

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
The epidemiology of coronavirus disease 2019 (COVID-19) has changed continuously throughout the pandemic. These changes have been related to evolving public control policies, the introduction of variant strains, and the development of vaccines. Early in the pandemic, COVID-19 incidence was significantly higher in adults than in children.1 However, with the introduction of COVID-19 vaccines, reductions in infections and hospitalizations have been reported, particularly among high-risk populations.23 In South Korea, vaccination was initiated on February 26, 2021, for the prioritized groups, and vaccination was further expanded for the younger populations.4 On July 19, 2021, the BNT162b2 messenger RNA COVID-19 vaccine (Pfizer-BioNTech) was offered to all 12th-grade students (senior year in high school), and vaccination was further expanded to children aged 12–17 years on October 18, 2021.5 In addition, on October 29, 2021, the United States Food and Drug Administration issued an Emergency Use Authorization (EUA) for children aged 5–11 years and was approved for the EUA in Korea on February 23, 2022.67 Herein, we analyzed changes in the incidence of SARS-CoV-2 infection according to the age group in South Korea from February 2020 to December 2021.
Go to : 
METHODS
This was a retrospective observational study comprising all populations residing in or traveling to Korea who were diagnosed with COVID-19 through laboratory testing (reverse transcription-polymerase chain reaction; RT-PCR) from January 2020 to December 2021. We analyzed nationwide epidemiological data on age-based COVID-19 cases collected by the Korea Disease Control and Prevention Agency. The age distribution during the COVID-19 pandemic in Korea was analyzed by assessing the number of daily RT-PCR-confirmed COVID-19 cases. The age groups were classified as 0–4, 5–11, 12–17, and ≥ 18 years. The weekly incidence of SARS-CoV-2 infection per 100,000 individuals was calculated. The 7-day moving average of new cases (current day + 6 preceding days) was calculated to smooth the expected variation in daily case counts. The monthly age-adjusted incidence rate ratio (IRR) of SARS-CoV-2 infection in children by age group was compared with that in adults during the study period.
Ethics statement
This study was approved by the Institutional Review Board of Korea University Anam Hospital and the requirement for informed consent was waived (IRB. 2021AN0314).
Go to :
RESULTS
During the study period, among all the age groups, the population-based incidence was the highest in adults aged ≥ 18 years throughout 2020 (Fig. 1A). This trend continues until 2021, up to week 30 of 2021 (Fig. 1B). The COVID-19 vaccination campaign targeting adults started on February 26, 2021, and for adolescents on October 18, 2021 (Fig. 1A). From weeks 31–48 of 2021, the incidence in children aged 12–17 years was the highest among all the age groups and was later replaced by children aged 5–11 years from week 49 to the end of 2021.
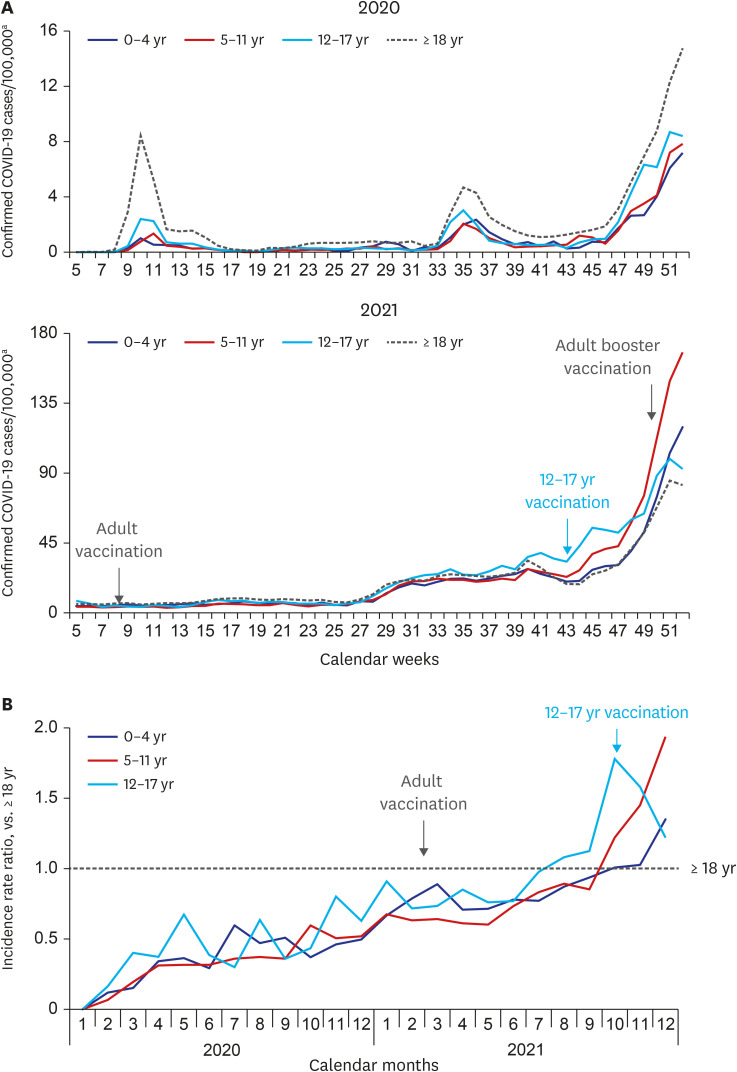 | Fig. 1Timeline of confirmed COVID-19 incidences by (A) age-specific weekly incidence, and (B) monthly age-adjusted incidence rate ratio in children by age group, in comparison to adults, South Korea January 2020–December 2021.COVID-19 = coronavirus disease 2019, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
aThe 7-day moving average of new cases (current day + 6 preceding days/7) was calculated to smooth the expected variation in daily case counts.
|
Throughout the study period, the incidence of COVID-19 was the highest during weeks 51–52 of 2021 for all ages. According to the age groups, the incidence was the highest in week 51 with 85 and 99 cases/100,000 population for adults aged ≥ 18 and children 12–17 years, respectively. The peak was the highest in week 52 of 2021, with 168 and 120 cases/100,000 population in children aged 5–11 and 0–4 years, respectively.
When comparing the monthly age-adjusted IRR of SARS-CoV-2 infection according to the age groups up to June 2021, the IRR in children was < 1 compared with adults (Fig. 1B). However, the IRR increased in 2021 compared with that in 2020, after the initiation of adult vaccination. The incidence of children aged 12–17 years exceeded that of adults in June 2021 and was 1.8 times higher than adults aged ≥ 18 years in October 2021. After the implementation of COVID-19 vaccination in children aged 12–17 years in October and booster shot for adults aged ≥ 18 years in November, the increase in incidence showed a trend towards decrease, and the age group with the highest incidence was replaced by children aged 5–11 years in December 2021 which showed 1.9 times higher incidence compared with adults.
Go to :
DISCUSSION
Since the COVID-19 pandemic, the incidence among adults aged ≥ 18 years was higher than all the other age groups in 2020; however, a shift toward younger ages occurred in June 2021. The increase in COVID-19 cases in children coincides with reports from other countries.689
Many reasons may be attributed to its increased incidence in children. Early in the pandemic, strong non-pharmaceutical interventions were implemented for children, including school closures and restrictions on extra-curricular activities.10 In addition, children have been reported to have a large proportion of asymptomatic infections, and severe cases are less common than in adults.1112 Therefore, children have a lower risk of exposure and may have been tested relatively less frequently than adults. Modifications and ease of public health control measures and the increase in prevalence in the community related to the introduction of SARS-CoV-2 variants have provided increased opportunities for exposure to COVID-19 in children.
The IRR of children compared with adults was < 1 from the beginning of the pandemic; however, it showed a turning point in July 2021. This was attributed to the increase in vaccine uptake in adults and the vaccination campaign for 12th-grade students in July. The vaccination campaign for 12th -grade high school students initiated in July reached a two doses vaccine coverage rate of 95.4% by August 2021.10 Thereafter, the incidence was the highest at aged 12–17 years, followed by aged 5–11 years, and showed a continuously increasing trend. However, after the initiation of vaccination in children aged 12–17 years, cases started to decrease at week 52 of 2021, in which vaccination rates were 67.8% for one dose and 46.3% for two doses in aged 12–17 years.13 The decrease in incidence in children aged 12–17 years and adults may be associated with social distancing policies and an increase in the third dose in adults (74.7% of adults ≥ 60 years).14
Understanding of COVID-19 has evolved during the pandemic. Early in the pandemic, when cases in children were low, it was proposed that children may be less susceptible to infection than adults.15 However, with the increase in exposure for children and the relative decrease in incidence in vaccinated populations, the incidence is currently the highest in children aged 5–11 and 0–4 years in South Korea since December 2021. Although children may have a relatively less severe clinical spectrum than adults, children aged 5–11 and 0–4 years serve as an important population of new COVID-19 cases in Korea. Between January 2020 and October 2021, eight critically ill pediatric patients with COVID-19 were admitted to the intensive care unit.16 Furthermore, cases of multisystem inflammatory syndrome in children (MIS-C) are expected to increase, necessitating careful monitoring of the adverse outcomes of pediatric COVID-19 in the coming season.
The increase in the incidence in children aged 5–11 years has various clinical implications. Young children are the only age group in which vaccines are not yet provided and may contribute to the transmission of SARS-CoV-2 in households and communities.17 Moreover, although the clinical spectrum may be less severe compared with adults, according to the analyses in the US, the cumulative COVID-19 associated hospitalization rate for children aged 5–11 years (28.6/100,000 population) has been reported to be similar to the influenza-associated hospitalization rate during 2017–2018, 2018–2019, and 2019–2020 influenza seasons (24.3–31.7/100,000 population).6 In addition, COVID-19 was reported as the eighth leading cause of death in children aged 5–11 years, and MIS-C most commonly occurs in this age group.6 Moreover, an increase in COVID-19 cases in children will lead to absences in parental workplaces.
This study is limited because the impact of various policies, such as social distancing or vaccine passes, which may have affected the changes in incidence in different age groups, was not analyzed. Moreover, our study did not reflect differences in vaccination rates between the adolescent age groups (i.e., 12–14 years vs. 15–17 years). Regardless, this study shows a change in incidence among the different age groups and shows that children aged 5–11 and 0–4 years have the highest incidence after the introduction of vaccines in other age groups.
In conclusion, we found significant changes in epidemiology after the introduction of SARS-CoV-2 vaccines in adults aged ≥ 18 years and children aged 12–17 years. Until recently, children were not regarded as the drive for the pandemic; however, children aged 5–11 and 0–4 years had the highest incidence among age groups. Therefore, policies for clinical support for an increase in COVID-19 cases among young children and age-specific preventive measures are needed.
Go to :
 XML Download
XML Download