

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Human immunodeficiency virus (HIV) status disclosure is an act that not only has an important personal meaning to people living with HIV/acquired immunodeficiency syndrome (AIDS) (PLWH) but also has a social significance. Disclosure can be a first step to allow PLWH to access social support.1 Additionally, this can lead to safer sexual behavior that prevents the seroconversion of HIV-negative individuals,2 better adherence to antiretroviral therapy (ART), and less treatment failure.3 Despite these positive effects, disclosure can be a huge challenge to PLWH because it is associated with risks that lead to negative outcomes. It can lead to stigmatization, rejection, avoidance, physical harm, and negative social interactions, such as workplace discrimination. Additionally, it can impair psychosocial well-being in PLWH.45 Nevertheless, numerous studies report greater positive effects of disclosure than negative. In addition, previous studies have shown that PLWH usually do not regret their disclosure, which also supports its importance.67
Depression is the most common psychiatric complication among PLWH; it is more than twice as prevalent than in the general population.8 Anxiety is also prevalent among PLWH. Previous studies have shown that these psychiatric complications are associated with risky sexual behavior, disease progression, and higher mortality rates among PLWH.910 Emotional well-being is an important factor influencing disclosure; several studies have tried to clarify this correlation. However, the evidence is mixed in differing study designs or differs according to the background of the participant group.511 HIV-related stigma is common among PLWH, which can lead to a loss of affective, behavioral and physical well-being.12 Many studies, including one meta-analysis, have confirmed the negative correlation between perceived HIV-related stigma and disclosure in various research settings.513 Taken together, these data indicate that depression, anxiety, or stigma can act as major predictors of the disclosure of HIV status.
There may be common disclosure barriers worldwide; however, social context may account for some differences. A previous study has reported that race, ethnicity, and culture may play a role in the effects of disclosure.14 Therefore, it can be assumed that disclosure behavior barriers can be attributed to cultural differences. Studies dealing with HIV status disclosure have been conducted worldwide; however, to date, few studies have been conducted in South Korea. This lack of information means that the obstacles to the positive perception of disclosure are unknown. This can make it difficult to promote disclosure despite its many advantages. In the unique culture of Korea, people are reluctant to discuss sexual minorities or sexually transmitted infections; therefore, different barriers are expected compared with other countries.15 This study aimed to investigate the associated characteristics of HIV status disclosure in PLWH living in South Korea, including demographics, and clinical and psychosocial factors.
METHODS
Participants
The participants were 147 PLWH who visited the outpatient infection clinic in Kyungpook National University Hospital (KNUH), Daegu, South Korea, between June 2020 and January 2021. The inclusion criteria were: patients who had been diagnosed with HIV infection; currently being treated with an ART regimen; aged ≥ 20 years; able to provide written informed consent; and able to read and write in Korean.
Sociodemographic and clinical data
The demographic information of participants was reported, including age, gender, marriage, employment, monthly income, education, religion, HIV transmission route, experience with AIDS-related diseases, ART period from start, and ART adherence. This was measured using the question, “How often have you missed your medication in the last four weeks?” Responses were dichotomized as “Very good” if the answer was not more than once and “Not very good” if the answer was more than once. Clinical data were extracted from the patient medical records. Total CD4 T cell counts (cell/μL) and HIV quantitative reverse transcription polymerase chain reaction (RT-PCR, copies/mL) were included.
Disclosed and non-disclosed group
Before starting the psychiatric measures, all participants were asked to answer the following question, “Have you ever informed anyone around you of your HIV infection?” Participants who had no experience in informing other people about their HIV/AIDS status were classified into the ‘non-disclosed group’ and others who had experienced disclosure were classified into the ‘disclosed group’. The participants of the non-disclosed group did not complete the ‘enacted stigma’ subscale in HIV Stigma Scale (HSS), which represents an experience-induced stigma among PLWH.
Measures
HIV related stigma
The revised HIV Stigma Scale (HSS-R) were used in this study.16 Several recent studies that have noted the stigma related to HIV use this measure.1718 The HSS was first designed to measure the stigma perceived by individuals who were HIV-positive.19 The HSS-R, which was used in this study, has been shortened from the original 40 items to 32. It consists of four subscales: disclosure concerns, negative self-image, concern with public attitudes, and enacted stigma. Disclosure concerns are related to the perceived need to keep one’s own HIV information concealed. The negative self-image provides information about the feelings of guilt or shame of HIV-positive individuals have about being HIV infected. Concern with public attitudes relates to the beliefs that HIV-positive individuals have about other people’s opinions of them. Enacted stigma relates to the reactions from other individuals after HIV status disclosure. This is also related to the experience of rejection. This subscale was measured in the disclosed group alone.
Items for each subscale were rated using a four-point Likert scale ranging from 1 (strongly agree) to 4 (strongly disagree). In total, 32 items showed good overall internal consistency (0.897), which was measured using Cronbach’s alpha. Disclosure concerns (0.785), negative self-image (0.822), and concerns with public attitudes (0.834) showed good internal consistency. Enacted stigma (0.933) showed an excellent level of internal consistency. Bunn et al.16 has shown that Cronbach’s alpha for these subscales range from 0.90 to 0.97, with an overall value of 0.95.
Depression
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9); we used the validated Korean version of the PHQ-9.20 Several studies that assessed depression in HIV-positive individuals have used this measure.1718 The PHQ-9 scale is half the length of many other depression measures and consists of nine criteria upon which the diagnosis of 4th Edition of Diagnostic and Statistical Manual of Mental Disorders major depressive disorder is based. It assesses how often the participants are bothered by symptoms related to depression in a two-week period. Nine items were scored using a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). Total scores ranged from 0–27. High scores indicate a more severe degree of depression.
Anxiety
Anxiety symptoms were measured using the Generalized Anxiety Disorder-7 (GAD-7); the validated Korean version of GAD-7 was used in this study.21 Using a 4-point Likert scale from 0 (not at all) to 3 (nearly every day), participants were asked how often they experienced feelings of nervousness, worry, or restlessness in the past two weeks. Total scores ranged from 0–21. The higher the score, the higher the degree of anxiety.
Statistical analysis
First, preliminary analyses were performed to identify significant group differences within the sample. The χ2 tests were conducted using the categorical variables – gender, marriage, employment, monthly income, education, religion, HIV transmission route, experience with AIDS related diseases, and ART adherence. Fisher’s exact test was applied when > 20% of cells had expected frequencies lower than 5. Independent two sample t-tests were conducted for the continuous variables – ART period from start, total CD4 T-cell count, HIV quantitative RT-PCR, disclosure concerns, negative self-image, concern with public attitudes, depression, and anxiety. Pearson’s correlation analysis was conducted for continuous variables, including enacted stigma.
Second, logistic regression analysis was performed to determine the predictors for non-disclosure of HIV serostatus. All the sociodemographic, medical, and psychological variables investigated in this study were included in the analysis to determine potential explanatory variables.
All statistical analyses were performed using SPSS version 21 for Windows (IBM Co., Armonk, NY, USA).
RESULTS
Participant sociodemographic, clinical, psychiatric characteristics
The mean age of participants was 42.7 ± 12.5 years with the majority being male (n = 142, 96.6%). Most participants were single (68%), employed (65.3%), had a monthly income of 3 million won or less (66.7%), no religion (65.3%), did not experience AIDS-related diseases (68.7%), had a very good ART adherence (89.8%), and had disclosed their HIV serostatus to others (61.2%). Almost half of the participants reported their HIV transmission route via homosexual or bisexual behavior (45.6%). There were similar proportions of participants who continued their education after high school and those who did not. The mean ART period was 71.3 ± 58.6, CD4 T-cell count (cells/µL) was 610.3 ± 428.7, and HIV quantity using RT-PCR analysis was 8,544.9 ± 87,642.9 copies/mL. For the psychiatric measures, the mean PHQ-9 and GAD-7 scores were 5.9 ± 6.3 and 4.4 ± 4.8, respectively. The mean HSS-R disclosure concern score was 25.2 ± 5.1. The negative self-image and concern with public attitudes scores were 17.8 ± 4.9 and 19.0 ± 4.2, respectively. Additionally, the mean enacted stigma among HIV serostatus disclosure group score (n = 90) was 23.2 ± 8.5 (Table 1).
Table 1
Demographic, clinical data and psychiatric measures of the study sample (N = 147)
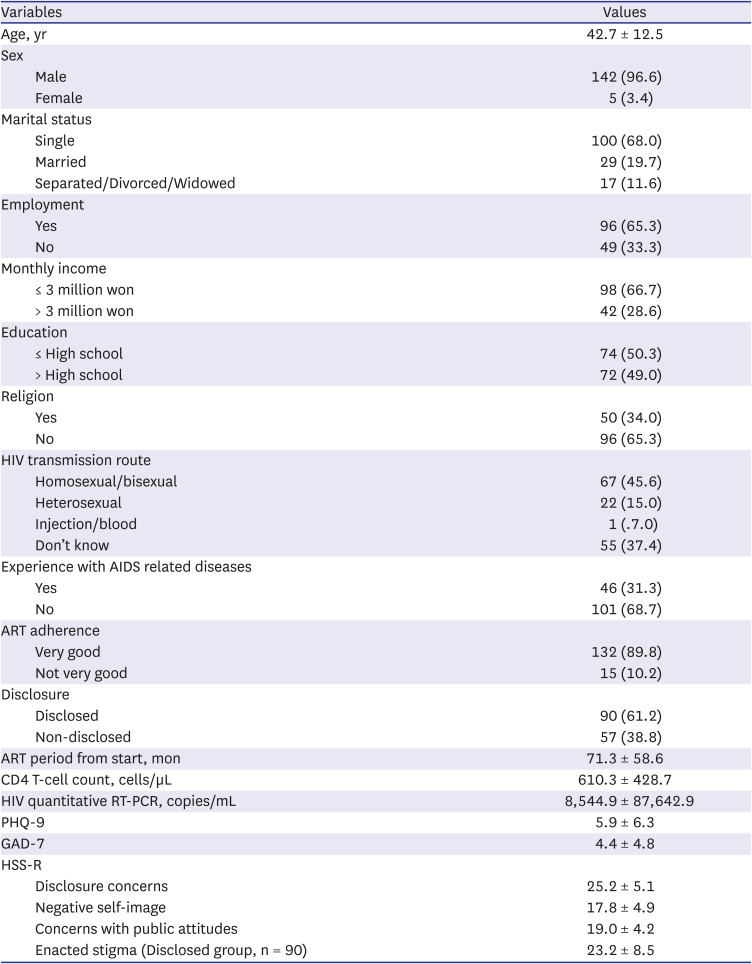
Values are expressed as mean ± standard deviation or number (%).
HIV = human immunodeficiency virus, AIDS = acquired immunodeficiency syndrome, ART = antiretroviral therapy, RT-PCR = reverse transcription polymerase chain reaction, PHQ-9 = Patient Health Questionnaire-9, GAD-7 = Generalized Anxiety Disorder-7, HSS-R = revised HIV Stigma Scale.
The medical and psychosocial factors between the disclosed and non-disclosed groups
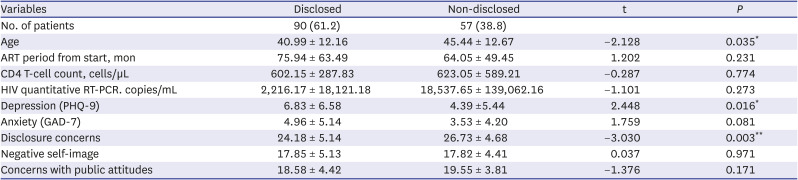
There was decreased disclosure in individuals who were married (P < 0.001) and had higher education levels (P = 0.046). Additionally, Depression (PHQ-9) (P = 0.016) was lower in the non-disclosed group than in the disclosed group. By contrast, age (P = 0.035) and disclosure concerns (P = 0.003) were higher in the non-disclosed group than in the disclosed group (Tables 2-4).
Table 2
Results of χ2 test comparing the medical and psychosocial factors between disclosed and non-disclosed group
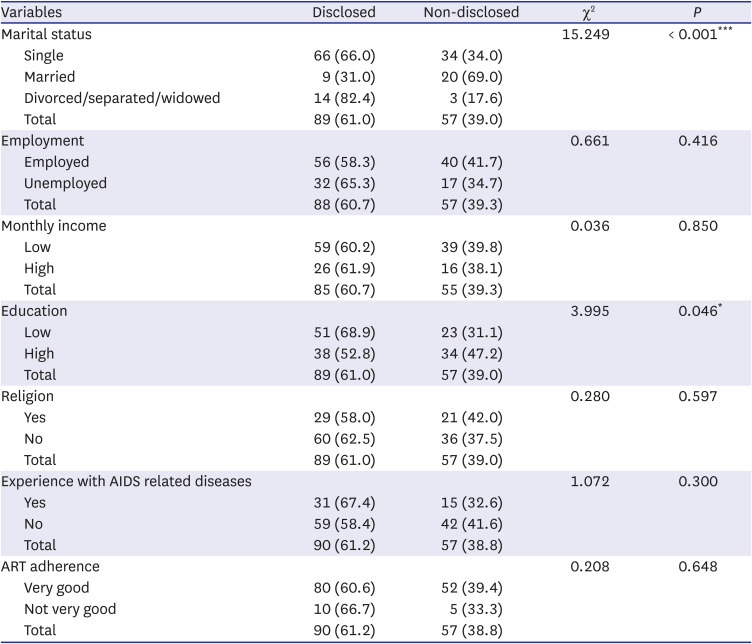
Table 3
Results of Fisher’s exact test comparing the medical and psychosocial factors between disclosed and non-disclosed group
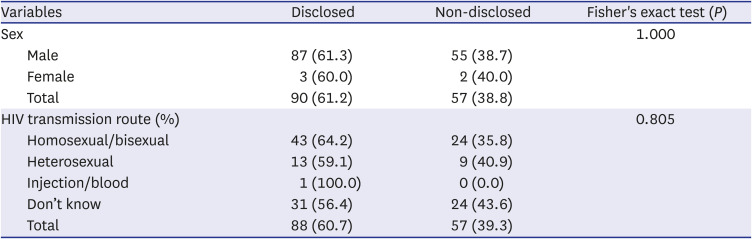
Table 4
Results of independent two sample t-test comparing the medical and psychosocial factors between disclosed and non-disclosed group
Correlation analysis of continuous variables
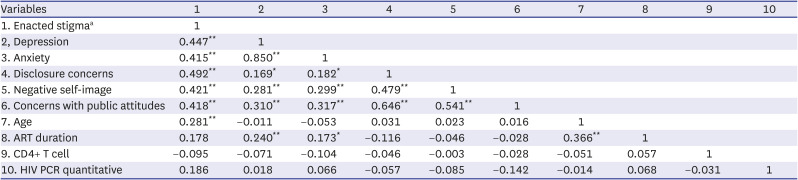
Enacted stigma, measured in the disclosed group alone, was significantly correlated with depression (r = 0.447), anxiety (r = 0.415), disclosure concerns (r = 0.492), negative self-image (r = 0.421), concerns with public attitudes (r = 0.418), and age (r = 0.281). Depression, measured in both groups was significantly correlated with anxiety (r = 0.850), disclosure concerns (r = 0.169), negative self-image (r = 0.281), concerns with public attitudes (r = 0.310), and ART duration (r = 0.240). Anxiety, measured in both groups, was correlated with disclosure concerns (r = 0.182), negative self-image (r = 0.299), concerns with public attitudes (r = 0.317), and ART duration (r = 0.173). Disclosure concerns were significantly correlated with negative self-image (r = 0.479) and concerns with public attitudes (r = 0.646). In addition, negative self-image and concerns with public attitudes were significantly correlated (r = 0.541). Participants’ age showed some correlation with ART duration (r = 0.366; Table 5).
Table 5
Results of Pearson correlation test for continuous variable
The predictors of non-disclosure of HIV serostatus
Logistic regression analysis indicated that lower depression (odds ratio [OR], 0.918; P = 0.021) and higher disclosure concerns (OR, 1.133; P = 0.004) were significant predictors of non-disclosure. Further, marriage was a major predictor of non-disclosure when unmarried individuals were referred (OR, 3.002; P = 0.024), but divorce, separation or widow had no significant consequences (Table 6).
Table 6
Results of Logistic regression analysis for factors predicting HIV status non-disclosure

DISCUSSION
Our study showed that the age and gender distribution of participants were similar to a previous HIV/AIDS cohort study conducted in South Korea.22
As shown in the results, 61.2% of our study participants disclosed their HIV serostatus to at least one person. Similarly, a recent study of HIV disclosure in South Korea showed that only 54.7% of 148 participants reported disclosing their HIV status to their most trusted supporter.15 This is a significantly lower disclosure rate compared with studies that have been conducted in other countries. Previous research conducted in 12 countries over 5 continents have shown that 96% of respondents report having disclosed their HIV status to at least one person. The disclosure rate of other continents, except Asia-Pacific, is ≥ 90%. By contrast, the rate in the Asia-Pacific continent was 85%. Additionally, only 71% of 100 participants of South Korea reported their HIV status disclosure.6
There might be several factors that influence the low disclosure rate in Korea. A major influence is the difference in social perception and disease stigma between different countries and cultures. In our study, disclosure concerns were a significant in predicting non-disclosure. Disclosure concern is a perceived social stigma of PLWH that is closely related to the actual social perception of the disease. The social discrimination and stigma against HIV positive individuals remains a problem worldwide; however, this problem is more serious in Korea. A survey released in 2019 by the Korea Center for Disease and Prevention has reported that 52.4% of the 1,000 respondents said that they are reluctant to eat with individuals with HIV.23 This result is different from the results of a US report assessing stigmatizing attitudes, which found that only 17.5% of respondents stated that they were afraid of casual contact with PLWH.24 In a previous study, Asian-Pacific responders, including South Korea and Australia, reported more perceived stigma than other continents’ responders. For example, they thought that other people believed HIV-infected individuals engaged in risky behaviors, such as sexual promiscuity, prostitution, or drug use.6 This higher perceived stigma is shown in our study; the disclosure concern, concerns with public attitudes, and negative self-image subscale scores were higher in all participants than in the results of a previous study conducted in the US.16 Previous studies have shown that increased perceived stigma is predictive of non-disclosure in PLWH.525
In our study, as a result of the Fisher’s exact test, there was no statistically significant difference between the disclosed and non-disclosed groups depending on the route of infection (Table 3). A small number of previous studies have studied the correlation between the disclosure of HIV serostatus and HIV transmission route, and studies on this have not been known in Korea. One study conducted in China suggested that in the case of individuals infected by sexual activity, there was a tendency to disclose their HIV status less than those infected by injection drug use (IUD) or blood transfusion. And it was interpreted that this may be the fear of participants infected by sexual activity receiving ethical criticism such as promiscuity from others after disclosure.25 Other study conducted in Taiwan showed that the disclosure rate to at least one other person was higher in order of men having sex with men (MSM), heterosexual, and injection drug users. And it was interpreted that people with injected drug use would often not be able to gain support from their families due to their existing criminal history of illegal drug use.26 In our study, only one person answered that there was an infection caused by blood or injection, and 37.4% of the respondents said they did not know the route of infection. In the future, if more participants are studied in multiple organizations, different research results could be obtained.
In this study, participants with more depressive symptoms tended to disclose their HIV status. Our finding appears to be contradictory to some of previous studies, as those studies show that HIV disclosure is inversely related to depression or depressive symptoms. One study of HIV diagnosed African American women showed that perceived support from others and satisfaction with support mediated HIV disclosure and depression, HIV disclosure to others and depression were inversely correlated.27 Another study of HIV patients in Uganda, showed that general disclosure and depression were negatively correlated.28 The study with newly HIV-diagnosed MSM showed that depressive symptoms were negatively associated with disclosure to their sexual partners.29 However, these previous studies can be said to be different from our study results in that they are obtained by subdividing the disclosure targets or the participants were limited to specific regions or genders. In this respect, our research results have something to understand more in the cultural context of Korea.
One hypothesis for our result is that disclosure may be the cause of depression but can be a result of it. Therefore, disclosure may occur in order to seek support in coping with depressive symptoms or the result of experienced stigma. And this assumption can be said to be in line with the result of one previous study which showed the positive correlation with HIV disclosure and depression.30 We found that enacted stigma, which is a measure of experienced discrimination, had a higher association with depression than any other stigma subscales. Therefore, it is possible that depression is exacerbated by experienced stigma. Further, the positive association between enacted stigma and depression are shown in several previous studies.3132 Another assumption is that non-disclosed participants tend to have difficulty revealing their depressive symptoms honestly, especially in individuals who find it difficult to reveal themselves to others. To support this hypothesis, further investigation into characteristics of this group is required. One review article has suggested that there is mixed evidence for the relationship between disclosure and psychological well-being. They argue that disclosure alone does not appear to benefit psychological well-being. Additionally, there may be a mediating process, including social support. Further studies examining this processes may provide this important information.5
The results showed that marriage is a major predictor for non-disclosure. A previous study indicated that 83% of all respondents in 5 continents disclosed their HIV status to their spouse or partner. By contrast, only 45% of South Korean respondents in this study shared their HIV status with their sexual partner. This may be due to the higher tendency to link HIV infection to sexual promiscuity in Pan-Asia than in other continental cultures. This may be a significant barrier in status disclosure for married people. Further, this may be related to the fears that disclosure would cause the loss of family or friends, which are significantly higher in the Asia-Pacific continent compared with other regions.6 According to a recent HIV-related perception and behavior survey, most Koreans perceive HIV infection as a filthy, shameful, and unspeakable disease.23 This negative perception of the disease in Korea might cause married people not to disclose their HIV status to their spouse. Some studies have suggested that the greater intimacy of a relationship rather than the sexual partnership itself can be important factor in disclosure.3334 This implies that both marital status and intimacy with the spouse can affect disclosure. Further research is required to confirm this.
Additionally, higher levels of education and older age were related with non-disclosure; however, they were not revealed as predictors of non-disclosure in the logistic regression analysis. Previous studies have shown a correlation between higher education level and lower disclosure rate, which might be influenced by higher self-stigma and cause a fear of disclosure.2335 Another hypothesis is that highly educated people are more likely to have a high income and high employment security when compared with low educated people.36 These people may feel at greater risk of losing a stable job if they disclose their HIV status. Furthermore, several previous studies have suggested that older adults are more likely to not disclose their HIV status when compared with younger adults.3738 This age difference may be attributed to the tendency of older adults to think that behavior related to HIV risk is morally wrong when compared with younger adults. Therefore, they are more concerned about public stigma.39 However, the difference in mean age alone cannot be considered to reflect the difference in other age groups. Further studies are necessary to elucidate this.
There are several limitations in this study. First, there may be a selections bias in including the participants in the study. There is a possibility that the individuals who did not cooperate with the survey may be more reluctant to reveal their status or that their physical or emotional conditions were poor. Second, the study was based in a single center; therefore, further studies that include a larger sample size with multiple centers are required to validate our findings. Finally, this cross-sectional study can only reflect a correlation in the data. Causal inferences would require a longitudinal study. Despite these limitations, this study is of great significance because, to the best of our knowledge, it is one of the first studies to examine the factors that predict the disclosure of HIV status in Korea. Furthermore, we have shown differentiated results when compared with studies conducted in other countries.
Taken together, our data show that the rate of HIV disclosure is lower in South Korea than in other countries. The higher disclosure concerns, lower depression and married state were suggested to be important predictors of HIV non-disclosure. Higher disclosure concerns might be related to the perceived stigma of PLWH. The discrimination and stigma experienced by the people in disclosed group may have influenced their depression, or the depressed people may have sought to gain support by disclosing their illness. The cultural atmosphere that links HIV infection with sexual promiscuity may have prevented married people from disclosing their disease. Considering these predictors, it is a very important task to create a social atmosphere in which PLWH can relieve concerns about social prejudice and discrimination. Education continues to reduce the stigma of HIV and promote knowledge at the national level in South Korea. Recently, a reduction in personal levels of stigma and increased knowledge about HIV infection has been shown; however, the social stigma remained problematic.2340 Nationwide efforts should continue in the public and health care institutions to reduce overall stigma and create a social environment where PLWH feel safe to disclose their disease status.
 XML Download
XML Download