

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since coronavirus disease 2019 (COVID-19) was first identified in December 2019, the outbreak has dramatically changed not only the medical field but also all aspects of society. Several vaccines have been developed and administered worldwide, but many countries still face difficulties containing the infection due to the rapid spread of variants, including B.1.617.2.12
COVID-19-related health issues, including complications and sequelae have been investigated with accumulated evidence from extensive research and clinical practices. Unsurprisingly, the pandemic has triggered a wave of mental health issues, with COVID-19 patients reporting social stigma and feelings of guilt.3 In addition, people have been reported to experience anxiety and depression due to socioeconomic impacts of the pandemic, a situation referred to as “corona blues”.4 Moreover, frontline healthcare workers (HCWs) caring for patients with COVID-19 are at risk of mental health problems related to the fear of becoming infected and burnout during this “never-ending” pandemic.5 Even before the emergence of COVID-19, several studies explored the psychological impact of epidemic diseases on HCWs during severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) outbreaks.67 According to previous studies, the levels of anxiety and stress increased among HCWs during the pandemic, highlighting the importance of psychosocial support. Several studies conducted during the first wave of the COVID-19 pandemic in China had similar findings.8 An observational study conducted in Korea also showed that HCWs reported significant depression and anxiety.9 As COVID-19 continues changing the course of the pandemic, it will continue affecting mental well-being and triggering anxiety.
Anxiety levels in HCWs have been associated with personal protective equipment (PPE) use behaviors.10 The fear of contracting COVID-19 has caused some HCWs to overestimate their need for PPE. SARS-CoV-2 spreads mainly through small liquid particles from an infected person’s mouth or nose. In specific situations such as aerosol-generating procedures, airborne transmission is also thought to be possible.11 Therefore, the current guidelines regarding PPE usage recommend wearing medical masks, gowns, gloves and facemasks when caring for COVID-19 patients, based on droplet and contact precautions, similar to the guideline for influenza prevention.12 However, some HCWs tend to use PPE excessively because they overestimate their risk of contracting COVID-19, even though the guidelines show that not so much is needed. In contrast, studies worldwide show that a shortage of PPE can cause anxiety among medical staff.1314 Therefore, appropriate access to PPE is imperative to help physicians feel physically safe.
Previous studies that explored anxiety among HCWs fighting against COVID-19 are limited to the early phase of the pandemic (February 2020),8 and significant changes have occurred since then, such as becoming accustomed to treating COVID-19 patients and developing immunity through vaccination. However, how these changes affect anxiety levels in HCWs has not yet been evaluated. In addition, earlier studies focused on psychological aspects, including anxiety among medical staff, risk factors contributing to emotional distress, and the importance of psychiatric management. To date, there is limited evidence on anxiety assessment of medical staff in the context of infection control. Therefore, we aimed at evaluating the relationship between anxiety levels and PPE use behaviors among HCWs caring for patients with COVID-19.
METHODS
Study design
This cross-sectional questionnaire study was conducted from July 1 to 31, 2021, at a municipal hospital in Seoul, South Korea, with 765 inpatient beds, including 195 nationally designated negative- pressure isolation units. During the 12 months periods prior to the study, the criteria for admission to the hospital did not change. Furthermore, the hospital conducted mass vaccination of HCWs in March 2021. Being a frontline HCW, either a doctor or a nurse, who treated patients with confirmed or suspected COVID-19, was the inclusion criteria. Study participation was promoted through posters in working spaces for HCWs. Participation was voluntary and anonymous by accessing the URL or QR code of the Google Surveys online questionnaire. The participants completed the questionnaire using a computer or smartphone (non-face-to-face communication).
We obtained basic information, including their age, sex, occupation type, working experience, and COVID-19 vaccination status. The degree of anxiety was evaluated using the self-rating anxiety scale (SAS), a clinical tool for analyzing subjective anxiety developed by W. Zung in 1971.15 SAS consists of 20 items measured on a 4-point scale. The score is calculated as the sum of the scores for the 20 items, and a high score indicates a high degree of anxiety. The Korean language version of Zung’s SAS was developed by Jung Hoon Lee.16 The test-retest reliability (coefficient r = 0.98, P < 0.001), and internal consistency (coefficient r = 0.96, P < 0.001) have been shown to be satisfactory.16 The mean SAS scores were assessed according to participant characteristics to evaluate risk factors for anxiety due to COVID-19.
In addition, the participants were asked questions about changes in their anxiety levels regarding: (a) becoming infected with SARS-CoV-2 while working; (b) spreading infection to their family; (c) experiencing financial difficulty due to infection; and (d) experiencing difficulty in caring for their children due to extended working hours. These variables related to anxiety about COVID-19 were selected based on literature review.17181920 Variables were compared between the period before and after March 2021, when the mass vaccination of HCWs was conducted. Participants rated the change in their anxiety level and perception after vaccination using a 5-point Likert scale: highly decreased, slightly decreased, neither decreased nor increased, slightly increased, and highly increased.
The type of PPE considered by the medical staff to be appropriate in each situation was investigated, and each situation was classified according to the US Centers for Disease Control and Prevention (CDC) guidelines.21 Exposure was first categorized as contact with the patients’ surroundings or with the patient directly, and the latter was further categorized by whether there was prolonged exposure or close contact, according to the guideline. Prolonged exposure was defined as exposure lasting 15 minutes or more. Close contact was defined as being within 6 feet of a person with confirmed SARS-CoV-2 infection or having unprotected direct contact with infectious secretions or excretions of a person with confirmed SARS-CoV-2 infection.
Respondents were allocated to two groups: “excessive demand for PPE” and “appropriate PPE use” groups, based on their answers about the appropriate type of PPE for each situation according to the current guideline.12 If respondents demanded more PPE than necessary (as indicated in the guideline) in any situation, they were assigned to the “excessive demand for PPE” group. In addition, to determine the characteristics of the participants with excessive demand for PPE, the basic characteristics of participants who used PPE excessively and the characteristics of those who did not were compared.
Data were collected on the monthly number of COVID-19 admissions and PPE supplies used in the study hospital over the 12-month period prior to the survey to determine changes in the PPE usage per patient during the previous year.
Statistical methods
Count data were expressed as number and percentage, and continuous data with normal-distribution were expressed as mean ± standard deviation. The amount of PPE used was corrected by dividing the corresponding number of hospitalized patients per month. Comparisons of anxiety levels measured by SAS between the two groups and stratified according to sex, profession, and vaccination status were performed using two independent-sample t-tests as normally distributed variables, and single-factor analysis of variance (ANOVA) was used to perform comparisons among multiple groups stratified by age, working experience, and level of exposure. Comparisons of basic characteristics of the participants according to PPE usage habits were performed using two independent-sample t-tests for SAS as normally distributed variables, and chi-square tests were used for the other variables. All statistical analyses were conducted using SPSS version 26.0 (IBM Crop., Armonk, NY, USA).
Ethics statement
This study was approved by the Institutional Review Board of Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 20-2021-62). Respondents were assured of anonymity and confidentiality, and web-based informed consent was obtained prior to the online survey.
RESULTS
Basic characteristics
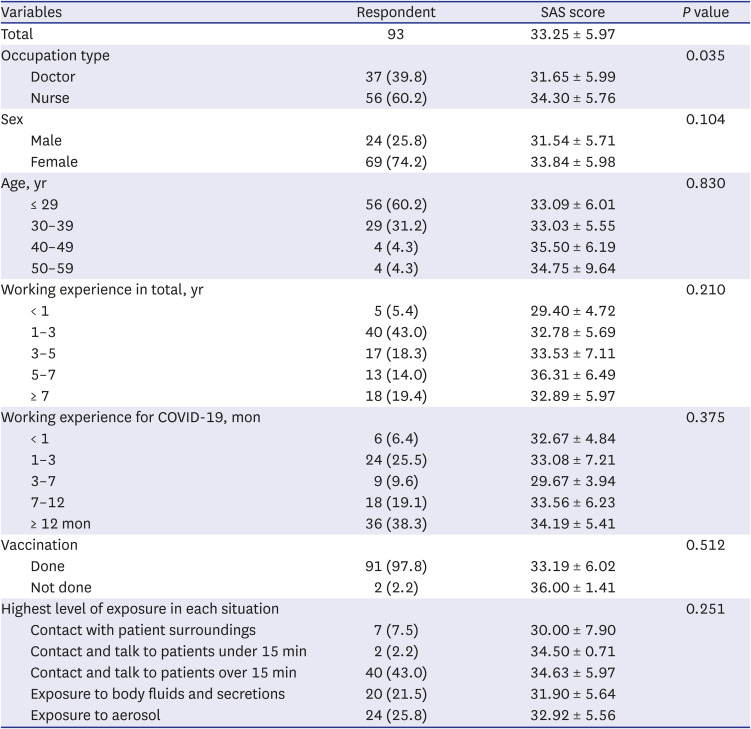
Of the 93 respondents, 24 were males (25.8%), and 69 were females (74.2%, Table 1). Thirty-seven were doctors (39.8%), and 56 were nurses (60.2%). Fifty-six (60.2%) were < 30 years old. Eighty-eight (94.6%) had a least 1 year of working experience, and 54 (57.4%) had more than 7 months experience of treating patients with COVID-19. All participants but two (91, 97.8%) were fully vaccinated against COVID-19. Eighty-six (92.5%) had direct contact with COVID-19 patients, and 24 (25.8%) participated in aerosol-generating procedures as their highest level of exposure.
Table 1
Basic demographic characteristics of the participants
Anxiety
The mean SAS score among participants was 33.25 ± 5.97 (range: 20–49) (Table 1). Four (4.3%) respondents had an SAS score of 44 or higher, indicating pathological anxiety disorder. Levels of anxiety differed significantly according to profession, but not according to age, sex, working experience, and level of exposure. Nurses had a higher mean SAS score than doctors (34.30 vs. 31.65, P = 0.035). Female, older aged and unvaccinated medical personnel showed higher SAS scores, but the difference was not statistically significant. Working experience and level of exposure were not associated with the level of anxiety about COVID-19.
Participants reported being less anxious about both contracting COVID-19 (68.8%) and spreading infections to their families (63.4%) (Fig. 1). The most common responses to questions about anxiety regarding financial crisis and caring for children were unchanged (Supplementary Table 1).

PPE use status and perception of PPE needed
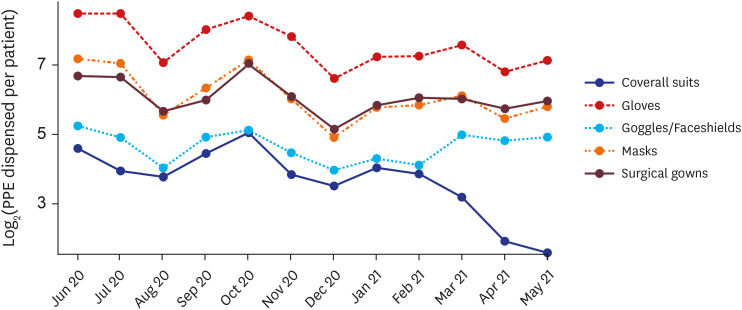
The use of PPE per patient decreased in 2021 compared to 2020 (Fig. 2). Regarding the use of coveralls, it was found that per person consumption dramatically decreased from 33.6 to 0. The use of goggles, face shields, and gowns, which can be used instead of coveralls, increased from January 2021. The use of goggles and face shields increased from 19.6 per patient in January 2021 to 29.9 per patient in May 2021, and the use of gowns increased from 57.1 per patient in January 2021 to 62.6 per patient in May 2021 (Supplementary Table 2).
Fig. 2
Monthly categorical personal protective equipment usage per patient during June 2020–May 2021 in the study hospital.
PPE = personal protective equipment.
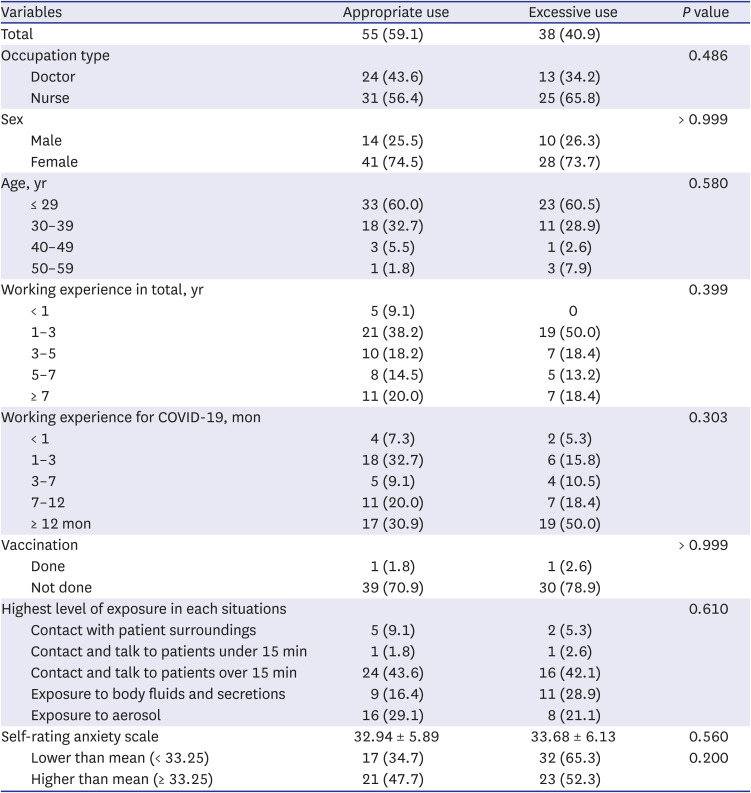
Data on the awareness of appropriate PPE use in each situation is shown in Table 2. Neither insufficient nor excessive demand for PPE was observed among those who had contact with patient surroundings. Most participants chose the appropriate level of PPE when they contacted and talked to patients for less than 15 minutes or were exposed to aerosols. However, some HCWs regarded the use of a powered air-purifying respirator, coverall, face shield, and gloves to be appropriate when they were in contact with patients for more than 15 minutes (n = 15, 16.1%), or when exposed to body fluids and secretions (n = 38, 40.9%; Supplementary Table 3), which is excessive according to the CDC guidelines. An excessive demand for PPE was observed, regardless of the degree of anxiety (Table 3). However, the proportion of HCWs who used more PPE than required according to their level of anxiety based on the mean SAS score, did not differ significantly (52.3% vs. 65.3% for higher and lower than average anxiety respectively, P = 0.20). Participants who tended to use PPE excessively did not differ from those who did not use PPE excessively in terms of their age, gender, occupation, working experience, vaccination status, and level of exposure. The mean SAS score was 33.68 ± 6.13 in the group with excessive PPE use and 32.94 ± 5.89 in the group without excessive PPE use, with no significant difference (P = 0.560).
Table 2
Awareness of appropriate personal protective equipment usage in specific situations

Table 3
Characteristics of the participants according to personal protective equipment use behavior
DISCUSSION
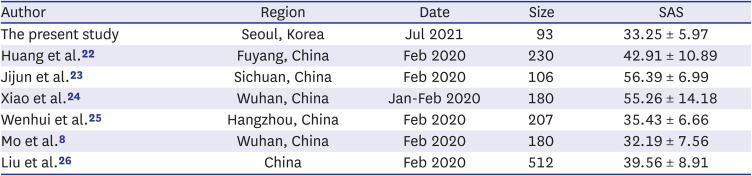
In this study, 70% of the respondents reported that their anxiety about infection and transmission of COVID-19 decreased when evaluated 1 year after the pandemic started and 4 months after vaccination was initiated. At the time of the study (July 2021), the mean SAS score was within the normal range. These results were supported by the diminished monthly usage of PPE and they are in alignment with what was reported in previous studies Table 4 shows the comparison of previous studies that used the SAS score to evaluate anxiety among frontline HCWs fighting against COVID-19.82223242526 This alleviation of anxiety levels was possibly due to a feeling of security because of immunity developed through vaccination, greater knowledge and clinical experience in managing patients with COVID-19, or both.
Table 4
Comparison of previous studies investigating the anxiety level by using SAS before vaccination
| Author | Region | Date | Size | SAS |
|---|---|---|---|---|
| The present study | Seoul, Korea | Jul 2021 | 93 | 33.25 ± 5.97 |
| Huang et al.22 | Fuyang, China | Feb 2020 | 230 | 42.91 ± 10.89 |
| Jijun et al.23 | Sichuan, China | Feb 2020 | 106 | 56.39 ± 6.99 |
| Xiao et al.24 | Wuhan, China | Jan-Feb 2020 | 180 | 55.26 ± 14.18 |
| Wenhui et al.25 | Hangzhou, China | Feb 2020 | 207 | 35.43 ± 6.66 |
| Mo et al.8 | Wuhan, China | Feb 2020 | 180 | 32.19 ± 7.56 |
| Liu et al.26 | China | Feb 2020 | 512 | 39.56 ± 8.91 |
The amount of PPE used per patient was also reduced during pandemic. The Korean guidelines on PPE for COVID-19 are based on the guidelines for responding to COVID-19 (for local governments) developed by the Korea Centers for Disease Control and Prevention. The 6th edition, dated February 20, 2020, presented for the first time the recommended range of PPE use for each situation. These recommendations remained unchanged until revised guidelines were released on January 3, 2022. In fact, a campaign regarding the appropriate use of PPE was carried out in the study hospital to encourage HCWs to wear appropriate PPE instead of coveralls, except when they were participating in aerosol-generating procedures. The campaign started on April 14, 2021; however, coverall usage had already decreased by 50% in March 2021 compared to the entire study period before March 2021 (9.11 vs. 18.45) and by 41% compared to January and February 2021 (9.11 vs. 15.48). Meanwhile, in the study hospital, COVID-19 mass vaccination was provided twice in the first and last weeks of March 2021, that is, so the timing of the sharp decrease in coverall usage coincided with the vaccination period. This trend of decrease in coverall use was maintained after April 2021, when the campaign began.
An excessive demand for PPE in specific situations remained. Some HCWs answered that they considered PPE equivalent to airborne protection to be appropriate, even in situations other than participation in aerosol-generating procedures. Although the overall use of coveralls decreased during the year, there is a need for further reductions in the inappropriate use of PPE.
There are many problems associated with the excessive use of PPE. First, wearing coveralls causes tiredness among medical staff when worn for a long time. Second, wearing coveralls incurs restrictions on medical procedures due to blunt movements when worn, and communication difficulties between medical staff.27 Finally, excessive use of PPE can cause a shortage of protective equipment. In countries such as the United States and European countries, there was a serious shortage of PPE due to the rapid increase in the number of COVID-19 patients. Accordingly, authorities, including the CDC recommended strategies to optimize PPE supplies in healthcare setrtings, to be used during periods of anticipated PPE shortage.2829 Therefore, it is important to manage the use of PPE preemptively and to identify and address the causes of excessive use of PPE.
Some participants in this study showed excessive PPE usage behavior. This tendency was observed regardless of age, gender, occupation, working experience, or level of exposure. Because there was no difference in the length of occupational experience between the “excessive” and “appropriate” PPE use groups a, occupational proficiency did not account for this difference. In addition, anxiety measured by SAS did not explain excessive PPE use. Presumably, as the characteristics of the hospitalized patients did not change, it is possible that the experience of dealing with COVID-19 patients led to the increasing selection of appropriate PPE by HCWs, considering that the use of PPE gradually decreased for one year compared to the earlier period of the pandemic.
Our results were in accordance with those of previous reports on the importance of mental health care of HCWs during a pandemic. The anxiety levels among medical staff investigated in this study decreased after vaccination, compared to the findings of previous studies. However, proper intervention and management are still required to address excessive needs for overprotection among some HCWs.
This study had a limitation in that ongoing changes in the course of the COVID-19 pandemic make it difficult to predict the transition of anxiety levels among HCWs and guidelines for PPE are changeable depending on the circumstances of COVID-19.
In conclusion, this study assessed the anxiety levels of HCWs exposed to COVID-19 after a year of pandemic and investigated their perception of the need for PPE use. To the best of our knowledge, this is the first study to assess PPE use among HCWs in relation to anxiety.
 XML Download
XML Download