

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Today, as the digital revolution is becoming a global trend, the importance of digital healthcare that combines information and communication technology and health care services is rapidly increasing worldwide. Moreover, Pear Therapeutics' digital therapeutics (DTx) “reSET” for the treatment of substance use disorder was approved by the US Food and Drug Administration (FDA) for the first time in the world,1) digital healthcare is expanding from wellness to disease prevention or management and even treatment. Especially, as awareness of non-contact healthcare has improved due to coronavirus disease 2019 (COVID-19) pandemic, interest in DTx that treat patients using digital technologies such as smartphones and wearable devices has increased significantly.2)
Compared to the time and monetary resources required for new drug development, DTx entails shorter periods and lower costs. DTx can also provide efficient healthcare services without the need for patient waiting times.3)4) Currently, DTx are mostly developed to treat mental health, but the treatment areas are expanding to include chronic diseases such as hypertension and diabetes. The prevalence of chronic diseases is continuously increasing, causing the social burden of chronic diseases to also increase significantly.5) Chronic diseases are closely related to lifestyle such as physical activity, smoking, and eating habits. Thus, maintaining a healthy lifestyle is very important in managing chronic diseases.6) As DTx can help manage chronic diseases by modifying lifestyle changes, it is expected that the use of DTx can reduce the socio-economic burden of chronic diseases. Thus, DTx is expected to meet new medical demands and create value in terms of the economy, and many countries are preparing policies to support DTx. In fact, FDA has recently eased its regulations on digital technologies to improve access to medical services under the constraints of COVID-19.7) Germany has also laid legislative groundwork for expanded digital technology usage, including the declaration of the Digital Healthcare Act (Digital-Versorgung-Geetz) in 2019.8)
Korea is also supporting the digital health market through the “Korean version of the Digital New Deal” policy, the regulatory innovation policy for medical devices, and Research and Development investment by government agencies. Regarding DTx, the Korean Ministry of Food and Drug Safety (MFDS) has published the Guideline on Review and Approval of DTx, thus making efforts to support the use of DTx.9) However there are currently no devices approved by the MFDS. Moreover, there is no standard in Korea after the approval stage of MFDS. The National Health Insurance (NHI) system accounts for a large amount of the total health finance, whether the health insurance system will cover DTx is a very important issue.
Based on the above, this study examined the concepts and characteristics of DTx and reviewed major countries' reimbursement policies for DTx, thus clarifying the political implications for introducing DTx in Korea.
CONCEPT OF DIGITAL THERAPEUTICS
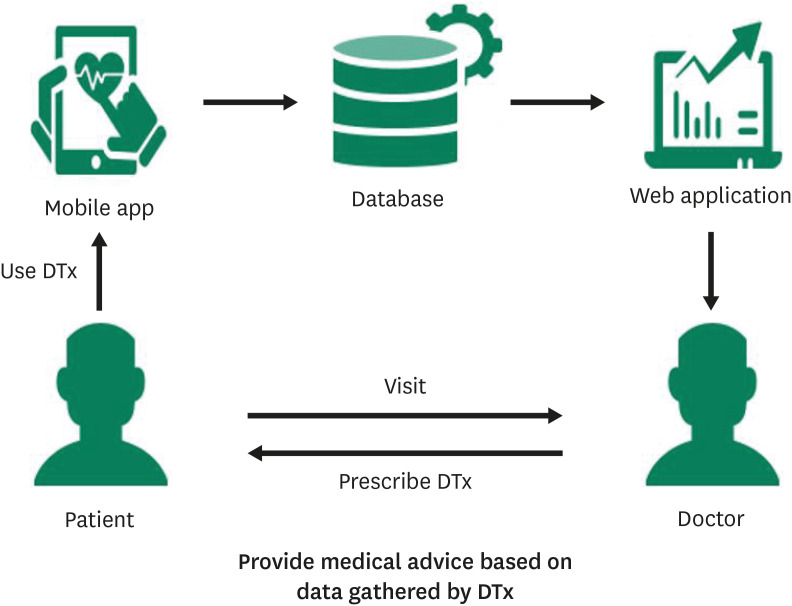
According to the Digital Therapeutics Alliance (DTA), DTx is defined as high-quality software that provides evidence-based therapeutic interventions designed to prevent, manage, and treat medical disabilities and diseases.10) The use of DTx also requires demonstrable clinically therapeutic effects and approval from specific regulatory authorities (e.g., when drugs are prescribed).10) In addition, DTx may be provided by various types of technologies such as mobile applications, virtual reality, and games. In the case of DTx in the form of mobile application, it may be used as shown in Figure 1. Doctors establish treatment plans using DTx according to the patient's condition. When doctors prescribe DTx, patients download the DTx and activate it using an access code to conduct treatment in their homes. Because DTx usage data is stored in a database, doctors can provide medical advice based on data gathered by DTx and it might be reflected in the treatment at the next visit.11)12)
DTx provides non-invasive treatment, thus they are mainly used in the treatment of neurological or mental health problems such as panic disorder or depression. Furthermore, DTx can be used to prevent deterioration of disease by providing lifestyle guidance for chronic disease patients. For example, high blood pressure is generally related to lifestyle habits such as excessive sodium intake, obesity, smoking, and drinking.5)13)14) Therefore, the optimal blood pressure can be achieved through lifestyle modification, but this depends on patients’ sustained self-management.5) An app that measures and monitors body weight and provides customized fitness or training plans for patients with high blood pressure leads to lifestyle changes and provides secondary precautions for patients with cardiovascular disease.15)
REGULATORY FRAMEWORK OF DIGITAL THERAPEUTICS
In Korea, the MFDS Guideline on Review and Approval of DTx establishes DTx as software as a medical device that provides evidence-based therapeutic interventions designed to prevent, manage, and treat medical disorders and diseases.9) Meanwhile, the Medical Device Act defines DTx as a form of medical device. The MFDS guidelines outline the scope of DTx based on both the International Classification of Diseases (ICD) and Korean Standard Classification of Diseases (KCD), and it is considered a program that is installed for use with general hardware (e.g., PCs and mobile devices). In addition, some DTx requires a prescription from a medical doctor, just as in the case of drugs or medical devices.9)
The US Policy for Device/Software Functions and Mobile Medical Applications defines DTx as a form of software application (mobile medical application) that is used to diagnose, treat, alleviate, and/or prevent diseases or other issues affecting the human body. According to the Federal Food, Drug, and Cosmetic Act, standards equivalent to the existing medical devices are applied with the classification in the range of class I–III, with most DTx applications considered class II medical devices. In the US, DTx can be used by patients or healthcare provider.16)
In the UK, there are comprehensive regulations on digital health products. In this case, there is no separate definition for DTx, as all such products are regulated as medical devices.17) However, the Improving Access to Psychological Therapies (IAPT) program defines DTx as a digitally enabled therapy provided through the internet under the guidance of clinicians and which is utilized as a secondary tool to aid treatments provided by healthcare professionals.18)19)
Germany declared the Digital Healthcare Act in 2019 to define DTx. Therein, DTx is described as a low-risk medical device (class I or IIa) that diagnoses, monitors, treats, and/or alleviates diseases or supports these functions. Prior to implementation, any DTx application must first be listed on Germany’s digital health app. Patients are also required to receive a DTx prescription from their doctor or therapist or prove their corresponding indication.15)
In Japan, DTx is defined as a software program that contributes to the diagnosis, treatment, and prevention of diseases according to the software as a medical device guideline of the Ministry of Health, Labor and Welfare. Any such application is regulated as a medical device (class I–IV). Most of the DTx can either be used by healthcare professionals or directly by patients that are supervised by healthcare professionals.20)
In Australia, DTx is defined as software that diagnoses, prevents, monitors, treats, and/or alleviates disease/injury or which controls and/or monitors anatomical or physiological functions of the body in accordance with the Therapeutic Goods Act and Software as a Medical Device Guidelines of the Therapeutic Goods Administration. Any such application is regulated as a medical device (class I–III). In Australia, DTx does not necessarily require implementation by a healthcare professional, but the class designation is lowered one level thereupon.21)22)
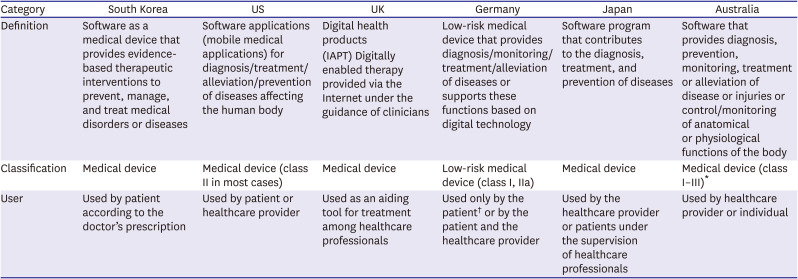
Table 1 shows a list comparing these elements by country.
Table 1
Regulatory framework of digital therapeutics
FINANCIAL SUPPORT POLICIES FOR DIGITAL THERAPEUTICS
In Korea, DTx can be supported through the systems of Innovative Health Technology and Conditionally Approved Health Technology, both of which are operated by the National Evidence-based Healthcare Collaborating Agency (NECA). Innovative Health technology is that which has received safety approval but is considered to have insufficient efficacy as determined by the New Health Technology Assessment. Such technologies can be selected when a “statement on the potential of health technology” is additionally submitted for application via the New Health Technology Assessment. Innovative Health Technologies are assigned preliminary classification codes so that temporary coverage of Korean NHI can be applied for three to five years, with clinical effectiveness re-evaluated thereafter. Meanwhile, a Conditionally Approved Health Technology is determined as a Research Stage Technology through the New Health Technology Assessment. In such cases, there are no problems in terms of safety. Further, the technology in question is deemed a priority in terms of the need for clinical implementation. For such types, government subsidies are provided for a set period based on a designation issued by the Minister of Health and Welfare.23)
In the US, a representative policy for DTx support is the Medicare Coverage of Innovative Technology (MCIT) program developed by Centers for Medicare and Medicaid Services (CMS).24)25) The MCIT program supports the market application of Breakthrough Devices; among products designated as such, the program is specifically intended for those that have obtained FDA Premarket Approval, including DTx. Manufacturers can apply for the MCIT program within two years following FDA approval (including authorization). Devices that are eligible for the program are allowed nationwide coverage for four years at the commercial level. After this, MCIT devices are assessed for National Coverage Determination (NCD), Local Coverage Determination (LCD), and claim-by-claim adjudication, according to the existing coverage determination procedure. Manufacturers wishing for NCD must submit data for coverage applications in the third year of the MCIT program. If a manufacturer does not wish to apply for NCD, LCD, or claim-by-claim adjudication, then their situation is assessed by the Medicare Administrative Contractor, which has been given the authority to establish LCD.25) However, the MCIT policy, which is slated for implementation in December 2021 was repealed in November 2021 for reasons such as evidence development or patient safety and CMS plans to develop another coverage policy to support DTx.26)
In the UK, the representative DTx support policy includes the NHS England Test Beds Programme, which handles clinical trials and collects real-world test data (Real-World-Testing) for digital health products, and the MedTech Funding Mandate policy (MTFM), which aims to reduce the financial burdens of new technologies, especially by assessing whether products that have acquired National Institute for Health and Care Excellence (NICE) approval reduce costs.27)28) In the case of the Test Beds Programme, funds are jointly raised by the Department of Health and Social Care, Office for Life Sciences, NHS England, and NHS Improvement; different levels of financial support may be provided depending on the size of the participating company.27) In the MTFM, the lowest price among the actual product cost, nominated supply cost, reference price set by NHS England and NHS improvement is used to set the product price. The NHS Commissioners provide funding support for a four-year period by paying the cost for the healthcare service provider that is purchasing the applicable product from the manufacturer.28)29)
Germany provides financial support for the development of DTx through the Innovation Fund (Innovationsfonds), which is funded by German Health Insurance (Gestzlicher Krankenversicherung, GKV). The Innovation Fund aims to both improve the supply of medical services and provide new medical services. Meanwhile, the Innovation Committee operates under Gemeinsame Bundesausschuss, and specifies the areas and standards of application, thus determining the recipients of support and paying accordingly. The Innovation Fund can support up to 100% of the total development costs, but funding is provided only when support is necessary.8)30)
Japan announced Digital Transformation action strategies in healthcare for SaMD called “DASH for SaMD” to support the establishment of a foundation for DTx development in 2020. While there is support for unifying channels, specific financial support programs have not been described to date.31)
In Australia, the National Digital Health Strategy indicates that the use of mobile apps can improve patient access to medical information, enhance quality, and ensure efficient healthcare services. Accordingly, Australia tests the clinical or economic effects of DTx through various pilot programs.32) For example, according to the University of Canberra's pilot program “Mobile health: Empowering people with type 2 diabetes using digital tools” most patients' diabetes status improved during the program, and the diabetes management app was found to be cost-effective.33) However, there are no clear financial support programs for DTx mentioned at the government level. Table 2 shows the financial support policies for DTx by country.
Table 2
Financial support policies for digital therapeutics by country
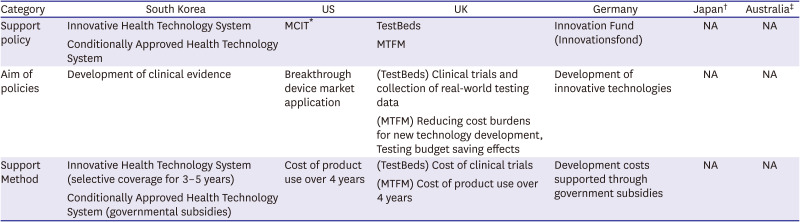
MCIT = Medicare Coverage of Innovative Technology; MTFM = MedTech Funding Mandate Policy; NA = not applicable.
*MCIT was repealed in November 2021; †Japan supports approval process of digital therapeutics through ‘DASH for SaMD’. However, a clear financial support policy has not been mentioned yet; ‡Various pilot programs are implemented as part of Australia’s digital strategy, but clear financial support policies at the government level have not been mentioned.
STANDARDS AND PROCEDURES FOR DIGITAL THERAPEUTICS COVERAGE DETERMINATIONS
In Korea, there are no dedicated standards and procedures for coverage determination as related to DTx. In the same manner of application for existing medical devices, the coverage status for approved DTx is determined through the New Health Technology Assessment conducted by NECA, assessed by the Health Insurance Review and Assessment Service (HIRA), and reviewed by the Health Insurance Policy Committee. Final coverage status is determined by notice of the Ministry of Health and Welfare. Clinical safety and effectiveness are also evaluated in the New Health Technology Assessment; however, usability testing is not currently considered. Coverage determination is done in the same manner that applies to existing medical devices, in which coverage is determined when both adequacy of coverage and economic efficiency have been demonstrated. In Korea, there have been no cases in which a DTx application has received MFDS approval and a health insurance coverage determination (Figure 2).23)34)35)
Figure 2
Health insurance coverage determination process for DTx by country.
DTx = digital therapeutics; IAPT = improving access to psychological therapies; PICO = Population, Intervention, Comparator and Outcome.
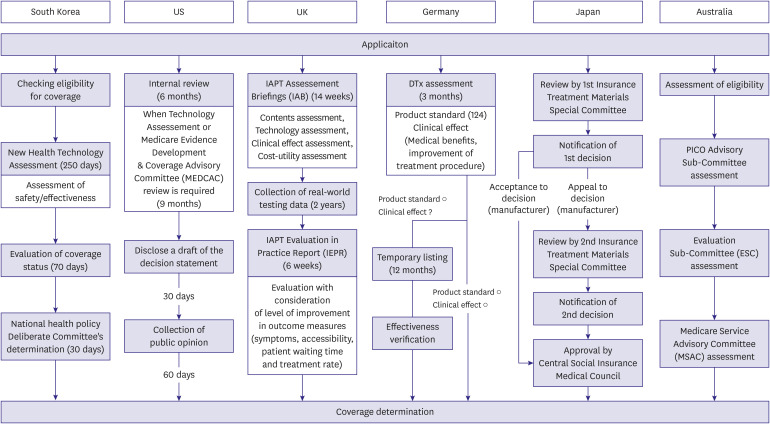
In the US, applications for Medicare coverage are assessed by CMS after FDA approval. There are no separate standards or procedures for coverage determinations pertaining to DTx; rather, existing NCD standards and procedures apply. In the case of NCD, coverage is determined when it is deemed both reasonable and necessary; the following criteria are used for healthcare services: 1) must be safe and effective; 2) should not be experimental or investigational; and 3) adequacy should be satisfied (duration, frequency of use, compliance with standard medical practice, provision of the service in an appropriate environment, provision of the service by qualified healthcare professionals, status of oversupply, demonstration of equivalent or superior effects when compared to existing technology). Any price is set during closed negotiations that consider the market value, development cost, and production cost. The NCD process takes approximately nine to twelve months, ranging from application to coverage determination (Figure 2).25)36) While DTx applications have received FDA approval, none have been granted coverage by CMS.37)
In the UK, approval must first be received from the Medicines and Healthcare Products Regulatory Agency (MHRA). Coverage is then determined by NHS England upon evaluation by the NICE.38) To date, the IAPT program has been tasked with granting DTx coverage. This entails a 14-week product review period, followed by a 2-year period in which real-world test data are collected; thereafter, coverage is determined upon the completion of a final six-week period of empirical testing, given its success.17)39)40) Product reviews require assessments for contents, clinical effects, and cost-utility, with the results (Improving Access to Psychological Therapies Assessment Briefings) used a basis for proceeding to the components involving the collection of real-world data and empirical testing (Figure 2).39) Based on the results of the real-world data collection process and evaluation, the Improving Access to Psychological Therapies Evaluation in Practice Report is published to cover factors such as symptoms, accessibility, patient waiting times, treatment rates, and the level of patient satisfaction. Coverage is granted if the DTx is deemed to have an effect equivalent or superior effect when compared to the relevant existing technology and is cost-effective or shows superior clinical effects.40) In the case of IAPT program, price is determined based on the outcomes of the collected data. To date, only one DTx application has been granted coverage through the IAPT program. Such coverage is permitted when it is still possible to monitor patients who want to discontinue their treatments, when there is sufficient communication between healthcare professionals and the patients, and when a clear plan of support is established by the healthcare professionals.41)
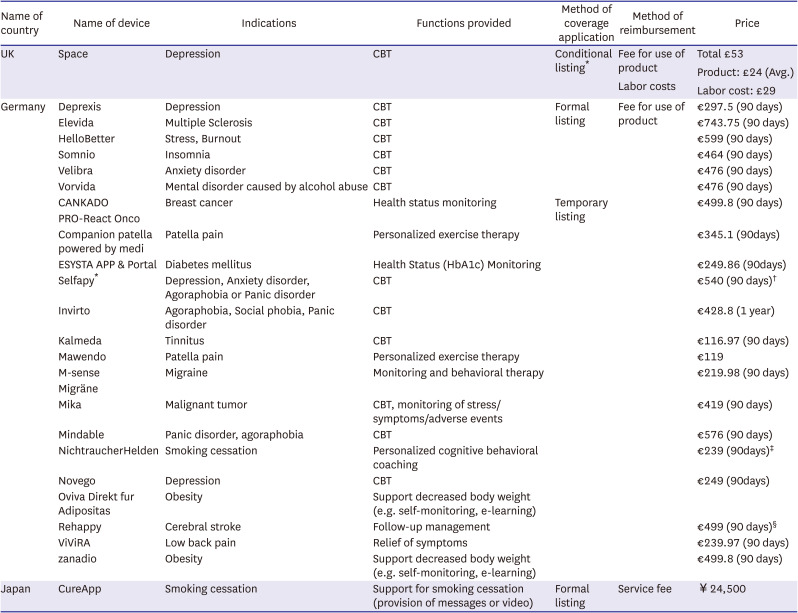
In Germany, DTx coverage is determined through a three-month evaluation conducted by the Federal Institute of Medicines and Medical Devices (Bundesinstitut für Arzneimittel und Medizinprodukte), which operates under the Digital Healthcare Act. DTx coverage is divided into temporary and formal listings.15) It is possible to achieve a formal listing upon demonstrating positive healthcare effects and meeting 124 device requirements (e.g., safety and suitability for use, data protection, information security, interoperability, device robustness, consumer protection, usability, support for healthcare provider, healthcare content quality, patients safety).15) A temporary listing may be granted for a duration of one year when only the device requirements are satisfied, but a formal listing can only be obtained in such cases if positive healthcare effects are verified during the same period (Figure 2).15) DTx pricing is set using a similar method that applies to medicines. Here, DTx prices are annually determined through closed negotiations between the German health insurance agency (GKV-Spizenverband) and the respective DTx manufacturers. If a price negotiation fails, then the arbitration committee determines the price within a three-month period. GKV-Spizenverband and the DTx manufacturer in question then renegotiate the price one year from the date of this determination. For a temporary listing, the prices of medicines or products with similar effects to the DTx are used as references to set the maximum price. The cost submitted by the manufacturer is reimbursed for one year, then determined through closed negotiations.15) In Germany, DTx has been listed for use in various fields, including mental disease, tinnitus, stroke, cancer, and obesity. Currently, 18 DTx devices are on temporary listings, while six devices are on formal listings.42)
In Japan, approval must first be received by the Pharmaceuticals and Medical Devices Agency. This is conducted in the same manner that applies to the existing treatment materials. DTx coverage is then determined after evaluation by the Health Insurance Treatment Materials Special Committee under the Ministry of Health, Labour and Welfare of Japan as well as review and approval by the Central Social Insurance and Medical Council. Treatment materials are classified into group A (reimbursement is comprehensively included within the existing treatment reimbursement score), group B (separate reimbursement), group C (corresponding to New Health Technology), and group F (non-coverage). DTx applications are also classified into one of these groups at the time of application for coverage, which is granted based on an evaluation of similar functions, new functions, manufacturing costs, import costs, and cost effectiveness (Figure 2).43) There are two pricing methods. The first pertains to situations in which existing devices can be used as points of reference, followed by a moderation process to set the base price. In cases where there are no similar functions, the base price is set according to various relevant factors, including manufacturing, imports, sales, administrative issues, operations, distribution, consumption, and local consumption taxes. Once a base price has been established, the final price is determined after making adjustments, taking into consideration average prices overseas.44) Looking at currently listed DTx products, one supports smoking cessation treatment, with coverage determined as group C in terms of the treatment materials. The price was determined based on the service fees (i.e., fees for the management of nicotine dependence).45) Moreover, DTx for hypertension management will possibly be under discussion for health insurance coverage in 2022.46)
Australia has not established separate standards and procedures for making coverage determinations relevant to DTx. Rather, such determinations are made in the same manner used for existing medical devices where coverage is determined by the Department of Health when safety, effectiveness, and cost-utility have been demonstrated after a four-to-six-month evaluation conducted by the Medical Services Advisory Committee (Figure 2). Currently, there are no known cases in which coverage listings have been granted to DTx products.47)48) DTx coverage determination standards and DTx application cases by country are summarized in Tables 3 and 4, respectively.
Table 3
Digital therapeutics coverage determination standards by country
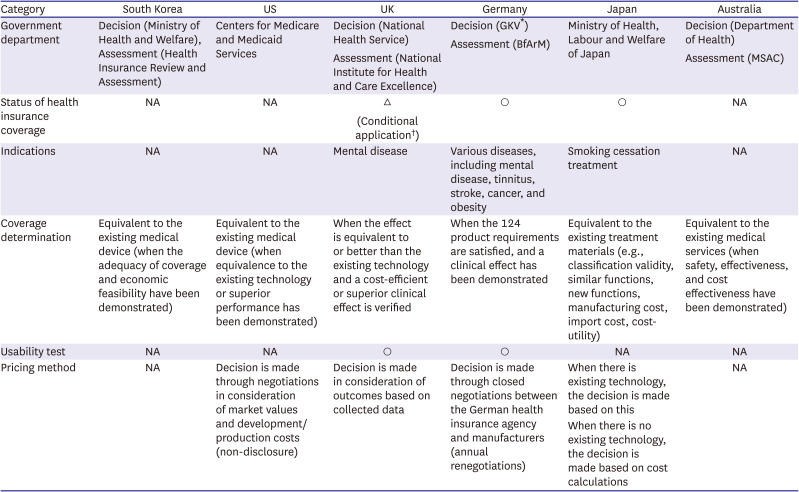
BfArM = Bundesinstitut für Arzneimittel und Medizinprodukte; MSAC = Medical Services Advisory Committee; NA = not applicable.
*GKV-Spizenverband; †Health insurance coverage is permitted when it is still possible to monitor the patient even after they have discontinued their treatment, there is still sufficient communication between healthcare professionals and the patient, and a clear support plan has been established by the healthcare professionals.
Table 4
Cases of digital therapeutics application by country
KEY LESSONS LEARNED
Most of the current health insurance listed cases are about mental health. However, like Germany and Japan, DTx in various areas, including hypertension or diabetes management can be developed and covered by national health insurance in the near future. Therefore, according to the Korean situation, it is necessary to prepare this in advance at the national level.
Regarding the concept of DTx, Korea uses a similar definition to those employed in the US, UK, Germany, Japan, and Australia. DTx is also regulated as a form of medical device in Korea. As for relevant financial support, two representative reimbursement methods are used outside Korea: 1) government subsidies or fundraising and 2) applications for health insurance coverage. Although details of support methods used in countries such as the US, UK, and Germany are different in various areas, each country operates a system in which the development or usage costs are supported to reduce the financial burdens related to DTx. In the US, financial support for DTx usage through MCIT was planned but unfortunately repealed in November 2021. In the UK and Germany, support is either provided at the cost level for a certain period or government subsidies and funds are garnered to support the development or usage costs. In Korea, the Innovative Health Technology system currently permits financial support for clinical trials and clinical use, but reimbursements are not fully processed due to the difficulty of setting standards. In addition, burdens may be imposed on the national health insurance budget. To fully implement DTx within the Innovative Health Technology system, Korean policymakers should refer to examples such as the MTFM used in the UK and the temporary listings system used in Germany, both of which provide support through reimbursements at cost levels for set periods. As in the case of the UK TestBeds program, in which support projects are run by multi-ministerial budgets, or the Innovation Fund in Germany, support for DTx can also be provided by government subsidies or fundraising.
In countries outside Korea, DTx coverage determination standards and procedures are applied based on existing medical devices or medical procedures. Coverage is considered when DTx applications are demonstrably equivalent to or better than their existing technological counterparts. For reimbursements, coverage is applied in the same manner used for drugs or medical devices in the UK and Germany, however it is applied according to medical procedures in Japan. Meanwhile, pricing is determined through closed negotiations or depending on the presence of an existing technology; medical benefits or cost information that can be applied are also referred to when estimating price. Rather than establishing separate standards for introducing DTx into the national health insurance system in Korea, it would be more reasonable to determine health insurance coverage according to existing standards and procedures. However, in terms of reimbursements for medical devices in Korea, payments are usually made by including the healthcare service fees. Considering that DTx is treated similarly to drugs (e.g., usage requires a prescription), the remaining challenges are establishing pricing and determining the details of reimbursement. In this regard, policymakers should apply the existing standards used to reimburse the costs of drugs and treatment materials. When DTx is used as a tool to aid in the application of medical services provided by doctors, it may be best to implement a combined reimbursement method that includes service fees and costs of treatment materials.
In the UK, usability assessments are considered when making DTx coverage determinations. Apart from the clinical effects, real-world testing is highly important, but usability assessments are not currently considered in the process used by the New Health Technology Assessment in Korea. This highlights the need to improve the current system by establishing an additional procedure for testing and verifying the actual effects of DTx under the New Health Technology or Innovative Health Technology systems. However, it is also necessary to adjust the assessment period in consideration of the rapid pace at which software changes are often implemented. While countries such as the UK and Germany apply a one- or two-year period, the New Health Technology Assessment and Innovative Health Technology systems in Korea apply a much longer period of three to five years. In this regard, the prompt adoption of DTx requires a shorter the assessment period; this process demands clear specifications and selection criteria to prevent indiscriminate approval and entry.
CONCLUSION
In countries outside Korea, DTx is financially supported through two representative methods, including 1) government subsidies, or fundraising and 2) the application of health insurance coverage. Currently, costs are a major problem in the utilization of digital health technologies, which highlights the need for a financial support system aimed at the provision of non-contact healthcare in Korea. However, the overall budget impacts must be considered when applying health insurance coverage for DTx. The future direction for relevant support in Korea should include 1) cost-level reimbursements for a set period for Innovative Health Technology and 2) financial support through government subsidies or fundraising. From a long-term perspective, the application of health insurance coverage for DTx requires a reimbursement system that considers the value of DTx rather than the cost. This entails a condition in which validation is achieved through real-world testing. In this regard, either a council should be organized to lead the coverage determination process, or a dedicated assessment committee should be established.
 XML Download
XML Download