

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first case of coronavirus disease 2019 (COVID-19) was reported from Wuhan, China, more than 450 million confirmed COVID-19 cases have been reported worldwide on 12 March 2022.1 A significant number of patients were reported to experience COVID-19-related complications,2 and secondary infection is one of the most common complications.34
The association between respiratory virus infections and subsequent invasive fungal infections, such as pulmonary aspergillosis, has been raised.56 The risk of pulmonary aspergillosis among influenza patients was relatively well-documented in serial studies.57 A similar association has been observed in critically ill COVID-19 patients.3891011 Several factors associated with COVID-19-associated pulmonary aspergillosis (CAPA) have been reported, including old age, invasive respiratory support, chronic pulmonary disease, and receiving tocilizumab.910111213 Meanwhile, a corticosteroid is one of the most important treatments for COVID-19 patients requiring oxygen therapy.14 Corticosteroids could suppress the hyper-inflammation syndrome caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection; however, concerns for the risk of secondary infections are also expected due to possible over-immunosuppression.15 The usual recommended dose for COVID-19 patients requiring oxygen therapy is 6 mg of dexamethasone daily for 10 days or until discharge.1416 However, a longer and/or higher-dose corticosteroid regimen has been prescribed for refractory COVID-19-related acute respiratory distress syndrome.1718
In this regard, we evaluated risk factors for CAPA among critically ill COVID-19 patients and compared their clinical outcomes with those of patients without CAPA.
METHODS
Study design and population
This was a nationwide, multicenter, retrospective cohort study in patients with laboratory-confirmed SARS-CoV-2 virus infection from the Republic of Korea. A total of 13 academic hospitals (11 tertiary hospitals and 2 secondary hospitals, ranging from 300 to 2715 beds) participated in this study. Among 13 participating hospitals, 5 hospitals reported patients with CAPA (Supplementary Table 1). Patients who were admitted to an intensive care unit (ICU) between July 2020 and March 2021 and satisfied the following criteria were collected: 1) adult (≥ 18 years old) patients, 2) patients requiring respiratory support, and 3) patients who survived and were admitted ≥ 10 days after ICU admission. By including only those who survived and were admitted more than 10 days, the effects of early corticosteroid treatment and initial ICU treatment factors could be uniformly applied to all patients. Also, the confounding effect that early mortality cases might be associated with insufficient survival time for the development of CAPA could be excluded. Respiratory support was defined as mechanical ventilation or high-flow oxygen therapy (≥ FiO2 0.4 with a setting ≥ 30 L/min flow rate). Because a prior study reported that mortality for patients with CAPA not receiving appropriate antifungal treatment was 100%,19 we excluded patients who satisfied the CAPA definition but improved with short-term antifungal therapy (< 10 days) or without antifungal therapy. In addition, we excluded those who did not meet the CAPA definition but were treated as CAPA cases.
Definition, outcome, and data collection
CAPA was diagnosed by the 2020 European Confederation for Medical Mycology and the International Society for Human and Animal Mycology (ECMM/ISHAM) consensus criteria, which define CAPA as three classifications (proven, probable, and possible) based on histological, microbiological, imaging, and clinical factors (Supplementary Table 2).3 Two infectious disease physicians evaluated by consensus whether the patient satisfied the ECMM/ISHAM consensus criteria and whether the diagnosed patient was clinically false positive for ECMM/ISHAM criteria. In this study, we included possible CAPA, because of the difficulty of invasive study to diagnose CAPA - which was resulted from transmission risk, and could be a factor for false-negative diagnosis for CAPA rather than false-positive. Galactomannan of serum or respiratory tract specimen was measured using an enzyme-linked immunosorbent assay kit (Platelia Aspergillus; Bio-Rad Laboratories, Hercules, CA, USA), following the manufacturer’s instructions. Fungus cultures were implemented in Sabouraud dextrose agar at 25°C for 5 days
The primary objective of our study was to evaluate risk factors related to development of CAPA. The secondary objectives of our study were comparing clinical outcomes between patients with CAPA (CAPA group) and those without CAPA (non-CAPA group). Two clinical outcomes were compared: 90-day overall mortality and respiratory support-free rates among surviving patients. For example, when a COVID-19 patient was extubated and was stable on low-flow oxygen therapy, that patient was recorded as free from respiratory support. If patients were continuously supported by mechanical ventilation, ECMO, or high flow oxygen therapy during the observation period, that patient was recorded as not free from respiratory support. Patients were observed until death, discharge from the admitted medical center, transfer to other medical institutions, or for 90 days after at least 10-day ICU admission.
Since results of dexamethasone use for COVID-19 patients from the RECOVERY trial were published in July 2020, corticosteroids have become a standardized treatment for severe COVID-19.16 Considering the dexamethasone dose of the RECOVERY study protocol (6 mg once daily for up to 10 days or until hospital discharge), we collected the following data of steroid dose: 1) Cumulative dose for initial 10 days, 2) Peak dose, and 3) Total cumulative dose (Supplementary Fig. 1). In addition, we divided patients into two groups whether the patient received more than 60mg of dexamethasone or a dexamethasone equivalent dose based on the steroid dose suggested from the RECOVERY study protocol. To evaluate additional risk factors for CAPA and adjust clinical factors related to clinical outcomes, patient demographics, underlying disease (myocardial infarction and chronic heart failure for chronic heart disease; chronic obstructive pulmonary disease, asthma, and bronchiectasis for chronic lung disease), COVID-19 disease severity, and concomitant COVID-19 treatments were collected from electronic medical records.
Statistical analysis
All statistical analyses were performed using Stata 15.1 (StataCorp., College Station, TX, USA). To compare patient characteristics between the CAPA and non-CAPA groups, Student’s t-test or Mann-Whitney U test was used to compare continuous variables, and the Chi-square test or Fisher’s exact test was used to compare categorical variables. Variables with statistical significance in the univariate analysis along with variables considered potential clinically meaningful were included in the binary logistic regression model.
To compare clinical outcomes between the CAPA and the non-CAPA groups, matched propensity score (PS) modeling of 1:5 was used to reduce the risk of bias for exposure. PS was calculated based on the logistic regression method including the following variates: mechanical ventilation, inotrope or vasopressor use, early high-dose corticosteroid administration, diabetes, chronic lung disease, glycopeptide use, and carbapenem use. If patients in the CAPA group could not be matched with five patients in the non-CAPA group, they were matched with one to four patients in the non-CAPA group. Because not all pairs were matched equally, a weighted-matching analysis was implemented. Covariate balance after weighting was assessed using the absolute standardized mean difference. A standard difference ≥ 20% was considered a meaningful imbalance. A Cox proportional hazard regression model was used to compare in-hospital mortality and respiratory support-free rates.
All P values were two-tailed, and P values < 0.05 were considered statistically significant.
RESULTS
Study population
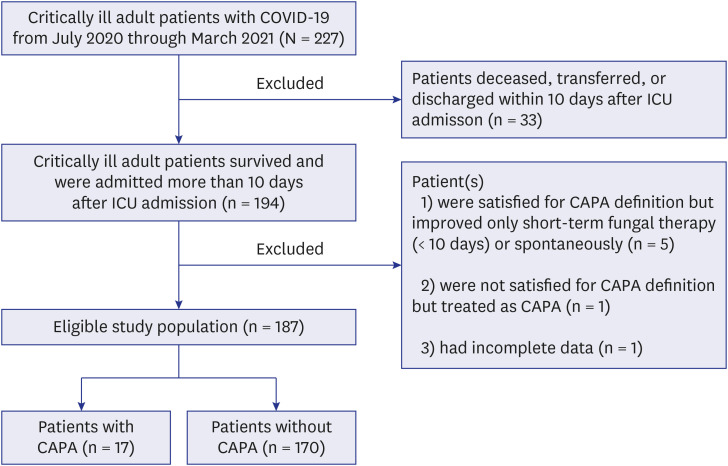
There were 227 critically ill COVID-19 patients during the study period. Of these, 33 patients were deceased within 10 days after ICU admission. Five patients fulfilling the CAPA definition were excluded because they spontaneously recovered without antifungal treatment. One patient did not meet CAPA criteria but was treated as a CAPA case. One patient with incomplete clinical data was excluded. Thus, 187 patients who survived ≥ 10 days after ICU admission were further analyzed (Fig. 1). Of these, 17 (9.1%) patients developed CAPA, an incidence of 33.10 (95% CI, 19.93–51.92) per 10,000 patient-day units. Fifteen and two cases were defined as probable and possible CAPA, respectively. Computed tomography was performed in 58.8% (10/17) of patients with CAPA. There were three patients with multiple pulmonary nodules, two with lung cavitation, and three with newly developed focal consolidation. The others had aggravating pulmonary infiltration. The median interval between symptom onset and CAPA diagnosis was 25 days (range: 2–77 days). Voriconazole, which was administrated to 94.1% (16/17) of CAPA patients, was the most favored antifungal agent for CAPA patients (Supplementary Table 3).
Risk factors associated with CAPA
There was no difference in the age distribution (median: 73 vs. 72 years old in CAPA vs. non-CAPA groups, P = 0.533) or sex ratio (64.7% and 59.4% male for CAPA and non-CAPA groups, respectively; P = 0.671). Chronic lung disease, cumulative dose for the initial 10 days > 60 mg of dexamethasone or dexamethasone equivalent dose, and glycopeptide use were more common in the CAPA group compared to the non-CAPA group (all P < 0.05). The total cumulative corticosteroid dose was tended to be higher in the CAPA group without statistical significance. Although there was no statistical significance, patients with CAPA experienced more frequent mechanical ventilation and inotrope/vasopressor use (Table 1).
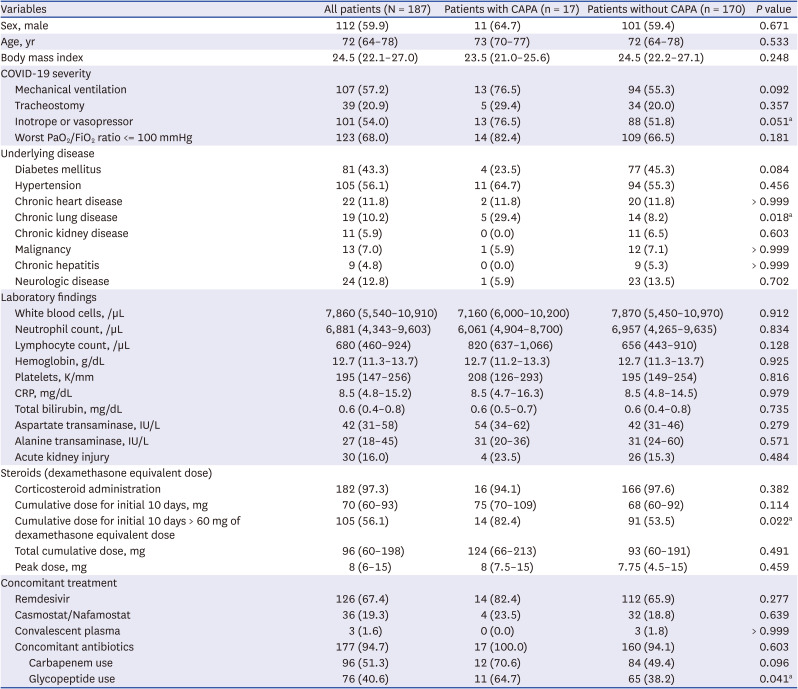
Table 1
Clinical characteristics of patients with or without coronavirus disease 2019-associated pulmonary aspergillosis
Values are presented as median (IQR) or number (%) for descriptive analyses or frequency analyses, respectively.
CAPA = coronavirus disease 2019-associated pulmonary aspergillosis, COVID-19 = coronavirus disease 2019, IQR = interquartile range.
aVariables included in the binary logistic regression model.
![]()
In multivariable analysis, cumulative dose for the initial 10 days > 60 mg of dexamethasone or dexamethasone equivalent dose was associated with the CAPA group (adjusted odds ratio [OR], 3.77; 95% confidence interval [CI], 1.03–13.79, P = 0.045). In addition, chronic pulmonary disease was also associated with the CAPA group (adjusted OR, 4.20; 95% CI, 1.26–14.02; P = 0.020; Table 2).

Table 2
The factors associated with coronavirus disease 2019-associated pulmonary aspergillosis
![]()
Clinical outcomes
The 30-day and 90-day all-cause mortality rates in the CAPA group were 36.3% and 54.3%, and those in the non-CAPA group were 23.6% and 35.2%, respectively (P > 0.05). The 90-day mortality of CAPA patients tended to be higher than that of non-CAPA patients, without statistical significance (hazard ratio [HR], 1.48; 95% CI, 0.65–3.37; P = 0.346; Fig. 2A). In the PS-matched model, the absolute standardized differences of all covariates included in the model were less than 20% (Supplementary Fig. 2). After matching, there was still no statistical significance in 90-day overall mortality difference between the CAPA and non-CAPA groups (54.3% vs. 41.7%, HR, 1.28; 95% CI, 0.49–3.31; P = 0.613; Fig. 2B).
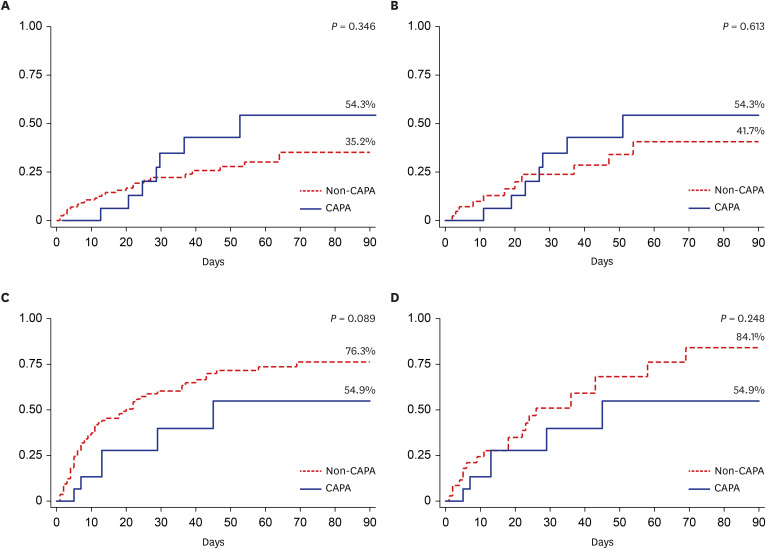
Fig. 2
Cumulative incidence curve of primary and secondary outcomes. (A) 90-day overall mortality (raw data), (B) 90-day overall mortality (propensity score [PS]-matched model), (C) respiratory support-free rates among surviving patients (raw data), and (D) respiratory support-free rates among surviving patients (PS-matched model).
CAPA = COVID-19-associated pulmonary aspergillosis.
![]()
In the analysis of respiratory support-free rates in the study population, only patients who needed respiratory support on the starting day of the observation period (10 days after ICU admission) were included. Therefore, 15 and 109 patients in the CAPA and non-CAPA groups, respectively, were included in this analysis. The CAPA group showed a lower respiratory support-free rate among surviving patients compared to the non-CAPA group (54.9% vs. 76.3%, HR, 2.07; 95% CI, 0.90–4.79; P = 0.089, Fig. 2C). A similar difference was observed in the PS-matched model (54.9% and 84.1%, HR, 1.71; 95% CI, 0.69–4.25; P = 0.248; Fig. 2D).
DISCUSSION
In the present study, early high-dose steroid administration and chronic pulmonary disease were associated with CAPA in the setting where steroids and remdesivir were considered as standard COVID-19 treatments. In addition, patients with CAPA seemed to have higher mortality and delayed recovery from respiratory support.
Since the 2010s, invasive pulmonary aspergillosis has been frequently observed among patients admitted to ICU or infected with a respiratory virus such as influenza.520 These patients did not have typical host factors for invasive fungal infection defined by the EORTC/MSG criteria.21 Several prospective and retrospective cohort studies have shown risk factors and clinical outcomes of CAPA. A prospective multicenter study from Italy showed that 27.7% of patients were diagnosed with CAPA among patients receiving mechanical ventilation therapy, and the 30-day mortality of CAPA patients was significantly higher than that of non-CAPA patients (44% vs. 19%, P = 0.002). Corticosteroids were administered to 60% and 46.6% of CAPA and non-CAPA patients, respectively (P = 0.29), and the cumulative dose did not differ significantly between the groups (100 mg and 107 mg of median prednisone equivalent doses in CAPA patients and non-CAPA patients, respectively, P = 0.89).11 In contrast, another multicenter CAPA study from five Johns Hopkins hospitals reported that corticosteroid exposure during index admission was associated with CAPA. In that study, patients with CAPA required a longer time to improve and a longer hospital length of stay.10
In our study, the incidence of CAPA among critically ill patients who needed respiratory support was 9.1% or 33.10 (95% CI, 19.93–51.92) per 10,000 patient days. One systematic review and meta-analysis of CAPA cohort studies reported that the incidence of CAPA from eight serial studies was 14.9% (between 3.3 and 34.4%), and all of these studies were conducted during the first wave of the COVID-19 pandemic (January to July 2020).22 The CAPA incidence in our study was similar or slightly lower than those of the previous cohort studies. This might be associated with regional and temporal differences in COVID-19 epidemiology.
The prior meta-analysis, which included 64.7% of patients receiving corticosteroids after COVID-19 diagnosis, reported that initial corticosteroid treatment was not associated with CAPA in pooled data (OR, 0.69; 95% CI, 0.19–2.58).22 Our study included 97.3% of patients receiving corticosteroids, but the incidence of CAPA was similar to those of prior studies. These findings support that steroid exposure itself is not associated with CAPA. One retrospective cohort study from France reported a trend between high-dose dexamethasone (cumulative dose ≥ 100 mg) and IPA.13 Our study showed that COVID-19 patients with CAPA were tended to be receiving the higher dose of corticosteroids, especially for initial periods for steroid administration. Patients with CAPA statistically more received > 60 mg of dexamethasone or equivalent dose of corticosteroid during the initial 10 days. The total cumulative dose or peak dose of corticosteroid was higher in patients with CAPA, but no significance was observed. It might be because 1) CAPA patients had a relatively short observation period resulting from high mortality and 2) dose of steroid administrated after CAPA diagnosis should not be included.
Traditionally, invasive fungal infection was associated with corticosteroids in a dose-dependent manner 23. In addition, the pathogenesis of severe COVID-19 was associated with both immunosuppression and hyper-inflammation.24 Patients with severe COVID-19 frequently show lymphopenia, which was presumed to be the result of direct viral invasion of lymphocytes, redistribution of chemokines, and apoptosis enhancement.2425 In contrast, a significant increase of pro-inflammatory cytokines such as IL-6 and IL-1β due to overreaction to viral stimulation is frequently observed in severe COVID-19 patients and leads to tissue damage and multiple organ failure.2426 Dexamethasone was administered to adjust hyper-inflammation during COVID-19 disease progression17; however, our study suggested that a high dose of corticosteroids could be contributed to the occurrence of invasive aspergillosis accompanied by immunosuppression and tissue damage during COVID-19 pathogenesis. Therefore, an appropriate dose of steroid administration to suppress hyper-inflammation without causing excessive immunosuppression might be important, especially for the early phase when patients experienced disease progression. Although the COVID STEROID 2 Randomized trial suggested that there was no difference of invasive fungal infection between patients with COVID-19 and severe hypoxemia receiving 12 mg/day and 6 mg/day of dexamethasone up to 10days (3.0% versus 4.3%, relative risk 0.85 [95% CI, 0.50–1.43]), this study observed occurrence of invasive fungal infection for only 28 days after randomization.18 In our study, the median interval between symptom onset and CAPA diagnosis was 25 days. In addition, 72.7% of patients received corticosteroid more than 10-days. Therefore, observation periods of COVID STEROID 2 Randomized trial might be not enough to include late-onset invasive fungal infection, and our study might have a higher late-onset CAPA rate because of longer corticosteroids administration.
Our study showed that chronic pulmonary disease was also associated with CAPA. This finding was in line with prior studies. One systematic review for 186 patients with CAPA from March to August 2020 reported that 21.5% of patients had chronic pulmonary disease.8 The meta-analysis reported that patients with COPD had a 2.75-fold higher risk of CAPA occurrence than did those without COPD.12 Direct damage of the airway epithelium and ciliary dysfunction due to a respiratory virus promote tissue invasion by aspergillus.27 Therefore, patients with existing structural or functional chronic pulmonary disease could be more vulnerable to CAPA than patients with normal respiratory systems. In this regard, close monitoring for CAPA occurrence should be needed for critically ill COVID-19 patients with underlying chronic pulmonary diseases receiving high-dose of corticosteroids.
There were some discrepancies; several studies reported that CAPA patients had higher mortality or delayed recovery.9101322 Although statistical significance was not observed, possibly because of the small number of included patients, our study showed that CAPA patients had higher 90-day mortality and less frequent recovery from respiratory organ support. Compared to prior studies reporting the more apparent poor outcomes of patients with CAPA, our study included only COVID-19 patients after the introduction of remdesivir and corticosteroids. In addition, health care services in the Republic of Korea were well maintained across the pandemic period.28 This might lead to timely and standard management for critically ill COVID-19 patients and could attenuate the adverse effects of CAPA in COVID-19 outcomes. Furthermore, the CA PA onset of COVID-19 patients was relatively delayed compared to a prior study (median of 22 days after symptom onset in our study vs. 10 days in the prior meta-analysis), and CAPA seems to be associated with delayed mortality and poor outcomes in the late period of ICU admission.
There are several limitations to this study. First, no definitive CAPA cases were observed. In this study, elevated serum galactomannan index was the most common microbiological evidence of CAPA. This reflected the attempts of most clinicians to diagnose CAPA with a non-invasive method because of transmission risk in invasive diagnostic procedures. However, it has been established that the sensitivity of serum galactomannan is not high in diagnosing CAPA.3 False-negative CAPA cases could be included in this study. Second, this study was implemented before the Delta variant of the SARS-CoV-2 outbreak in the Republic of Korea.29 In addition, no patients with completed vaccinations were included in this study. Because of the increased virulence of the Delta variant and the preventive effect of COVID-19 vaccination for severe disease,3031 the epidemiology and clinical characteristics of CAPA in the more recent period might be different from those in this study.
In conclusion, our study suggests that patients receiving corticosteroids at a higher dose than recommended in the early period and patients with chronic pulmonary disease might be at high risk for CAPA, which could affect the adverse outcomes for critically ill COVID-19 patients in the late period of disease progression. Further studies are warranted to prevent CAPA, such as prophylactic antifungal treatment for critically ill COVID-19 patients with risk factors for CAPA development.
 XML Download
XML Download