

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Osteoarthritis (OA) is one of the most common chronic diseases, and the knee joint is commonly involved and associated with pain and functional disability.12 Various international and national guidelines for the pain management in OA recommend oral non-steroidal anti-inflammatory drugs (NSAIDs).345 Although pain relief is the goal of OA treatment, there are many concerns about the adverse effects (AEs) of the consistent use of NSAIDs.1 Consequently, the American Geriatric Society recommends that oral NSAIDs should not be prescribed to people over the age of 75.6 The European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis, and Musculoskeletal Diseases recommends the minimum effective dose of NSAIDs for the shortest time required to reduce pain.7 Older patients are more likely to suffer from cardiovascular disease and decline in their renal function with increasing age, which are AEs that are highly associated with the use of NSAIDs. Therefore, the non-surgical management of knee OA from the Osteoarthritis Research Society International (OARCI) suggests that the treatment with non-selective NSAIDs (nsNSAIDs) are suitable for individual OA patients without comorbid condition, but are uncertain for patients with a moderate comorbidity risk and not for patients with a high comorbidity risk.8
NSAIDs are the most widely used medication for OA. More than 50% of patients with OA in the USA,9 and 60% of patients with OA in Europe who use prescription drugs have received NSAIDs.10 In Korea, the regular use of NSAIDs in patients with knee OA had a similar frequency of 48.8%.11 As well as NSAIDs, there was a significant prevalence of prescriptions of opioids, including tramadol, in knee OA (12.2%), although it was lower than overall opioid prescription in other Western countries.12 The OARCI group conditionally recommend duloxetine for knee OA patients with persistent symptoms despite NSAIDs.13 In Korea, the indication of duloxetine was expanded for the treatment of OA unresponsive to NSAIDs in 2016. A recent report on the treatment effect in knee OA suggested that oral NSAIDs, cyclooxygenase-2 (COX-2) inhibitors, and opioids had similar pain control effectiveness.14
Although celecoxib, a selective COX-2 inhibitor, has been developed that theoretically reduces gastrointestinal AEs over nsNSAIDs, the safety of its use remains controversial.15 For patients with gastrointestinal diseases, COX-2 inhibitors are recommended at higher levels than nsNSAIDs.4 Recently, the patent of celecoxib expired in Korea (June 2015) and it is thought to have affected patterns of the initial choice of knee OA treatment. Therefore, we investigated trends in the use of celecoxib as the initial drug for knee OA and changes in the use of other drugs during the same period.
METHODS
Data source and study population
Data source: Health Insurance Review and Assessment (HIRA) claims database
Korea has a universal health insurance system that covers almost 98% of the population. The database of Health Insurance Review and Assessment (HIRA) includes patients’ diagnosis, treatment, procedures, prescription drugs, and health care utilization.16
Study population
Knee OA patients were defined using algorithm of the knee OA diagnostic code (M17) or any OA diagnostic code (M15 to M19) with performance of a knee X-ray based on our pervious validation study.17 After excluding patients with rheumatoid arthritis, ankylosing spondylitis, or psoriatic arthritis, we enrolled patients ≥ 50 years of age with knee OA.
Demographic characteristics, health care utilization related to the initial treatment (type of institution or department), and prescription for medication were evaluated at the index date. Elixhauser comorbidity index18 were evaluated within one year prior to the index date of knee OA, because physician may consider pre-existing comorbidities when prescribing COX-2 inhibitors for knee OA patients (Supplementary Fig. 1).
Medications for knee OA
Our study included medication such as oral NSAIDs, acetaminophen, tramadol, and opioids. We divided oral NSAIDs into 2 groups consisting of nsNSAIDs and COX-2 inhibitors. Well-known symptomatic slow-acting drugs for OA (SYSADOAs) such as diacerein, avocado soybean unsaponifiables, and chondroitin were included in this study, but glucosamine was not included because it was only reimbursed in Korea since 2011. Several herbal drugs that combine herbal extracts were included.11 The uses of oral glucocorticoid (CS) and combined medication for gastrointestinal protection were also investigated.
Furthermore, medication possession ratios (MPRs) were calculated to determine the quantitative use of each different medication. The MPR is calculated with the number of days for which medication is available divided by the number of days of treatment,19 and 50% of MPR was defined as regular use.
Factors for the early use of COX-2 inhibitor
First, we presented the trend of COX-2 inhibitor utilization in patients with knee OA over 3 years between 2013 and 2015. To evaluate the pattern of other medication for knee OA according to a change in COX-2 inhibitor use, we also analyzed the trend of nsNSAIDs, analgesics, or SYSADOA. Next, we performed an analysis to evaluate baseline or clinical factors for the initial use of COX-2 inhibitors.
Statistical analysis
Variables are presented as the mean with standard deviation (SD) for continuous variables and the frequency with percentage for categorical variables. We described the trend of drug utilization in knee OA patients over 3 years with the Cochran–Armitage test for trend P values. A multivariable logistic regression model was constructed to examine factors related to COX-2 inhibitor use. Significant demographic and clinical factors in the crude model were included in the multivariable model. All analyses were performed using SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
The Institutional Review Board (IRB) of our hospital determined that this study was exempt from IRB review because we used existing data and the information could not be linked to individual subjects (HYUH-2016-06-008-002). No informed consent was required from patients due to the nature of public data from NHIS.
RESULTS
Baseline characteristics
We identified 2,857,999 incident knee OA patients between 2013 and 2015 (955,259 in 2013, 981,314 in 2014, and 921,426 in 2015) (Fig. 1). Their mean age ± standard deviation was 64.2 ± 9.8 years. Most patients visited a private clinic (67.7% in 2013 and 68.6% in 2015) or a community hospital (13.4% in 2013 and 14.1% in 2015). More than half of the patients (64.3% in 2013 and 66.8% in 2015) visited an orthopedic surgery department. In terms of comorbidities, percentages of peptic ulcer disease and mild liver disease were similar (22.8% and 20.3% in 2013, 21.0% and 21.2% in 2015, respectively). The mean Elixhauser score was 4.36 ± 1.78 in 2013 and 4.52 ± 6.31 in 2015 (Table 1).
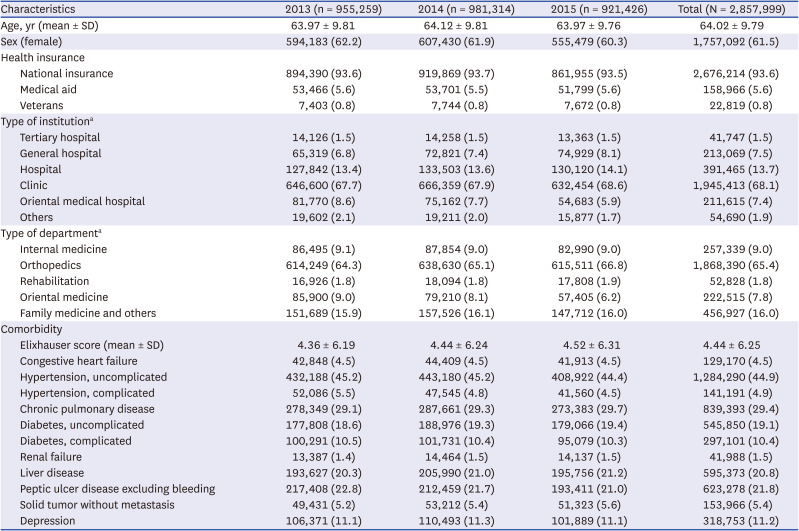
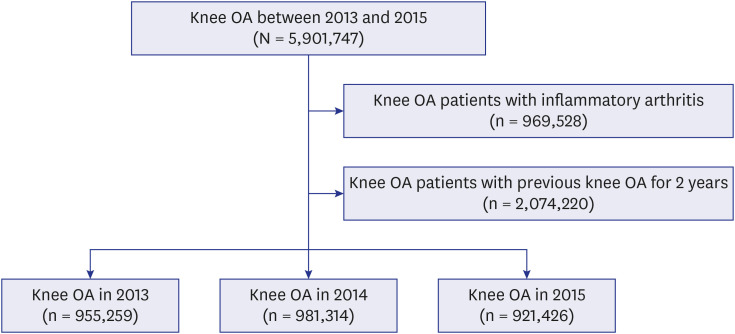
Table 1
Baseline characteristics of the knee OA patients according to year
Values are presented as the number and percentage or mean with standard deviation.
OA = osteoarthritis, SD = standard deviation.
aFrequently visited hospitals are noted.
![]()
Patterns of oral medication for knee OA patients
Among all patients, 19.5% of patients in 2013 and 16.9% in 2015 did not use any medications for knee OA. In the initial prescription for knee OA, the frequency of COX-2 inhibitors as the initial treatment increased from 3.5% in 2013 to 7.2% in 2015 (trend P value < 0.01) (Fig. 2, Table 2). However, the frequencies of nsNSAIDs use or analgesics use did not decrease remarkably. The frequency of nsNSAIDs use (55.3% in 2013 and 56.8% in 2015, trend P value < 0.01) or analgesics use (17.1% in 2013 and 17.3% in 2015, trend P value < 0.01) increased slightly.
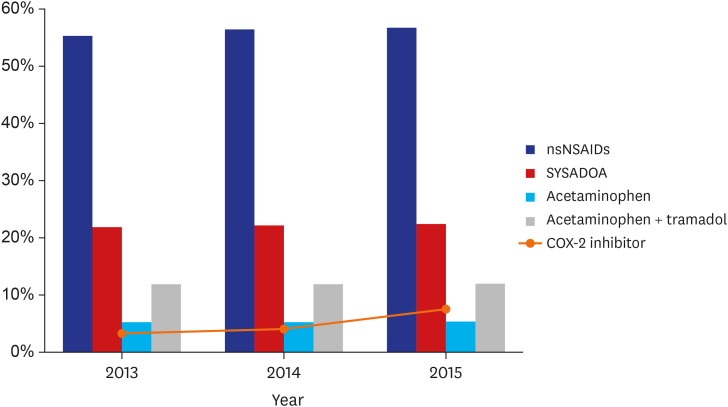
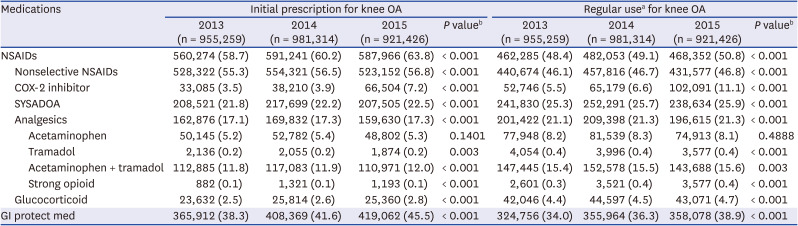
Fig. 2
Trend of initial treatment for knee osteoarthritis between 2013 and 2015.
nsNSAID = non-selective non-steroidal anti-inflammatory drug, SYSADOA = symptomatic slow-acting drug in osteoarthritis, COX = cyclooxygenase.
![]()
Table 2
Trend of drug utilization in incident knee OA patients in the first year after diagnosis
OA = osteoarthritis, NSAID = nonsteroidal anti-inflammatory drug, COX = cyclooxygenase, SYSADOA = symptomatic slow-acting drug in osteoarthritis, GI = gastrointestinal.
aRegular use was defined as a medication possession ratio (MPR) of 50%; bCochran–Armitage test for trend P values.
![]()
A quantitative analysis for drug utilization, defined as regular use (MPR ≥ 50%) was presented for each drug (Table 2). In regular users, COX-2 inhibitor use also rapidly increased from 5.5% in 2013 to 11.1% in 2015 (trend P value < 0.01). However, the frequencies of nsNSAIDs use or analgesics use did not decrease remarkably. The frequency of nsNSAIDs use (46.1% in 2013 and 46.8% in 2015, trend P value < 0.01) or analgesic use (21.1% in 2013 and 21.3% in 2015, trend P value < 0.01) increased slightly (Table 2).
Factors for the early use of COX-2 inhibitors
Baseline characteristics of knee OA patients treated with COX-2 inhibitors as an initial treatment compared with COX-2 inhibitor non-users are presented in the Supplementary Table 1. COX-2 inhibitor users were older than COX-2 inhibitor non-users (71.10 ± 8.98 vs. 63.66 ± 9.70, P < 0.001) and were more likely to be female (65.4% vs. 61.3%, P < 0.001). Patients who visited a private clinic (44.4% vs. 69.0%, P < 0.001) were less likely to be treated with COX-2 inhibitors.
Associated factors for early COX-2 inhibitor use at the early stage of knee OA were older age (odds ratio [OR], 1.08; 95% confidence interval [CI], 1.08–1.08) or female (OR, 1.23; 95% CI, 1.21–1.24). Orthopedic surgeons were more likely to use COX-2 inhibitors than internists (OR, 1.04; 95% CI, 1.02–1.06). National insurance compared with medical aid (OR, 1.17; 95% CI, 1.14–1.19) and tertiary hospitals compared with private clinics (OR, 9.44; 95% CI, 9.17–9.70) were more likely to use COX-2 inhibitors. Combination with other OA medications (SYSADOA [OR, 0.75; 95% CI, 0.74–0.76], analgesics [OR, 0.67; 95% CI, 0.66–0.68], and glucocorticoid [OR, 0.79; 95% CI, 0.76–0.82)] were less likely to use COX-2 inhibitors (Table 3).
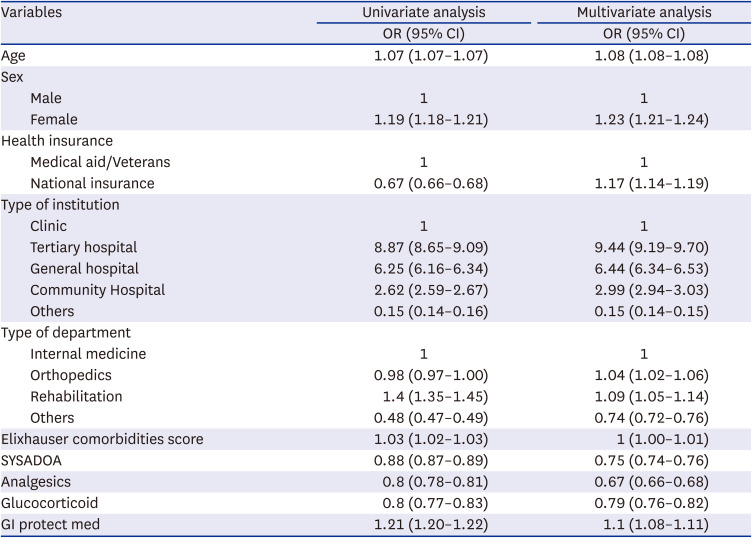
Table 3
Factors for the use of COX 2-inhibitors as an initial treatment
COX = cyclooxygenase, OR = odds ratio, CI = confidence interval, SYSADOA = symptomatic slow-acting drug in osteoarthritis, GI = gastrointestinal.
![]()
DISCUSSION
In Korea, the use of COX-2 inhibitors has rapidly increased as an initial treatment for knee OA patients. However, their use has not reduced the use of nsNSAIDs and analgesics. Old age, female sex, as well as comorbidity were patient factors associated with the early use of COX-2 inhibitors for knee OA. Patients who were treated by an orthopedic surgeon, or who visited a tertiary hospital, or who were supported by national insurance, were more likely to take COX-2 inhibitors.
The increase in COX-2 inhibitor use in knee OA patients may be explained by several factors. First, there is a possibility that the price of COX-2 inhibitors, which are relatively expensive compared with nsNSAIDs, were lowered and their utilization increased as their patents expired. Second, it is possible that pharmaceutical companies actively promoted generic drugs with the expiration of the patents for COX-2 inhibitors. Third, the numbers of patients with gastrointestinal (GI) disorders may have increased leading to an increase in the use of COX-2 inhibitors. Although the prevalence of peptic ulcer disease did not increase over 3 years, the GI protective drugs has increased concurrently.
NSAIDs have potential risk for GI and cardiovascular disease through their action on COX-1 and COX-2 enzymes, and there is an increased risk of developing acute myocardial infarction and heart failure. There is a particularly strong risk of myocardial infarction with COX-2 inhibitors20 because the imbalance between prostacyclin and thromboxane-A2 depends on the relative extents of inhibitors of COX-2 and COX-1.21 COX-2 inhibitors are also associated with an increased risk of upper GI disorders and cardiovascular diseases compared with placebo.22 COX-2 inhibitors as well as nsNSAIDs are also associated with an increased risk of acute kidney injury.23 There is also evidence of an increased all-cause and cardiovascular mortality in patients with OA of lower extremities.24 Increased mortality from GI and cardiovascular disorders was observed, and this may be explained by decreasing physical activity related to OA of lower extremities. Moreover, AEs associated with drugs, particularly NSAIDs, as well as comorbidities such as cardiovascular diseases may also be related with the excess mortality in OA.2425 This increased mortality in OA may be attributed, in part, to treatment strategies that include NSAIDs.26 Furthermore, older patients showed better adherence to NSAIDs.27 Therefore, different strategies to reduce pain in patients with OA should be considered for each individual patient. Moreover, care should be taken about the long-term use of COX-2 inhibitors because they have potent toxicity similar to that of nsNSAIDs.
Old age, female sex, as well as comorbidity based on the Elixhauser comorbidity index were factors associated with the early use of COX-2 inhibitors for knee OA. Patients who were treated by an orthopedic surgeon, or who visited a tertiary hospital, or who were supported by national insurance were more likely to take COX-2 inhibitors. Patients who were treated with SYSADOA, analgesics or glucocorticoids were less likely to take COX-2 inhibitors, whereas patients who were treated with GI protective medication were more likely to take COX-2 inhibitors. Our findings of a rapid increase in the use of COX-2 inhibitors as an early treatment option for knee OA, without any change in use of other drugs, and related factors provide useful evidence to make proper recommendations for NSAIDs use in knee OA patients. A recent study has proposed a clinical model and related factors predicting knee replacement.28 We need further studies to determine whether early treatment with COX-2 inhibitor can reduce the rapid progression of knee OA.
The strength of this study is that it used a nationwide database that covers all drugs prescribed. The Korean insurance system is a single-payer, and the national reimbursement standards apply equally to all health providers. This comprehensive data avoided selection bias and included all NSAID prescriptions in patients with knee OA. Furthermore, we extracted early knee OA patients who initiated medication. Therefore, this study provided information about early COX-2 inhibitor treatment for knee OA patients, which has so far been rarely presented.
There were several limitations in this study. First, we did not find a direct cause, although we found a rapid increase in the use of COX-2 inhibitors for knee OA patients as an initial treatment. Second, we did not evaluate the consequence of the increased use of COX-2 inhibitors. Third, we could not adjust patients’ preferences for treatment choice. In addition, treatment patterns may be changed after surgery, but the effect of knee replacement surgery was not considered. Further long-term studies are required to identify the impact of the increased availability of COX-2 inhibitors as an initial treatment for knee OA patients. In Korea, the reimbursement of COX-2 inhibitors is possible for elderly patients over 60 years of age. The mean age of incident knee OA patients was 64 years old for 3 years. Therefore, it is not appropriate to conclude that patient age has contributed to this rapid change. Further studies using long-term data are needed to determine whether the use of COX-2 inhibitors continues to increase, whether this increase leads to a decrease in nsNSAIDs use, or whether the development of AEs can be reduced by the appropriate stratification of patients.
In conclusion, COX-2 inhibitor use has rapidly increased as an initial treatment for knee OA patients in Korea, but it does not appear to have reduced the use of non-selective NSAIDs and analgesia. Old age, female sex, as well as comorbidity were patient factors associated with the early use of COX-2 inhibitors for knee OA.
 XML Download
XML Download