

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Interleukin-6 (IL-6) plays a key role in inflammatory and immune responses.12 The levels of IL-6 and soluble IL-6 receptors in the serum and synovial fluid of the affected joint are elevated in rheumatoid arthritis (RA) patients and are correlated with disease activities.34 Tocilizumab (TCZ) is a recombinant humanized monoclonal antibody of the IL-6 receptor that inhibits IL-6-mediated signaling.5 TCZ is available as an intravenous (IV) formulation (TCZ-IV) and subcutaneous (SC) formulation (TCZ-SC).6
The route of drug administration is an important factor in the patient’s drug adherence.7 The SC formulation can be self-administered, and many patients prefer the SC formulation over IV administration.89 The dose of TCZ-IV (8 mg/kg) can be increased according to body weight, while the dose of TCZ-SC is fixed at 162 mg once every other week for those weighing less than 100 kg.
Many randomized clinical trials have shown that the effectiveness is maintained even when switching from TCZ-IV to TCZ-SC.101112 However, in real-world practice, it is reported that symptoms worsened in half of RA patients who switched TCZ-IV to TCZ-SC during the recent coronavirus disease 2019 (COVID-19) pandemic.13 Thus, the effect of switching TCZ-SC from TCZ-IV is still controversial. Moreover, overweight was reported to be related to RA flare, but the characteristics of patients with RA flare after switching the TCZ-SC from TCZ-IV have not been evaluated and the risk factors are not well-defined.1014 Furthermore, there were no studies to date have examined the effect of changing back to TCZ-IV on RA flare after switching from TCZ-IV to TCZ-SC. The present study aimed to evaluate the incidence and risk factors for RA flares after switching to TCZ-SC in stable RA patients as TCZ-IV.
Go to : 
METHODS
Study population
In our historical cohort, we analyzed RA patients who had treatment initiation with TCZ treatment between January 2013 and April 2020 at a tertiary referral hospital in Seoul, Korea. Patients with improved RA disease activity evaluated by disease activity score in 28 joints (DAS28) using the erythrocyte sedimentation rate (DAS28-ESR) during the use of TCZ-IV and reaching below low disease activity (DAS28-ESR ≤ 3.2) were included. The exclusion criteria were as follows: 1) patients who started TCZ with SC formulation; 2) patients who discontinued TCZ-IV before 6 months due to loss of follow-up, no efficacy, or adverse events.
TCZ-IV was administered every 4 weeks at a dosage of 8 mg/kg and subsequently 162 mg every two weeks after the TCZ-SC changed. At the time of conversion to TCZ-SC, patients were instructed by a single clinical nurse specialist on the use of TCZ-SC and monitored to ensure that TCZ-SC was injected correctly at every subsequent outpatient visit. Data of the following variables were collected from the electronic medical records: demographic information (sex, age, body mass index [BMI], and body surface area), comorbid diseases (hypertension, diabetes mellitus, and interstitial lung disease), TCZ dosage, previous biologic diseases modifying anti-rheumatic drug exposure, concomitant methotrexate (MTX), use of corticosteroids and daily dosage, DAS28-ESR score, and baseline laboratory data (white blood cells, hemoglobin, platelet counts, ESR, and C-reactive protein).
The primary outcome of interest was the incidence of RA flare after switching TCZ-SC from TCZ-IV. RA flare was defined as an increase in the DAS28-ESR > 1.215 within 6 months after switching from TCZ-IV to TCZ-SC.12 We defined “SC ineffective group” as patients with RA flare and “SC effective group” as patients with stable RA after TCZ-SC switched.
Statistical analysis
The χ2 test or Fisher’s exact test was used to compare categorical data. Continuous values are expressed as means (standard deviations) or as median (interquartile range) and were calculated using Student’s t-test for parametric data or the Mann-Whitney U test for nonparametric data. Logistic regression analysis with a stepwise backward elimination procedure was performed to identify risk factors for RA flare after switching TCZ from IV to SC and reported as odds ratio (OR) and 95% confidence intervals (CIs). Variable that had a P value of < 0.1 on univariable analysis were selected for multivariable analysis. Statistical significance was set at P < 0.05. All statistical analyses were performed in IBM SPSS, version 21.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
This study was approved by the Institutional Review Board of Asan Medical Center, Seoul, Korea (approval No. 2021-0742). The requirement for informed consent was waived due to the retrospective design of this study.
Go to :
RESULTS
Clinical characteristics of the study population
As shown in Fig. 1, TCZ was initiated in 229 patients with RA, of whom 135 patients started the treatment with TCZ-IV. Of them, 29 patients were excluded due to follow-up loss or discontinuation of treatment within 6 months of initiation. Finally, 106 patients were included in the analysis, of whom 69 maintained TCZ-IV treatment without switching to TCZ-SC and 37 switched to TCZ-SC upon remission or low disease activity assessed by the DAS28-ESR according to their preference, and after discussion with attending physicians.
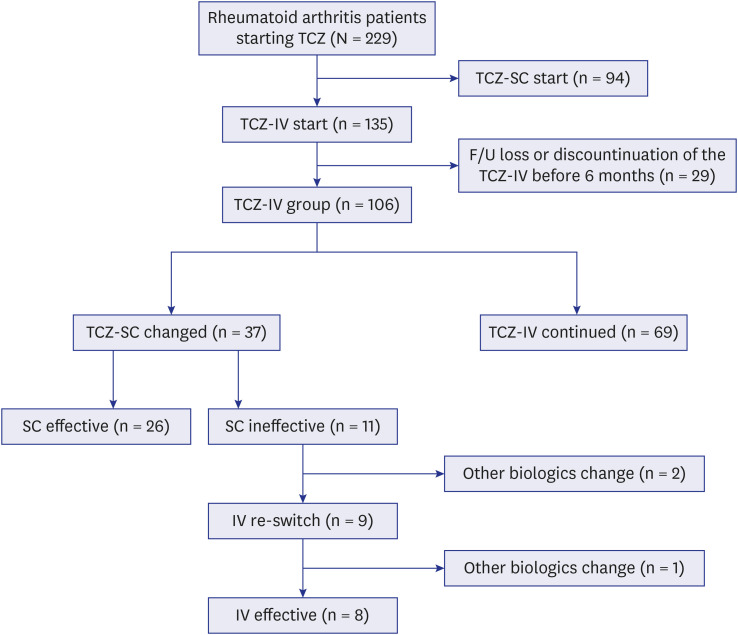
There were 11 (29.7%) patients who experienced RA flare after switching to TCZ-SC (SC ineffective group), and the remaining 26 (70.3%) patients maintained the activity of RA stably even after switching to TCZ-SC (SC effective group). Nine patients in the SC ineffective group were re-administered TCZ-IV, and 8 patients except one acquired low disease activity again within 6 months of re-administration.
Table 1 was compared the clinical characteristics between TCZ-SC changed group and TCZ-IV continued group. The DAS28-ESR score was lower in the TCZ-SC changed group (measured at switching) than in the TCZ-IV continued group (measured at 6 months after initiation) (2.26 vs. 2.69, P = 0.008). All patients had significant improvement in disease activity at follow-up (decrease of DAS28-ESR 1.2 or greater), with none of the patients in the TCZ-SC changed group showing disease activity higher than low disease activity; however, 36.2% of patients in the TCZ-IV continued group had moderate disease activity.

Table 1
Clinical characteristics of TCZ-SC changed group vs. TCZ-IV continued group
Values are presented as mean ± standard deviation, median (interquartile range) or number (%).
TCZ = tocilizumab, SC = subcutaneous, IV = intravenous, BMI = body mass index, MTX = methotrexate, DAS28 = disease activity score in 28 joints, ESR = erythrocyte sedimentation rate, RA = rheumatoid arthritis.
aCalculated only among the patients who used those medications.
bThe DAS28-ERS score was measured at the time of switch in the TCZ-SC changed group and at 6 months after TCZ initiation in TCZ-IV continued group.
Statistically significant P values were marked with asterisks (*P < 0.05, **P < 0.01, ***P < 0.001).
![]()
The baseline characteristics of TCZ-SC changed patients are shown in Table 2. The mean age was 58.7 years and 32 (86.5%) patients were female. All patients were positive for rheumatoid factor or anti-cyclic citrullinated peptide antibody. The median duration of the use of TCZ as an IV formulation before switching to the SC formulation was 9 months in the SC ineffective group and 13.5 months in the SC effective group. At the time of RA flare in the SC ineffective group and 6 months after SC switch in SC effective group, the mean DAS28-ESR score was significantly higher in the SC ineffective group (5.0 vs. 1.7, P < 0.001). The TCZ dose per body weight at SC change was significantly higher in the SC ineffective group than in the SC effective group (8.2 mg/kg vs. 7.7 mg/kg, P = 0.001). The proportion of patients using concomitant MTX at the TCZ-SC change was significantly higher in the SC effective group than in the SC ineffective group (84.6% vs. 45.5%, P = 0.038). There was no difference in the number of exposures to the previous biological agents. There were no significant differences between the two groups with regard to age, comorbidities, BMI and, baseline DAS28-ESR. The mean time interval between the TCZ-SC transition and RA flares in the SC ineffective group was 3.2 months. More than half (6/11 [54.5%]) of the patients in the SC ineffective group developed an RA flare within 2 months after SC switching. These six patients had significantly higher DAS28-ESR scores at the time of switch compared with the SC effective group (2.80 vs. 2.17, P = 0.018).
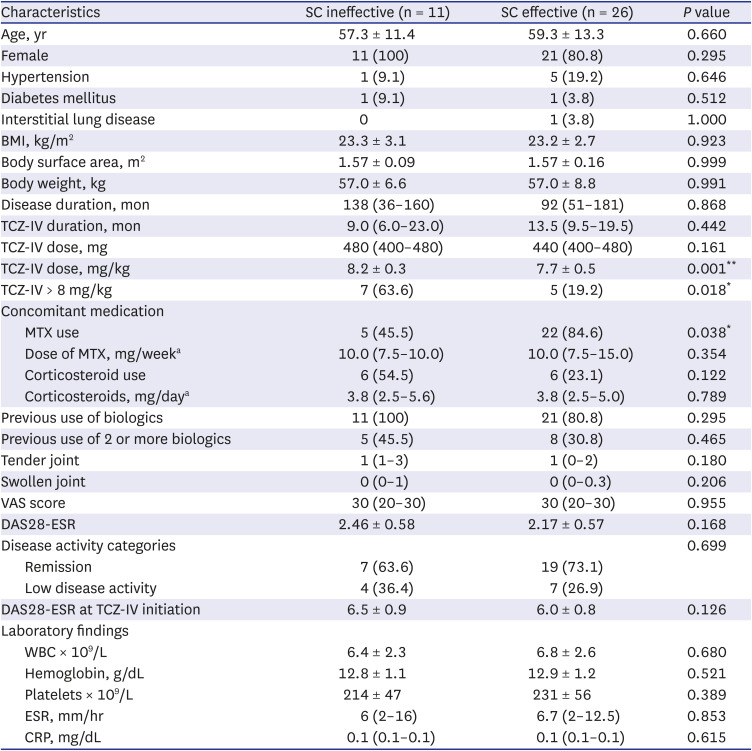
Table 2
Clinical characteristics of the study patients (n = 37) with rheumatoid arthritis at the time of switching from TCZ-IV to TCZ-SC
Values are presented as mean ± standard deviation, median (interquartile range) or number (%).
IV = intravenous, SC = subcutaneous, BMI = body mass index, TCZ = tocilizumab, MTX = methotrexate, DAS28 = disease activity score in 28 joints, ESR = erythrocyte sedimentation rate, VAS = visual analog scale, WBC = white blood cell, CRP = C-reactive protein.
aCalculated only among the patients who used those medications.
Statistically significant P values were marked with asterisks (*P < 0.05, **P < 0.01).
![]()
Clinical factors associated with RA flare in patients who switched TCZ from IV to SC formulation
The results of the logistic regression analysis for factors associated with RA flares after switching TCZ from IV to SC are presented in Table 3. The results of the univariable analysis showed that the dose per weight of TCZ-IV at switching, MTX non-use, and steroid use were associated with an increased risk of RA flares after switching from TCZ-IV to TCZ-SC. Obesity and previous use of 2 or more biologics were not associated with the risk of RA flare in TCZ-SC switched from TCZ-IV. Multivariable analysis revealed that the dose per weight of TCZ-IV at switching (OR, 20.70; 95% CI, 2.22–192.84; P = 0.008) and MTX non-use (OR, 8.53; 95% CI, 1.21–60.40; P = 0.032) were significantly associated with an increased risk of RA flare events.
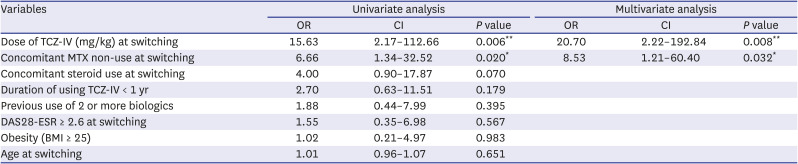
Table 3
Factors associated with rheumatoid arthritis flare after switching from TCZ-IV to TCZ-SC
TCZ = tocilizumab, IV = intravenous, SC = subcutaneous, MTX = methotrexate, DAS28 = disease activity score in 28 joints, ESR = erythrocyte sedimentation rate, BMI = body mass index, OR = odds ratio, CI = confidence interval.
Statistically significant P values were marked with asterisks (*P < 0.05, **P < 0.01).
![]()
Go to :
DISCUSSION
The present study showed RA flares in patients after switching from TCZ-IV to TCZ-SC frequently, with a crude rate of 29.7% (11/37). Notably, we also found that at the time of switching to TCZ-SC, high dose of TCZ-IV and concomitant MTX non-use was significantly associated with an RA flare after SC switching.
TCZ is widely used in the treatment of RA, juvenile idiopathic arthritis, giant cell arteritis and cytokine release syndrome.16 The recommended initial dosage for TCZ-IV in RA patients differs in the European Union (EU) and the United States.17 The recommended initial dosage of TCZ-IV is 8 mg/kg every 4 weeks in the EU, whereas a starting dosage of 4 mg/kg every 4 weeks followed by an increase to 8 mg/kg every 4 weeks based on clinical response is recommended in the United States.17 In the present study, according to EU standards, TCZ-IV was started at 8 mg/kg and the average dose per body weight of TCZ at the time of SC change actually used was 7.8 mg/kg, which was higher in the SC ineffective group than in the SC effective group (8.2 mg/kg vs. 7.7 mg/kg, P = 0.001). However, when TCZ was changed to a SC formulation, the DAS28-ESR and disease activity categories assessed by DAS28-ESR did not differ between the two groups. Therefore, higher dose of TCZ-IV required to stably maintain the RA activity is considered as a risk factor for the flare after TCZ-SC change. Especially, patients who are being treated with > 8 mg/kg of TCZ-IV should consider the risk of flare when switching from TCZ-IV to TCZ-SC.
Many randomized clinical trials have shown that the effectiveness is maintained even after switching TCZ from IV to SC formulation.101112 However, looking at the subgroup, switching to TCZ-SC in patients with RA remission with TCZ-IV worsens the RA by 22%.10 Also, there are two real-world studies that the effect was maintained after switching from TCZ-IV to TCZ-SC, but one study include patients who used 4 mg/kg in TCZ-IV dose and another study used 8 mg/kg, but the actual dose was not described.1418 In addition, in a small study of RA patients that switched TCZ-IV to TCZ-SC during the recent COVID-19 pandemic, almost half (7 out of 16) of the patients had worsening symptoms after 3 months and most patients (14 out of 16) wanted to re-change to TCZ-IV.13 In a previous study, obesity (BMI ≥ 25 kg/m2) or high body weight (more than 60 kg or 70 kg) has been reported as a factor associated with RA flare after switching from TCZ-IV to TCZ-SC.1014 In our study, RA flare occurred in 11 (29.7%) of 37 patients who switched TCZ from IV to SC formulation, and overweight or obesity was not associated with the worsening of RA activity. Notably, eight of nine (88.9%) patients whose RA flare after switching TCZ-SC had improved RA activity after re-switching to the TCZ-IV. Our data suggest that TCZ-IV controls RA activity more effectively in these patients than TCZ-SC.
The results of several reports comparing the efficacy of TCZ monotherapy and TCZ combination with MTX in RA are controversial. Many studies have shown that there is no significant difference in the clinical or radiologic response between TCZ alone and MTX combination therapy in RA.192021 By contrast, other studies have reported that the combination of TCZ and MTX is clinically and radiographically superior to TCZ monotherapy and is important in achieving remission.2223 In this present study, MTX non-using was significantly associated with RA flares after TCZ-SC change. These findings cautiously suggest that when switching from TCZ-IV to TCZ-SC, the concomitant use of MTX is may be beneficial for sustaining the drug efficacy.
The present study had some limitations. First, this study may have been affected by a selection bias inherent to its retrospective and single-center cohort design. Second, the number of patients who switched from TCZ-IV to TCZ-SC in this study was small, resulting in a wide range of CIs and ORs. Therefore, multicenter research with more patients is required. Third, all patients were prescribed TCZ-IV based on 8 mg per body weight; however, the infused dosage per body weight may not be administered in the same manner because the unit of vial was produced only in 80 mg, 200 mg, and 400 mg doses, respectively. Despite these limitations, this is the first real-world study investigating the factors that are associated with RA flares after switching TCZ from IV formulation to SC formulation and whether the effectiveness of TCZ is maintained after re-switching to the TCZ-IV.
In conclusion, our study showed that RA flares occasionally occur after switching from TCZ-IV to TCZ-SC. RA patients treated with a high dose of TCZ or concomitant MTX non-user might experience RA flares after switching from TCZ-IV to TCZ-SC; thus, it is necessary to consider these factors when switching to TCZ-SC.
Go to :
 XML Download
XML Download