| Jovin et al.13 | 15 | 59 | 16 | 8 | 8/15 (53.3) | 15/15 (100) | 300 ± 54b | ND | asICH 6.7 | 26.7 | 40c |
| Papanagiotou et al.14 | 22 | 64.8 | 17.2 | ND | 14/22 (63.6) | 21/22 (95.4) | 246 ± 95a | 63 | sICH 18 | 13.6 | 40.9 |
| Dalyai et al.15 | 17 | 62 | 16 | ND | 0/17 (0) | 16/17 (94.1) | ND | ND | sICH 18 | 17 | 52.9c |
NIHSS = National Institutes of Health Stroke Scale, IV rtPA = intravenous recombinant tissue plasminogen activator, ICA = internal carotid artery, CAS = carotid artery stenting, mTICI = modified TICI, ICH = intracerebral hemorrhage, mRS = modified Rankin Scale, sICH = symptomatic intracerebral hemorrhage, PH = parenchymal hemorrhage, ND = not described, asICH = asymptomatic intracerebral hemorrhage.
aMedian (interquartile range); bmean ± standard deviation; cAt 30 days.
Antithrombotic therapy is required after CAS. Generally, the double antiplatelet regimen is highly recommended before and after CAS in order to prevent stent thrombosis and occlusion.101112131415 Our major concern about the safety of emergent CAS after IV rtPA therapy is that previous systemic thrombolysis might increase the risk of hemorrhagic transformation. Further, it is generally accepted that the administration of any antithrombotic drugs within 24 hours after IV rtPA therapy is contraindicated because of the risk of bleeding complications.28 Relevant evidence for this principle comes from a randomized controlled trial in which IV aspirin was administered after IV thrombolysis.33 This study showed that IV administration of 300 mg aspirin within 90 minutes after the start of IV rtPA did not improve functional outcome at 3 months but increased the risk of hemorrhagic complications. However, this result is limited to the overly rapid administration of IV aspirin (67 ± 25 minutes after IV rtPA). Generally, rtPA is rapidly removed from the plasma, with an initial half-life of less than 5 minutes.34 Thus, the risk of hemorrhage due to rtPA itself can be neglected after several hours. In a retrospective analysis of consecutive ischemic stroke patients, Jeong et al.35 found no increased risk of hemorrhage with early initiation of antiplatelet or anticoagulant therapy (< 24 hours) after IV rtPA compared with initiation > 24 hours. According to the updated American Stroke Association/American Heart Association Guidelines 2018 for the early management of patients with acute ischemic stroke, antithrombotic therapy (other than IV aspirin) within the first 24 hours after treatment with IV rtPA (with or without mechanical thrombectomy) might be considered in the presence of concomitant conditions for which such treatment given in the absence of IV rtPA is known to provide substantial benefit or withholding such treatment is known to cause substantial risk (CLASS of recommendation IIb - weak, Level of evidence B-Nonrandomized).36 Sallustio et al.37 performed a small case series study on the safety and durability of early CAS after IV rtPA for acute ischemic stroke. The authors suggested that CAS may be considered a safe treatment modality after IV rtPA in selected patients at high risk of stroke recurrence due to severe atherosclerosis in the carotid artery. However, they used a different study protocol: CAS was performed at least 24 hours after IV rtPA (with a median onset-to-CAS time of 2.5 days) and dual antiplatelet were administered before CAS and then for 6 weeks; afterward, only a single antiplatelet was prescribed.37 In our study, 13 patients without contraindication were administered antiplatelet agents to prevent stent thrombosis immediately after CAS. The rtPA may be cleared during the endovascular procedure, and it can be assumed that the risk of hemorrhage was not higher when antiplatelet drugs were administered. From a different point of view, although the rtPA has a short half-life, we should consider the downstream effects of rtPA. It can last well over 24 hours and lead to the increased risk of ICH.3334 Additionally, our data provide three-month and twelve-month or longer stent patency. Most of our patients (94.1%) maintained stent patency for a period of 12 months or longer.
Our study had several limitations, such as its retrospective, non-controlled design, and relatively small sample size. Additionally, endovascular treatment modalities varied over the time course of our series. Further prospective and randomized trials are needed to test whether this technique is the best treatment strategy.
In conclusion, we suggest that emergent CAS after IV rtPA therapy for hyperacute stroke caused by atherosclerotic proximal ICA stenosis or occlusion may be feasible and safe with long-term durability.
 XML Download
XML Download