

 PDF
PDF Citation
Citation Print
Print



The number of patients with ulcerative colitis (UC) has increased recently in South Korea and other Asian countries, where the disorder was once considered rare.123 Treatment of moderate to severe UC is based on immunosuppression using compounds such as steroids, immunomodulators, and biologics. Tofacitinib is an oral Janus kinase (JAK) inhibitor authorized for the treatment of UC. The efficacy and safety of tofacitinib in adults with moderate to severe UC have been evaluated in clinical studies.45 Tofacitinib was approved for such patients in South Korea on May 1, 2019. However, it has several safety issues. Several adverse events of interest have been reported: infection (severe or opportunistic; herpes zoster [HZ]), major adverse cardiovascular events, malignancy, thromboembolic events.6 The U.S. Food and Drug Administration announced a warning about the increased risk for serious heart-related events, cancer, blood clots and death for JAK inhibitors for the treatment of chronic inflammatory conditions, including UC, on September 1, 2021. UC is an independent risk factor for venous thrombosis.789 The incidence of venous thrombosis in an Asian population was lower compared to a Western population.101112 Therefore, there is a need for research on JAK inhibitor-related thromboembolic events in Asians. Tuberculosis (TB) is another important issue in South Korea because of its high prevalence.13 In one study, active TB associated with tofacitinib was reported in 0.5% of rheumatic arthritis (RA) patients, most of them in epidemic areas.14
We evaluated the safety of tofacitinib in moderate to severe UC by analyzing the National Health Insurance Service (NHIS) database. We used the diagnostic codes defined by the International Classification of Diseases, tenth revision (ICD-10) and the V code in the rare intractable diseases database.15
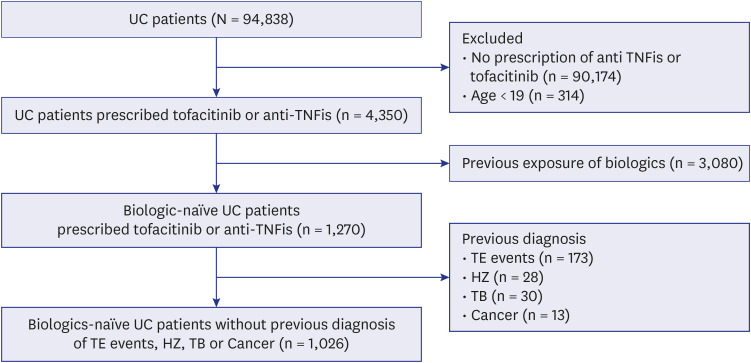
We enrolled UC patients identified by ICD-10 (K51.x) and V code (V131) from the NHIS database for May 1, 2019, to April 30, 2021. Tofacitinib was approved for the treatment of moderate to severe UC in Korea on May 1, 2019. To identify such patients, eligible patients were restricted to those prescribed an anti-TNF inhibitor (infliximab, adalimumab, golimumab) or tofacitinib. We also excluded those aged < 19 years; individuals with previous exposure to biologics or JAK inhibitors; and those with a previous diagnosis of major cardiovascular events (unstable angina [UA], acute myocardial infarction [AMI], congestive heart failure [CHF]), other thromboembolic events (ischemic stroke, pulmonary thromboembolism [PTE], deep vein thrombosis [DVT]), HZ, TB, or cancer (Fig. 1).
Demographic features (age, sex, duration of disease), comorbidities, and UC medication use were collected. Comorbidities included hypertension (ICD-10 code, I10.x–I15.x), diabetes mellitus (E10.x–E14.x), chronic renal failure (N18.x), and liver cirrhosis (K74.x). We also collected data on UC medications, including 5-aminosalicylic acid, immunomodulators (azathioprine, mercaptopurine, cyclosporine, tacrolimus, and methotrexate), steroids, biologics (infliximab, adalimumab, golimumab, vedolizumab), and JAK inhibitors.
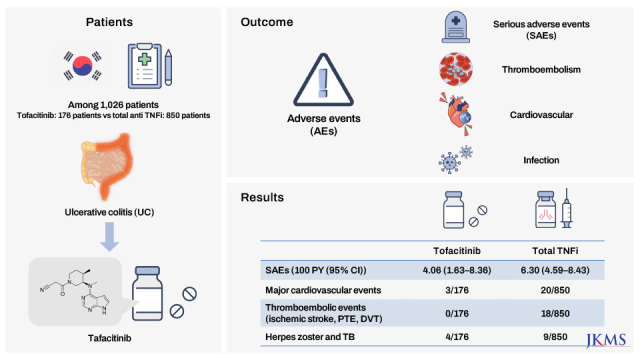
Patients were divided into tofacitinib and anti-TNFi groups, and we estimated the incidences of serious adverse events (SAEs) in the two groups. SAEs were defined as major cardiovascular events, other thromboembolic events, HZ, and TB. Major cardiovascular events included UA (I20.0, hospitalization/outpatient), AMI (I21.x, hospitalization), and CHF (I50.x, hospitalization/outpatient). Other thromboembolic events included ischemic stroke (I63.x–I64.x, hospitalization), PTE (I26.x, hospitalization/outpatient) and DVT (I80.x, hospitalization/outpatient). HZ was detected using ICD-10 codes and based on medication use (B02.x and antiviral agents, respectively). TB was detected based on the V code (V000, V206, V246) and use of anti-TB medications.
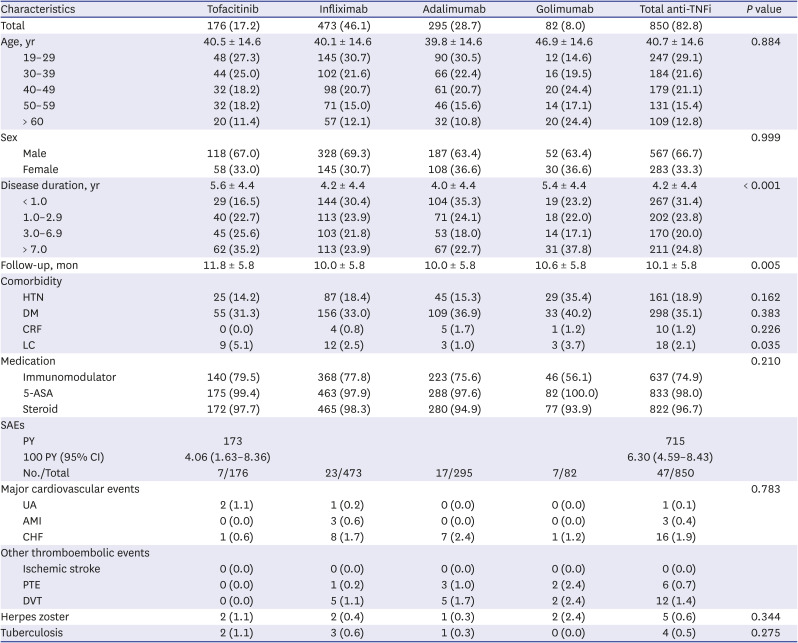
We reviewed a total of 94,838 UC patients from May 1, 2019 to April 30, 2021. Of these, 1,026 UC patients were enrolled and analyzed in this study (Fig. 1). The tofacitinib and anti-TNFi groups included 176 (17.2%) and 850 (82.8%) UC patients, respectively. The anti-TNFi group was subdivided into infliximab, adalimumab, and golimumab groups (473 [46.1%] vs. 295 [28.7%] vs. 82 [8.0%]). The mean patient age did not differ between the two groups (40.5 ± 14.6 vs. 40.7 ± 14.6 years, P = 0.884). The disease duration was longer in the tofacitinib group than the anti-TNFi group (P < 0.001). Overall comorbidity and medication history did not differ between the two groups.
The overall incidences (100 person-years; 95% confidence interval) of SAEs were 4.06 (1.63–8.36) and 6.30 (4.59–8.43) in the tofacitinib and anti-TNFi groups, respectively. In the tofacitinib group, major cardiovascular events occurred in three patients (two UA and one CHF). CHF was more common in the anti-TNFi group, but there was no statistical significance. No thromboembolic event, such as ischemic stroke, PTE, or DVT, occurred in the tofacitinib group. PTE and DVT occurred in 6 (0.7%) and 12 (1.4%) patients, respectively, in the anti-TNFi group. The incidence of HZ and TB did not differ between the two groups (Table 1).
Three patients with major cardiovascular events had DM and one patient had DM and hypertension. Of them, two patients were hospitalized for 3 and 7 days, respectively. The numbers of days to major cardiovascular events were 320, 122, and 126. HZ and TB occurred in four patients, and the average number of days to the events was 380. (Table 2).
There was no difference in the incidences of major cardiovascular events between the tofacitinib and anti-TNFi groups. There were 20 major adverse cardiovascular events among patients receiving any TNFi, for an incidence of 0.51 per 100 person-years in the UC trial-like cohort, compared with 0.28 per 100 person-years (seven patients with major cardiovascular events) in the tofacitinib UC clinical trial overall cohort.16 In a recent study of RA patients, the rate of major adverse cardiovascular events was 0.4 per 100 person-years.14 Our results are similar to those findings. There were two patients with UA and one with CHF among 176 patients in the tofacitinib group. Interestingly, CHF was more common in the anti-TNFi group than the tofacitinib group, albeit the difference was not statistically significantly. An association between anti-TNF agents, such as infliximab and adalimumab, and CHF has long been established.17 Our findings support that notion. In addition, the three patients with major cardiovascular events had DM and were older than the mean age of the study population. Therefore, we suggest caution when using tofacitinib in elderly and diabetic patients.
Pulmonary embolism and DVT, now the most important issue related to tofacitinib, were not found in this study; also, there were no cases of ischemic stroke. These findings do not correspond with recent reports of thromboembolic events in moderate to severe UC patients using tofacitinib.1819 However, a recent study that used claims data reported no pulmonary embolism or DVT but their rates were numerically higher in TNFi-treated patients, as in this study.16 The discrepancy may have one or more of several possible explanations. First, tofacitinib was approved recently for the treatment of moderate to severe UC. Therefore, it is possible that the observation period was too short to confirm the occurrence of thromboembolic events. Second, UC is an independent risk factor for venous thrombosis, the incidence of which in an Asian population was lower compared to a Western population. Third, there was no analysis of patients treated with both tofacitinib and TNFi. This study also had strengths. This is the first comparative study of tofacitinib-related SAEs in South Korea. More importantly, we enrolled only biologic-naïve patients to minimize the impact of previous use of biologics.
The HZ and TB rates were not different between the tofacitinib and anti-TNFi groups. This finding for HZ is similar to other clinical trials, in which the safety of tofacitinib was similar to that of TNFis.620212223 The incidence of TB was numerically low, although TB has a high prevalence in South Korea. Therefore, a latent TB test should be conducted before using tofacitinib or TNFis in South Korea; if the result is negative, those agents can be used.
This study had a major limitation. Although we estimated the person-year data of the incidence of overall SAEs, we could not do so for the person-year data of the incidence of each SAE, because there were no thromboembolic events in the tofacitinib group and a small number of adverse events (HZ, TB).
In conclusion, there was no difference in the overall incidence of SAEs, including thromboembolic events, between tofacitinib- and TNFi-treated UC patients. Therefore, tofacitinib can be used for moderate to severe UC with a similar risk profile to TNFis. However, the follow-up duration was insufficient to evaluate the incidences of SAEs. Collection and analysis of further data are necessary.

 XML Download
XML Download