

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Since the first case was reported in December 2019, coronavirus disease 2019 (COVID-19) has rapidly spread worldwide, with 264,414,261 confirmed cases and 5,250,036 deaths globally, as of December 2021.1 Meanwhile, South Korea reported 457,612 confirmed cases, with 3,705 deaths.2 The pandemic resulted in the expeditious development of vaccines. Currently, 79.9% of the Korean population has received appropriate vaccination.2 In conjunction with the vaccination drive, the Korean government announced a policy characterized as “living with COVID-19” (“with-corona”), preparing for a switch to the new normal, starting November 1, 2021.2 However, confirmed cases continued to increase rapidly after the change, leading to the postponement of the with-corona policy and the extension of distancing measures. In addition, breakthrough infections in vaccinated individuals were reported,3 underlining the need to promote the distancing policy.
Physical distancing is one of the most effective measures to prevent the spread of the virus.45 The term physical distancing appears more appropriate, rather than social distancing, since social distancing implies that people have to socially separate from their family or neighbors.6 Although physical distancing is effective in reducing the spread of the infection, adherence varies across different groups of individuals. Previous studies reported that country, race, income, education, and health service availability can influence adherence to physical distancing.789 Individual factors such as health-related beliefs and perceived social norms can also influence adherence to physical distancing.10
The health belief model has been widely employed to understand health-related behaviors.11 It was initially developed to explain why people did or did not participate in screening for tuberculosis. The model evolved over time, but the main constructs include perceived susceptibility, severity, perceived benefits, and perceived barriers.11 In addition, self-efficacy and cues to action further explain health-related behaviors of individuals. Previously, the constructs of the health belief model had been utilized to understand health-related behaviors associated with influenza vaccination.212 Similarly, during the COVID-19 pandemic, information from the media, government policy, and public feedback can interact and influence the health beliefs of individuals, thus changing health-related behaviors such as physical distancing.
Social and personal norms can also influence health-related behaviors.13 Norms are defined as attitudes and behaviors that are approved and expected by group members. Social norms can be descriptive or injunctive. Descriptive social norms indicate an individual’s perception of whether other people are engaging in a behavior, whereas injunctive social norms indicate the perception of what other people are thinking about an individual’s behavior. Injunctive personal norms indicate what an individual think about their own behavior, which reflect internalized moral rules. Given the independent association of each norm with health-related behaviors,1415 social and personal norms can influence adherence to physical distancing.
During the initial COVID-19 outbreak in Korea, high school students experienced a significant change in the school environment. The first COVID-19 case was reported on January 20, 2020, and an outbreak followed, leading to the postponement of the new school year, which typically begins in March. Schools reopened in mid-May, but thereafter, they closed and reopened at irregular intervals according to the physical distancing guidelines.16 When schools remained open, the students were required to maintain physical distance from others. This change in routine and physical distancing resulted in increased loneliness and isolation, causing mental health problems such as depression and anxiety.17 Adhering to the physical distancing guidelines may be more challenging for high school students, since they are highly dependent on peer groups. In addition, as adolescents, high school students display increased risk-taking behaviors.18 Breaking physical distancing guidelines may be one such behavior that can affect the health of students as well as others.
Assessing the factors that influence adherence to physical distancing is important, since different measures can be applied to encourage adherence. However, among high school students, the factors influencing adherence to physical distancing are still to be clarified. In this study, we aim to explore whether high school students’ adherence to physical distancing is associated with health beliefs, social norms, and psychological factors during the COVID-19 pandemic.
Go to : 
METHODS
Participants and procedure
This anonymous online survey was conducted among high school students from October 18–24, 2021, by the professional survey company, EMBRAIN (www.embrain.com). Through the survey, we collected participants’ age, sex, grades, types of school, living area, and responses to COVID-19 questions such as “Were you quarantined due to COVID-19 infection?”, “Were you infected with COVID-19?”, “Did you get vaccinated?”, or “Do you want to get vaccinated, if vaccines are available?”. Past and present psychiatric symptoms were evaluated by questions such as “Did you experience or receive treatment for depression, anxiety, or insomnia?” and “Do you believe you are depressed or anxious, or do you need help for your mood state?” We developed the survey form in Korean language and followed the Checklist for Reporting Results of Internet e-Surveys (CHERRIES) guidelines.19 An investigator (TL) tested the usability and technical functionality of the developed e-survey form before its implementation.
Sample size estimation was performed based on 30 participants per cell.20 For each sex (boys and girls) and grade (1st, 2nd, and 3rd), 50 samples were allocated.
Measures
Attitude toward physical distancing during the pandemic
Participants’ attitude toward physical distancing was evaluated using a questionnaire from a previous study.21 We evaluated participants’ adherence to physical distancing in terms of 3 types of concepts: adherence to physical distancing, health beliefs model, and social norms. First, adherence to physical distancing was assessed using 5 items related to one’s minimized contact with others by staying home, minimized non-essential errands outside the home, avoidance of receiving guests at home, avoidance of social gatherings with more than 2 people, and maintenance of at least 2 m distance from others in public places (5-point Likert scale ranging from 1 [never] to 5 [almost always]). Second, participants’ beliefs regarding health issues in COVID-19 was assessed using perceived susceptibility or severity, perceived benefit, and perceived barrier based on the health beliefs model.11
Perceived susceptibility or severity was evaluated with 3 items that assessed the extent to which participants perceived that they were susceptible to being infected by the virus, that the infection would be risky for them, and that the infection would be risky for members of the community (5-point Likert scale ranging from 1 [not at all] to 5 [extremely]). Perceived benefit of physical distancing was evaluated using 3 items: the belief that physical distancing was effective in protecting them from the virus, protecting vulnerable others, and solving the ongoing pandemic (5-point Likert scale ranging from 1 [not at all] to 5 [extremely]). Perceived barrier was assessed using 3 items regarding the extent to which participants found the recommendations financially costly for themselves, frustrating and unpleasant, and difficult to apply in their daily life (5-point Likert scale ranging from 1 [not at all] to 5 [extremely]). Third, perceived social norms were evaluated using an item related to descriptive social norms measuring the extent to which participants perceived that others in their community were respecting physical distancing directives (5-point Likert scale ranging from 1 [not at all] to 5 [extremely]), an item related to injunctive social norms measuring the extent to which they believed their close friends and family would (dis)approve if they learned that they did not respect physical distancing recommendations (5-point Likert scale ranging from 1 [they would approve] to 5 [they would very much disapprove]), and item related to injunctive personal norms measuring the extent to which they believed it was their civic duty to follow these directives (5-point Likert scale ranging from 1 [not at all] to 5 [extremely]).
Cronbach’s alpha in this study was 0.813 for adherence to physical distancing, 0.753 for perceived susceptibility or severity, 0.812 for perceived benefit, and 0.774 for perceived barrier. Confirmatory factor analysis (CFA) for confirming the single-factor structure model showed a good fit for model for adherence to physical distancing (comparative fit index [CFI] = 0.984, Tucker-Lewis index [TLI] = 0.968, root mean square error of approximation [RMSEA] = 0.064, and standardized root mean square residual [SRMR] = 0.065), perceived susceptibility or severity (CFI = 1.00, TLI = 1.00, RMSEA = 0.00, and SRMR < 0.001), perceived benefits (CFI = 1.00, TLI = 1.00, RMSEA = 0.00, and SRMR < 0.001), and perceived barriers (CFI = 1.00, TLI = 1.00, RMSEA = 0.00, and SRMR < 0.001). We did not conduct CFA for perceived social norms as it contains three items that reflect different types of social norms: descriptive social norms, personal injunctive norms, and social injunctive norms.
Stress and Anxiety to Viral Epidemics-6 items (SAVE-6)
SAVE-6 was originally developed to assess an individual’s viral anxiety 22 and was used to measure viral anxiety in this study. It consists of six items that can be rated on a 5-point Likert scale ranging from 0 (never) to 4 (always). The total score of SAVE-6 can range from 0 to 24, and higher total score reflects levels of anxiety response to viral epidemics. In this study, we applied SAVE-6 to high school students without any modification. Cronbach’s alpha was 0.844 among this sample.
Patient Health Questionnaire-9 items (PHQ-9)
PHQ-9 is a self-report rating scale for measuring severity of depression.23 It consists of 9 items, and each item can be rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The total score of PHQ-9 ranges from 0 to 27, and high scores reflect severe levels of depression. In this study, we used the Korean version of PHQ-9,24 and Cronbach’s alpha was 0.910.
Satisfaction with Life Scale (SWLS)
SWLS is a questionnaire that evaluates overall judgment about one’s life. It comprises 5 items grouped in a single dimension, and each item is rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). A higher total score indicates greater satisfaction with life. The reliability and validity of the SWLS have been previously confirmed.25
Connor Davidson Resilience Scale 2-items (CD-RISC2)
CD-RISC2 is a self-report rating scale for measuring resilience. It is a shortened version of the original full 25-item CD-RISC scale. It consists of two items that can be rated on a 5-point Likert scale ranging from 0 (not true at all) to 4 (true nearly all of the time). In this study, we used the Korean version of the CD-RISC2 scale,26 and the Guttman split-half coefficient was 0.730.
Statistical analysis
Demographic characteristics and rating scale scores are summarized as mean ± standard deviation. The level of significance for the analyses was defined as two-tailed at values of P < 0.05. Continuous variables were analyzed using the Student’s t-test, and categorical variables using the χ2 test. Correlation analyses were conducted using Pearson’s correlation analysis. A linear regression analysis was performed to reveal the predicting variables for adherence to physical distancing. In addition, to explore whether perceived susceptibility or severity and perceived social norms are associated with adherence to physical distancing, and whether perceived benefit from physical distancing and viral anxiety mediate the association, the bootstrap method with 2,000 resamples was implemented. Furthermore, we explored the validity and reliability of the questionnaires for attitude toward physical distancing during the pandemic21 among this sample. Data suitability and sampling adequacy were assessed using Kaiser-Meyer-Olkin (KMO) value and Bartlett’s test of sphericity. In CFA, model fit was assessed using CFI, TLI, RMSEA, and SRMR values.2728 Reliability based on internal consistency was evaluated using Cronbach’s alpha. We used SPSS version 21.0, AMOS version 27 for Windows (IBM Corp., Armonk, NY, USA), and JASP version 0.14.1 to perform the statistical analyses.
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of the Asan Medical Center (2021–1361), and the requirement of written informed consent was waived by the IRB.
Go to :
RESULTS
The demographic characteristics of the participants are presented in Table 1. They resided in the cities of Seoul (n = 55, 18.3%), Pusan (n = 9, 3.0%), Daegu (n = 15, 5.0%), Daejeon (n = 14, 4.7%), Gwangju (n = 5, 1.7%), Incheon (n = 25, 8.3%), Ulsan (n = 8, 2.7%), and the provinces of Gyeonggi (n = 81, 27.0%), Chungcheong (n = 19, 6.3%), Jeolla (n = 16, 5.4%), Gyeongsang (n = 41, 13.7%), Gangwon (n = 8, 2.7%), and Jeju (n = 4, 1.3%). Male students accounted for 50.0% of the participants. Regarding COVID-19, 22.7% had been quarantined, 1.7% had been infected, and 42% had been vaccinated, and among those who were not vaccinated (n = 174), 64.4% wanted to get vaccinated depending on the availability of vaccines. Among the students, 17.3% reported that they had experienced depression, anxiety, or insomnia, and 12.7% reported that they currently suffer from depression, anxiety, or insomnia.
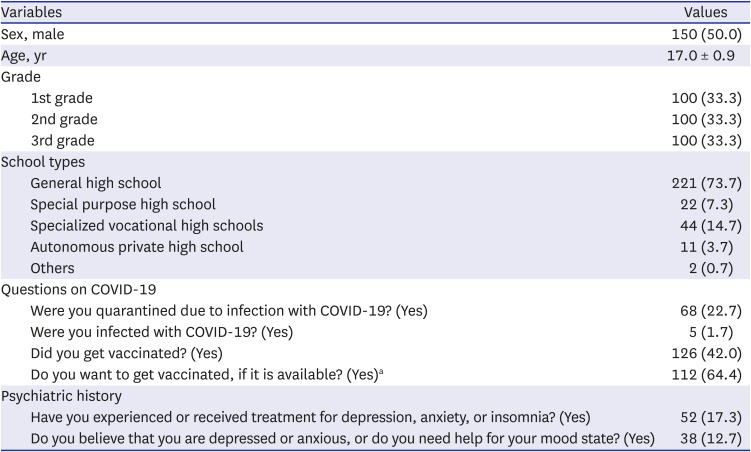
Table 1
Participant characteristics (n = 300)
Values are expressed as mean ± standard deviation or number (%).
COVID-19 = coronavirus disease 2019.
aAmong participants who did not get vaccinated (n = 174).
![]()
Pearson’s correlation analysis showed that age was significantly correlated with adherence to physical distancing (r = 0.12, P < 0.05), SWLS (r = −0.12, P < 0.05), and CD-RISC2 (r = 0.15, P < 0.01) (Table 2). Adherence to physical distancing was significantly correlated with perceived susceptibility or severity (r = 0.35, P < 0.01), perceived benefits (r = 0.51, P < 0.01), descriptive social norms (r = 0.26, P < 0.01), social injunctive norms (r = 0.47, P < 0.01), personal injunctive norms (r = 0.48, P < 0.01), SAVE-6 (r = 0.40, P < 0.01), and CD-RISC2 (r = 0.19, P < 0.01). Perceived susceptibility or severity was significantly correlated with perceived benefit (r = 0.47, P < 0,01), perceived barrier (r = 0.25, P < 0.01), social injunctive norms (r = 0.30, P < 0.01), personal injunctive norms (r = 0.40, P < 0.01), SAVE-6 (r = 0.64, P < 0.01), SWLS (r = −0.13, P < 0.05), and PHQ-9 (r = 0.17, P < 0.01). Perceived benefits were significantly correlated with descriptive social norms (r = 0.21, P < 0.01), social injunctive norms (r = 0.38, P < 0.01), personal injunctive norms (r = 0.54, P < 0.01), SAVE-6 (r = 0.32, P < 0.01), and CD-RICS2 (r = 0.17, P < 0.01). Perceived barriers were significantly correlated with descriptive social norms (r = 0.13, P < 0.05), SAVE-6 (r = 0.29, P < 0.01), and PHQ-9 (r = 0.15, P < 0.05). Descriptive social norms were significantly correlated with social injunctive norms (r = 0.28, P < 0.01), personal injunctive norms (r = 0.22, P < 0.01), SAVE-6 (r = 0.19, P < 0.01), and SWLS (r = 0.18, P < 0.01). Social injunctive norms were correlated with personal injunctive norms (r = 0.49, P < 0.01), SAVE-6 (r = 0.33, P < 0.01), and CD-RISC2 (r = 0.16, P < 0.01). Personal injunctive norms were correlated with SAVE-6 (r = 0.34, P < 0.01) and CD-RISC2 (r = 0.22, P < 0.01). SAVE-6 was significantly correlated with PHQ-9 (r = 0.16, P < 0.01), and PHQ-9 was correlated with SWLS (r = −0.38, P < 0.01) and CD-RISC2 (r = −0.21, P < 0.01). SWLS was correlated with CD-RISC2 (r = 0.16, P < 0.01).
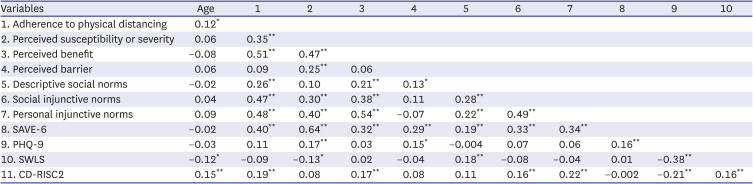
Table 2
Correlation coefficients of each variable for all participants
SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items, PHQ-9 = Patient Health Questionnaire-9 items, SWLS = Satisfaction With Life Scale, CD-RISC2 = Connor Davidson Resilience Scale-2 items.
*P < 0.05, **P < 0.01.
![]()
A multiple linear regression analysis was conducted to evaluate predicting factors for adherence to physical distancing among high school students (Table 3). Perceived susceptibility or severity (β = −0.13, P = 0.038), perceived benefit (β = 0.32, P < 0.001), descriptive social norms (β = 0.10, P = 0.041), social injunctive norms (β = 0.19, P < 0.001), and SAVE-6 (β = 0.24, P < 0.001) were significantly associated with adherence to physical distancing (adjusted R2 = 0.42, F = 19.2, P < 0.001).
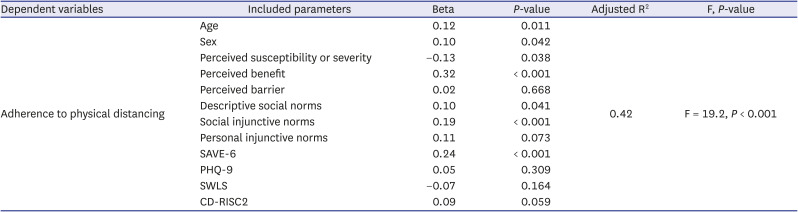
Table 3
Linear regression analysis exploring the adherence to physical distancing among high school students during the COVID-19 pandemic
COVID-19 = coronavirus disease 2019, SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items, PHQ-9 = Patient Health Questionnaire-9 items, SWLS = Satisfaction With Life Scale, CD-RISC2 = Connor Davidson Resilience Scale-2 items.
![]()
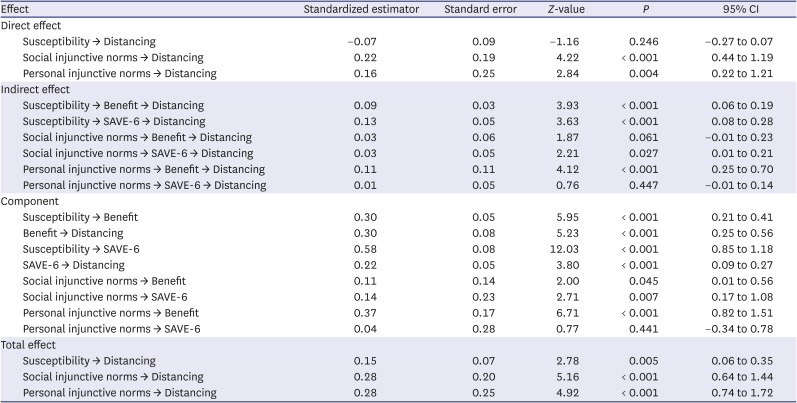
Mediation analysis showed that there was a direct effect of social and personal injunctive norms on adherence to physical distancing among high school students during the pandemic (Table 4). The association between social injunctive norms and adherence to physical distancing was partially mediated by viral anxiety measured by SAVE-6, but the relationship between personal injunctive norms and adherence to physical distancing was partially mediated by perceived benefit (Fig. 1). The association between perceived susceptibility or severity and adherence to physical distancing was entirely mediated by perceived benefit or viral anxiety.
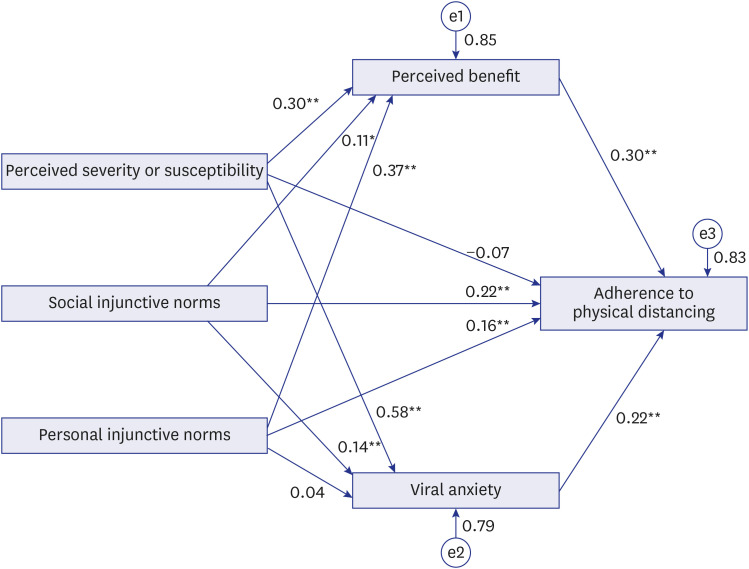 | Fig. 1Mediation model showing the pathway from the effect of perceived susceptibility or severity, social injunctive norms, and personal injunctive norms (independent variables) on adherence to physical distancing (outcome) through perceived benefit of physical distancing and viral anxiety (mediator). Viral anxiety was measured by SAVE-6.SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items.
*P < 0.05, **P < 0.01.
|
Table 4
The results of direct, indirect, and total effects on mediation analysis
![]()
Go to :
DISCUSSION
In this study, we observed that high school students’ adherence to physical distancing was predicted by their perceived susceptibility or severity, perceived benefit, descriptive social norms, social injunctive norms, and viral anxiety measured by SAVE-6 during COVID-19. Social and personal injunctive norms directly influenced their adherence to physical distancing. Viral anxiety partially mediated the association between social injunctive norms and adherence to physical distancing, and perceived benefits of physical distancing partially mediated the association between personal injunctive norms and adherence to physical distancing. In addition, perceived anxiety and viral anxiety entirely mediated the association between perceived susceptibility or severity and adherence to physical distancing of high school students.
Adherence to physical distancing was significantly associated with perceived benefits among high school students. In contrast, perceived barrier did not show a significant association with adherence to physical distancing. The findings from our study are in line with the results of a previous study on acquired immunodeficiency syndrome (AIDS), where perceived benefit was suggested as the main component that induced condom use.29 Taken together, this implies the importance of promoting positive effects in changing health-related behaviors. In addition, high school students in their adolescence are prone to underestimate barriers owing to egocentricity, a phenomenon that is referred to as personal fable.30 This cognitive bias may have affected the insignificant association of perceived barrier with physical distancing in our study.
The results indicated that adherence to physical distancing was significantly associated with injunctive social norms. This implies that whether other people approve or disapprove physical distancing behavior is important for such adherence. Previous studies indicate that injunctive norms can significantly influence a wide range of behaviors, from eating habits to drug use.31 In addition, as high school students are in a developmental stage in which acceptance by others, especially peers, is important, they would prefer avoiding situations that could evoke criticism from the group.32 This peer pressure sensitivity can magnify the effect of social injunctive norms.
Depressive symptoms assessed by PHQ-9 did not show significant association with adherence to physical distancing. This is in conflict with previous studies3334 that indicate that depressive symptoms predict lower compliance to distancing. However, these previous studies did not account for various factors that can affect adherence to physical distancing, such as perceived susceptibility or viral anxiety, which can have a confounding effect on adherence. A recent longitudinal study further supports the null effect of depressive symptoms on adherence to physical distancing.35
The results of the mediation analysis indicate that perceived susceptibility or severity has no significant direct effect on adherence to physical distancing. However, indirect effects mediated via viral anxiety or perceived benefits existed, suggesting that perceiving COVID-19 as risky alone is insufficient to influence physical distancing adherence. A possible reason for the lack of direct influence of perceived susceptibility or severity on adherence to physical distancing is that high school students may perceive the pandemic to be less severe than it is in reality. The results indicated that perceived susceptibility was one of the factors predicting COVID-19 prevention behavior, but perceived severity was not.36 In addition, high school students have high novelty-seeking and low harm-avoidance behaviors compared to adults,3738 which may explain the absence of direct effects of perceived susceptibility or severity. Second, the survey was conducted after 20 months of the implementation of physical distancing in Korea. This may have led to “pandemic fatigue,” in which people can have lower risk perceptions regarding COVID-19.39 However, in this study, this lack of direct association was entirely mediated by viral anxiety or perceived benefits.
Social and personal injunctive norms showed both direct and indirect effects on adherence to physical distancing. The indirect effect of social injunctive norms was mediated by viral anxiety. High school students with higher anxiety levels may be more sensitive to peer pressure.40 Peer pressure is closely related to social injunctive norms,41 which can be a possible explanation for this mediating effect. Additionally, the indirect effect of personal injunctive norms was mediated by perceived benefits. Our results suggest that beliefs about the benefits of physical distancing, combined with internalized values and expectations, can lead to autonomous behavioral change.
In this study, viral anxiety was assessed using SAVE-6. Originally developed as a subcategory of the SAVE-9 scale,42 SAVE-6 showed good internal consistency and reliability. Although widely used scales, such as the Generalized Anxiety Disorder 7-item, exist to measure anxiety, previous scales assess anxiety in general. In contrast, SAVE-6 measures anxiety specifically related to the viral epidemic, including fear, contagion, stigmatization, and anxious responses. Moreover, SAVE-6 is brief, and thus, is practical to apply in a pandemic situation.
The limitations of this study also warrant discussion. First, the study was conducted through an online survey system by a professional survey company. The participants were enrolled from those registered as panels in the survey company; this may have led to bias. Furthermore, as this study involved online surveys, and not face-to-face interviews, the reliability of the responses may be affected. We decided to conduct this study online to prevent the possible spread of the virus in light of the pandemic. Second, only 300 students participated in the survey, which corresponds to only 2.2% of all high school students in Korea, and thus, the results cannot be generalized. Third, 42% of the participants were vaccinated, which may have influenced the results. Fourth, the online education environment or the availability of remote learning might have influenced the attitude toward adherence to physical distancing. Lastly, we did not distinguish between perceived susceptibility and perceived severity, which are categorized independently in the health beliefs model, which needs to be elucidated in future studies.
In conclusion, we observed that high school students’ adherence to physical distancing was predicted by perceived benefits of physical distancing, social injunctive norms, personal injunctive norms, and viral anxiety under COVID-19. Moreover, viral anxiety or perceived benefits of physical distancing may mediate this relationship. Explaining the rationale or benefits of physical distancing may be important while developing public prevention policy to enhance adherence to physical distancing.
Go to :
 XML Download
XML Download