

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epidural block (EB) is an effective and popular treatment modality for acute lumbar radicular pain, even though the long-term efficacy of this modality remains controversial.1234 Lumbar EBs are performed via several routes, including transforaminal, caudal, and interlaminar approaches. Among these, transforaminal epidural block (TFEB) has the advantages of being target-specific and fulfilling the aim of reaching the primary site of disc pathology, i.e., the ventral epidural space.56
A recent review states that the efficacy of TFEBs with steroids for treating radicular pain from lumbar disc herniation (LDH) is supported by strong evidence.7 Moreover, in a recent systematic review and meta-analysis, the efficacy of TFEBs with steroids for radicular pain from LDH is supported by level I evidence, whereas the evidence is rated as level II for lumbar TFEBs without steroids.8
However, EBs with steroids can cause complications, including Cushing syndrome, loss of bone density, infection, and hyperglycemia.9 Moreover, although no large prospective studies have investigated the immune response to coronavirus disease 2019 (COVID-19) vaccines after steroid injections, it is reasonable to delay procedures involving steroids for approximately 1 to 2 weeks after vaccine administration and to delay vaccinations for approximately 2 weeks after a procedure involving steroids.10
In a study by Rabinovitch et al.,11 the relief of radicular and low back pain has a positive correlation with the injectate volume. The injectate displaces the dura forward and inward in addition to stretching the nerve. These effects can lead to the lysis of neural adhesions.11 Chun et al.12 found that the injectate volume may be one of the most important factors determining the effectiveness of lumbar TFEBs with steroids and that 8 mL of injectate was more effective than 3 mL. The higher injectate volume might enhance the efficacy of TFEBs with steroids.
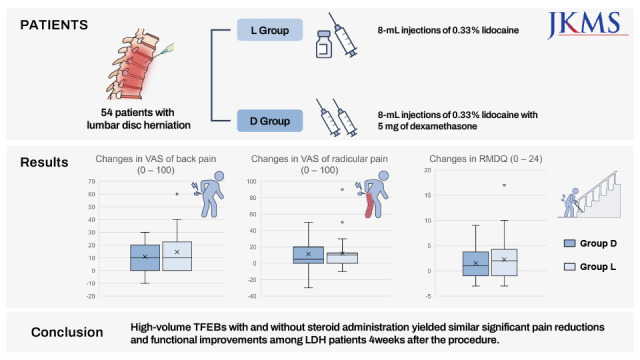
To the best of our knowledge, no controlled trials have compared the efficacy of high-volume TFEBs with vs. without steroids in LDH. We hypothesized that high-volume TFEBs without steroids effectively alleviate axial back and radicular pain associated with LDH. Therefore, this study compared the clinical effects of high-volume TFEBs with vs. without steroids for managing axial lumbar and radicular pain secondary to LDH.
Go to : 
METHODS
Study design and participants
This randomized, double-blind, controlled, parallel-group clinical trial was registered in the Clinical Research Information Service (CRIS, http://cris.nih.go.kr, number: KCT0005446). We included patients diagnosed with LDH at a single pain management center between June 2018 and April 2021.
The inclusion criteria were: (A) presence of axial back or radicular pain with a pain intensity ≥ 40/100 according to a visual analog scale (VAS), (B) age ≥ 18 years diagnosed with LDH after a series of neurologic and magnetic resonance (MR) examinations, and (C) need for single-level TFEBs. The exclusion criteria were: (A) long-term oral steroid treatment; (B) pregnancy; (C) cognitive impairment; (D) any condition that increased the risk of complications, such as bleeding diathesis, allergies to specific medications (contrast medium and local anesthetics [LAs], etc.), and infection; (E) motor grade less than 4; (F) bilateral symptoms; (G) prior therapeutic TFEBs in the previous 6 months; (H) prior surgery; (I) spinal stenosis; and (J) spondylolisthesis.
Procedures
Each patient was positioned in the prone position with a pillow under the abdomen above the iliac crest to reduce lumbar lordosis, prepared for the injection, and draped using sterile technique. Vital signs were monitored. An obliquely tilted C-arm was rotated toward the lesion site by 15–25 degrees, and the axial rotation was adjusted cephalocaudally. Then, a 22-gauge 5-inch spinal needle was guided inferolaterally to the pars interarticularis and into the intervertebral foramen. With biplanar visualization, the needle was advanced into the “safety triangle,” which was inferior to the pedicle and superolateral to the exiting spinal nerve. In the lateral projection, needle placement was confirmed with the needle tip just dorsal to the posterior margin of the vertebral body. About 1 mL of contrast medium was injected with real-time imaging guidance to confirm ventral epidural spread without intravascular, subarachnoid, or extra-epidural uptake. Patients in group D received 8-mL injections of 0.33% lidocaine with 5 mg of dexamethasone disodium phosphate. Patients in group L received 8-mL injections of 0.33% lidocaine.
Outcome measures
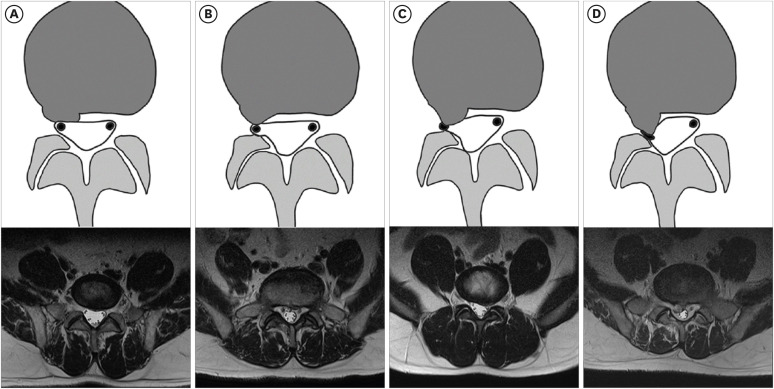
The patients’ age, sex, height, weight, duration of symptoms, site and level of injections, and radiologic features were recorded. The radiologic features of disc displacement at the level and side of the nerve root affected were assessed based on the classification system described by Fardon et al.,13 and the severity of nerve root compression was assessed using a modified version of the system described by Ghahreman and Bogduk14 In this system, Grade I refers to when the disc simply contacts the nerve root, Grade II refers to when the nerve root is displaced but with preservation of the periradicular cerebrospinal fluid or fat, Grade III refers to when the periradicular cerebrospinal fluid or fat is obliterated, and Grade IV refers to when the nerve root is morphologically distorted (Fig. 1). MR images were reviewed independently by a radiologist and a pain specialist, each blinded to the patients’ responses to treatment.
The primary outcome measure for this study was reduction of pain at 4 weeks after the procedure. To minimize recall bias, current back and lumbosacral radicular pain was assessed using a continuous VAS (mm scale, range 0–100; 0 = “no pain,” 100 = “worst imaginable pain”) at baseline and 4 weeks.15 Patients were asked to select a point on a line drawn between two points to express their perceptions of pain intensity.16
The secondary outcomes included the reduction of functional disability at 4 weeks after the procedure, pain scores during injection (procedural pain score), and adverse effects. Functional disability reductions were evaluated using the Korean version of the Roland-Morris Disability Questionnaire (RMDQ, range 0–24).17 The RMDQ consists of 24 items representing “physical functions that were likely to be affected by low back pain”; each item can be checked if it applies to a patient for that day, leading to a total score that is obtained by counting the number of checked items.18 The procedural pain scores reflected pain intensity during drug injection, and patients were asked to indicate their current pain scores immediately after injection.
Randomization and blinding
A total of 54 patients were enrolled and randomly assigned to either group D or group L. The random numbers were kept in sealed envelopes and were opened by an anesthesiologist not involved in this study. Sterile syringes containing lidocaine with dexamethasone or lidocaine only were prepared in a double-blind fashion by a pain nurse not involved in the management of the study patients. The patients were randomly assigned (1:1) into group D or group L. All of the procedures were performed by the corresponding author (KWJ), who was blinded to the type of administered treatment.
Statistical analysis
Power analysis was performed for sample size estimation to test the feasibility of the study using G*Power 3.1 (Heinrich Heine University, Düsseldorf, Germany). The calculation was based on data from a previous study.19 We hypothesized that the pain reduction associated with high-volume TFEB without steroids would be similar to that associated with high-volume TFEB with steroids (decrease in the VAS score from 4.73 ± 2.15 to 3.3 ± 2.45).19 A total of 54 patients (27 per group, dropout rate: 10%) was required, with a power of 0.80 and an α value of 0.05.
The normality of the distribution of continuous variables was evaluated by the Shapiro-Wilk test. Primary outcomes were analyzed with an independent t-test or the Mann-Whitney U-test for between-group analysis and the Wilcoxon signature rank test for within-group analysis. The secondary outcomes were analyzed in the same manner as the primary outcomes. Descriptive variables were evaluated using the χ2 test. Values of P < 0.05 were considered statistically significant. All statistical analyses were performed using PASW Statistics for Windows, version 18 (SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board of Ewha Womans University Hospital (EUMC 2018-05-028-011). Written informed consent was obtained from each participant before enrollment. The study complied with the Declaration of Helsinki.
Go to :
RESULTS
Between June 2018 and April 2021, the 54 patients who visited the pain management center were randomized into group D and group L. One patient did not meet the inclusion criteria, and three patients in group D and one patient in group L were lost in the follow-up. Consequently, 24 patients remained in group D, and 26 patients remained in group L. There were no missing data at 4 weeks after treatment (Fig. 2). No significant differences in the demographic data were founded between the groups (Table 1).
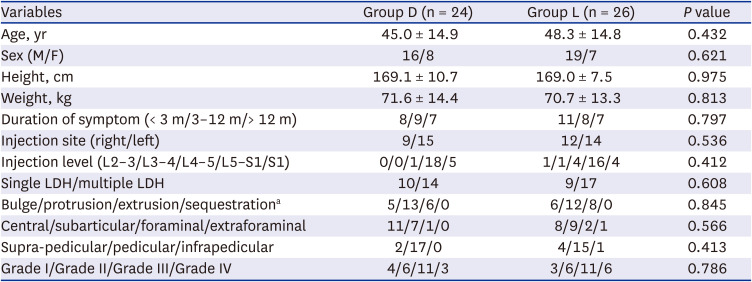
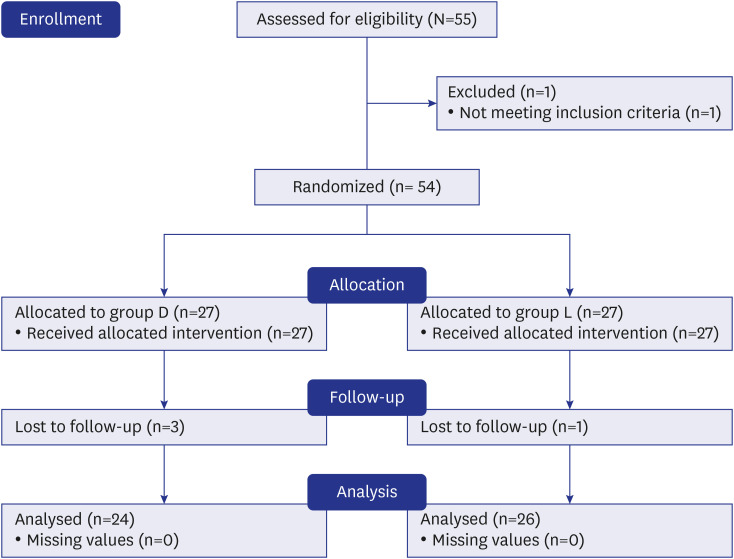
Table 1
Demographic data
Data are expressed as the mean ± standard deviation or number of patients.
aThe degree of disc displacement was assessed based on the classification system described by Fardon et al.13: Bulge – generalized displacement of disc material (> 50% or > 180° of disc circumference) beyond the limits of the intervertebral disc space; Herniation–localized displacement of disc material (< 50% or < 180°) beyond the limits of the intervertebral disc space; Protrusion–fragment does not have a neck that is narrower than the fragment in any dimension; Extrusion–fragment has a neck that is narrower than the fragment in at least one dimension; Sequestration–a type of disc extrusion that has lost continuity with the disc origin.
LDH = lumbar disc herniation.
![]()
Regarding the primary outcome, there were no significant differences in baseline VAS scores for back and radicular pain between the two groups, with no significant differences at 4 weeks after treatment (Table 2). At 4 weeks after the procedure, both groups demonstrated statistically significant improvements in back and radicular pain according to VAS scores (P < 0.05), with no significant differences between the two groups (Table 3).
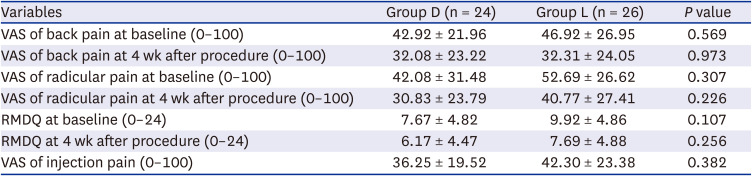

Table 2
Pain scores, functional disability, and injection pain
Data are expressed as the mean ± standard deviation.
VAS = visual analog scale, RMDQ = Roland-Morris Disability Questionnaire.
![]()
Table 3
Pain relief and reduction of functional disability
Data are expressed as the median (interquartile range).
VAS = visual analog scale, RMDQ = Roland-Morris Disability Questionnaire.
![]()
In terms of functional disability and pain scores during injection, there were also no significant differences in RMDQ scores between the two groups, with no significant differences at 4 weeks after treatment (Table 2). At 4 weeks after the procedure, both groups demonstrated statistically significant improvements in functional status according to RMDQ scores (P < 0.05), with no significant differences between the two groups (Table 3). Pain scores during injection were not significantly different between the two groups (Table 2). In group L, two patients complained of severe pain on injection, which was resolved immediately after the injection.
In terms of safety, no severe adverse events were reported in this study. Specifically, no dural punctures were observed in either group (no subdural or intrathecal injections). No patients in either group sustained any infectious complications, postdural puncture cephalalgia, persistent paresthesias, systemic steroid reactions, skin lesions, or any adverse reaction to contrast media or adjuvant medications.
Go to :
DISCUSSION
Our study showed that both group D and group L demonstrated significant reductions in back and radicular pain according to VAS scores and improved functional status according to RMDQ scores at 4 weeks after treatment. Furthermore, no significant differences were observed between the two groups in terms of pain reduction or functional status.
Although several studies of the efficacy of EBs with steroids for treating lumbosacral radicular pain have provided inconsistent results, recent review articles have reported that EBs with steroids are more effective for LDH than for lumbar spinal stenosis (LSS)7 and that steroid administration in conjunction with TFEBs is more effective than LAs alone for treating LDH.682021 However, in our study, compared with TFEBs with steroids, high-volume TFEBs without steroids yielded no significant difference in pain reduction or functional disability improvement at 4 weeks after treatment.
According to a review article by Smith et al.,7 for patients with LDH, using the criterion of ≥ 50% reduction in pain, success rates across the included studies were 63% at 1 month, 74% at 3 months, 64% at 6 months, and 64% at 1 year. For patients with LSS, success rates across the included studies were 49% at 1 month, 48% at 3 months, 43% at 6 months, and 59% at 1 year. Smith et al.7 concluded that there is strong evidence indicating that TFEB with steroids is an effective treatment approach for radicular pain due to LDH; however, there is a lack of high-quality evidence demonstrating its effectiveness for treating radicular pain due to LSS.
A systematic review and meta-analysis of eight randomized controlled trials (RCTs) that recorded the pain scores of patients with LDH demonstrated a significant but clinically modest reduction in mean pain scores among patients receiving TFEBs with steroids compared with TFEBs with LAs/saline at a median duration of 3 months after the intervention.20 Another recent systematic review and meta-analysis evaluating the effectiveness of TFEBs in LDH management also reported that there is level I evidence supporting the use of LAs and steroids, whereas the evidence is level II for LAs alone.8 Similarly, for TFEBs, there is good evidence supporting LAs and steroids and fair evidence supporting the use of LAs only for radiculitis secondary to LDH.6
A previous RCT compared the outcomes associated with TFEBs with steroids and LAs vs. LAs alone vs. normal saline at 1 month after treatment among patients with LDH.22 A significantly greater proportion of patients treated with TFEBs with steroids (54%) achieved pain relief than did patients treated with TFEBs with LAs (7%) or saline (19%). Pain relief was accompanied by significant functional improvements.22 This was inconsistent with the results of our study; however, a difference with our study was that the investigators used a lower dose (2 mL) of injectate.
Corticosteroids inhibit the vasodilatory effects associated with inflammation, decrease vascular permeability caused by inflammatory insults, and decrease leukocyte emigration to the site of injury.23 In response to injury, corticosteroids affect the transcription of various genes in leukocytes, resulting in immunosuppression and anti-inflammation.23 Although existing data suggest there is significant individual variability in the amount of systemic absorption of locally injected corticosteroids, it is clear that EBs with steroids can have systemic effects for weeks and that complications may be associated with their use, including Cushing syndrome, loss of bone density, infection, and hyperglycemia.9 Therefore, EBs with steroids should be performed with consideration of complications, especially for highly risky patients, such as postmenopausal women, people with diabetes, and those considering surgery in the near future.9
In the COVID-19 era, with most patients being vaccinated against COVID-19, the Spine Intervention Society recommends withholding steroid injections no less than 2 weeks prior to COVID-19 vaccination and no less than 1 week following vaccination.10 Injected steroids can be taken up in the systemic circulation via diffusion and potentially alter the immune response to vaccinations, rendering them less effective.24 Therefore, for treating LDH-associated pain, high-volume TFEBs without steroids can be considered for patients at high risk of complications from steroid injections or if they have recently received or plan to receive a COVID-19 vaccine and have persistent pain despite conservative treatment.
The effect of mechanical compression caused by LDH and chemical irritation of the nerve root from the leakage of disc materials is well documented in various studies.25 Various chemical mediators have been shown to induce ectopic firing.2627 Both phospholipase A2 and prostaglandin E2 have received significant attention in the development of clinically meaningful radiculopathy.28 It is believed that the achieved neural blockade alters or interrupts nociceptive input, reflex mechanisms of the afferent fibers, the self-sustaining activity of the neurons, and the pattern of central neuronal activities.29 LAs have been described to provide short- to long-term symptomatic relief through the alteration of various mechanisms, including excess nociceptive processes, excess release of neurotransmitters, nociceptive sensitization of the nervous system, and phenotype changes.3031 Experimental evidence has demonstrated the prolonged effect of epidural ropivacaine in a rat model of neuropathic pain31 and a lack of additional benefit in nerve root infiltration for LDH with the addition of corticosteroids.32
The effects of TFEBs appear to be influenced by the volume of the injected material. Rabinovitch et al.11 found a positive correlation between the fluid injection volume into the epidural space and the relief of radicular pain. It has been suggested that high-volume TFEBs wash out inflammatory cytokines from the affected area. Furthermore, the increased volume facilitates lavage of the epidural space, suppression of ectopic discharge from the injured nerve, and enhancement of blood flow to the ischemic nerve roots.12
It is difficult to explain the exact mechanism explaining our results, and several articles reporting on the role of steroids in TFEBs have provided discordant conclusions.8 However, we thought that increasing the volume of LAs can effectively eliminate various chemical mediators, including inflammatory cytokines, and inhibit ectopic discharge caused by LDH,3334 resulting in similar pain reductions and functional improvements to those achieved with steroids. Some studies of TFEBs using lidocaine have yielded results concordant with ours; pain reduction and improvement of functional disability were similar in both groups: those receiving lidocaine alone and lidocaine with steroids.3536 However, Riew et al.37 found bupivacaine with steroids to be associated with significantly superior effects over bupivacaine alone.
In our study, two patients complained of severe pain on injection, but the pain resolved immediately in both patients. A direct correlation between the volume of anesthetic injected and epidural pressure has been reported.3839 However, Paul and Wildsmith40 found similar epidural pressures with different injection volumes. Therefore, ensuring good runoff during injection is important to prevent volume-related increases in the local pressure, and the decision of when to incorporate high-volume TFEBs in patient care should be made at the physician’s discretion.
In terms of radiographic findings, there is little convincing evidence as to whether MR findings of disc pathology can predict outcomes of lumbar TFEBs with steroids.7 Ghahreman and Bogduk14 found that the success rate of TFEBs with steroids for patients with low-grade compression LDH was 75%; however, the rate was 26% for patients with high-grade compression LDH. On the other hand, Maus et al.41 demonstrated that patients with high-grade compression (grade III) responded to lumbar TFEBs with steroids most often, followed by patients with grade II, grade IV, and grade I. In our study, there was no significant difference in grade of LDH-associated compression between the two groups.
This study had several limitations. First, we did not examine long-term outcomes, but short-term effects are also meaningful. In the majority of patients, LDH will regress over time, and the symptoms can resolve by 12 weeks without any treatment.42 Moreover, a study found that the responders had significantly improved lower leg pain and less disability at 24 months compared with the non-responders starting from the second week, with the best discrimination at the 1-month or 3-month follow-up points after TFEBs in patients with LDH.43 Second, we enrolled a relatively small number of patients, and the sample size may have been insufficient to determine differences in meaningful pain relief and functional disability between the groups. Third, we focused on the RMDQ only. The Oswestry Disability Index may be better for detecting functional changes in patients with more severe disability, whereas the RMDQ may be more appropriate for patients with minor disability.44 Fourth, we used lidocaine, but different results can be obtained with TFEBs using other LAs. Fifth, spontaneous improvement in back and radicular pain over time was a potential cause of bias, which may have led us to overestimate the benefits of TFEBs; loss to follow-up was another potential source of bias.
In conclusion, compared with TFEBs with steroids, high-volume TFEBs were associated with similar significant pain reductions and functional improvements, among patients with LDH, even without steroids. However, further studies—including large, multicenter RCTs—are warranted to evaluate long-term outcomes associated with high-volume TFEBs without steroids for treating axial back pain and radicular pain associated with LDH.
Go to :
 XML Download
XML Download