

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pituitary tumors are second frequently diagnosed primary CNS tumors in both Korea and the Unites States1523). The conventional classifications are based on the size and functional status of tumors. Furthermore, several other classifications of suprasellar extension and parasellar extension of pituitary adenomas have been proposed1218). Parasellar extension is measured based on the preoperative MR image and reflects the cavernous sinus (CS) invasion status of the pituitary adenoma18).
Regarding the extent of resection for pituitary adenomas by endoscopic endonasal transsphenoidal surgery (EETS), good predictive factors include preoperative tumor size, volume, parasellar extension grade, and the skill of the operating surgeon51626). Among these factors, the highest predictive value has been reported for parasellar extension grades516).
In their revision of the Knosp's parasellar extension grading system (Fig. 1), Micko et al.21) divided Grade 3 of the previous classification into Grades 3A and 3B based on the involvement of the CS compartment. Grade 3A adenomas extend into the superior CS compartment, while Grade 3B adenomas extend into the inferior CS compartment. Micko et al. demonstrated that, with higher parasellar extension grades, the rates of the CS invasion increase and the possibility of gross total removal (GTR) and endocrinologic remission decrease. The additional division of Grade 3 results in significantly different outcomes of pituitary adenomas in Grades 3A and 3B.
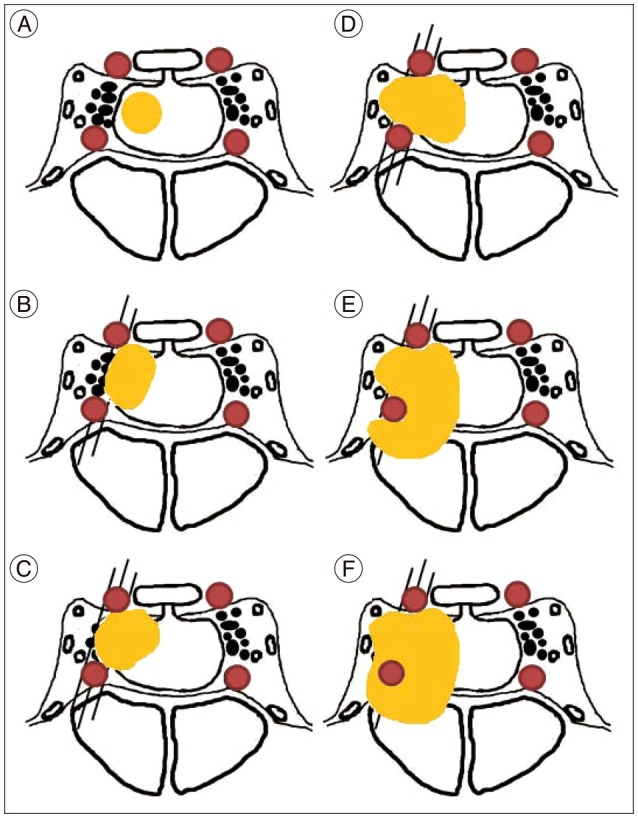 | Fig. 1According to the article of Micko et al.21), SHL redraws illustration of the modified Knosp's classification. A : Grade 0 : the adenoma does not encroach on the CS space. Thus, the tangent of the medial aspects of the intracavernous and supracavernous ICAs is not passed. B : Grade 1 : the medial tangent is passed, but the extension does not go beyond a line drawn between the cross-sectional centers of the intracavernous and supracavernous ICAs (the intercarotid line). C : Grade 2 : the tumor extends beyond the intercarotid line, but does not pass the tangent on the lateral aspects of the intracavernous and supracavernous ICAs. D : Grade 3A : the tumor extends lateral to the lateral tangent of the intracavernous and supracavernous ICAs into the superior CS compartment. E : Grade 3B : the tumor extends lateral to the lateral tangent of the intracavernous and supracavernous ICAs into the inferior CS compartment. F : Grade 4 : there is total encasement of the intracavernous carotid artery. CS : cavernous sinus, ICA : internal carotid artery.
|
However, when applying the Knosp's parasellar extension grading system, the lateral extent of the tumor extension showed ambiguous findings in several cases. In addition to the comparison of the gadolinium-enhanced T1 coronal images, routine comparison of T2 coronal images is mandatory (Fig. 2). Due to a more complex criterion, further subdivision of the grades can intensify this ambiguousness. Therefore, the inter-rater reliability of the grading system was assessed to show the agreement across different raters. The clinical validity was evaluated by analyzing the extent of resection and complications rates of each grade.
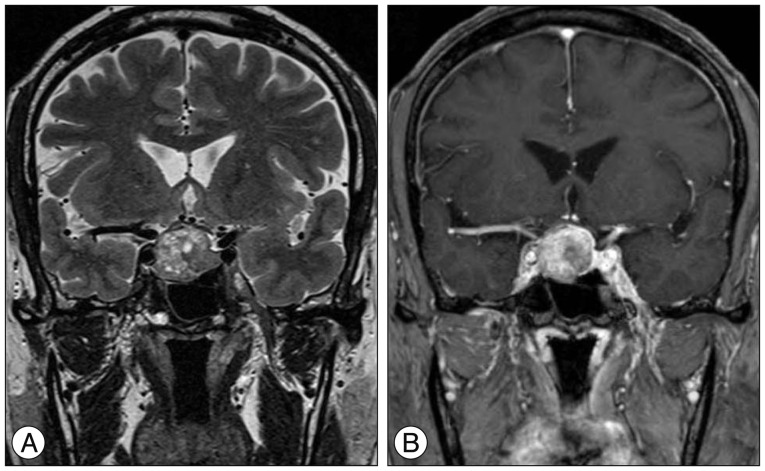 | Fig. 2An illustrative case emphasizing routine inspection of the T2 weighted image, as well as the gadolinium-enhanced T1 image on a preoperative magnetic resonance image scan. A : T2 weighted image. Cavernous ICA does not seem to be encased by the pituitary mass. In grading, two raters confirmed these cases as Grades 1 and 2, respectively. B : T1 weighted image with gadolinium enhancement. Right cavernous ICA seems to be encased by the pituitary mass. One rater confirmed this case as Grade 4. ICA : internal carotid artery.
|
Go to : 
MATERIALS AND METHODS
Patient characteristics
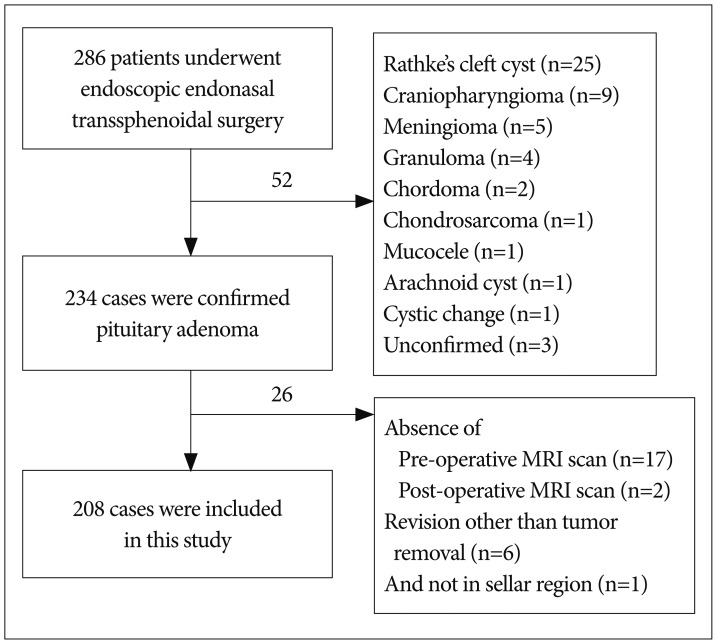
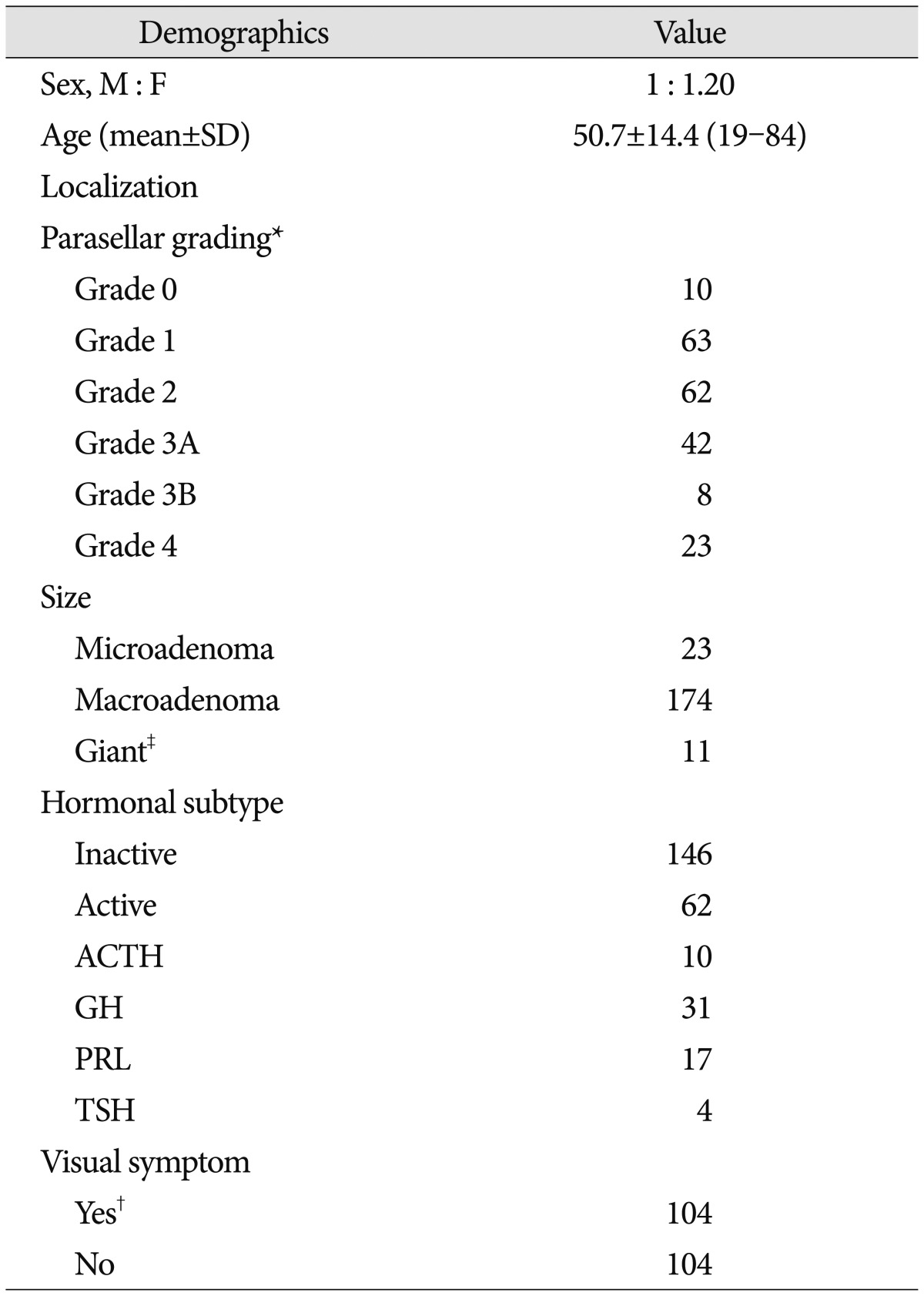
From November 2008 to August 2015, 286 EETSs were performed with the binostril approach by the senior author (YKH) in Seoul St. Mary's Hospital, the Catholic University of Korea. Of those, only pathologically confirmed pituitary adenoma cases were included in this study, regardless of the size and hormonal function of adenomas; the total number of cases amounted to 234. The cases without proper pre- and post-operative image for analysis, revision surgeries not for tumor removal, and pathologies other than those in the sellar area were excluded from the dataset (Fig. 3). The summary of the demographic data is provided in Table 1.
Data acquisition
This study was approved by the Institutional Review Board of Seoul St. Mary's Hospital. Baseline characteristics of the patients and tumors were acquired in the retrospective manner by reviewing the medical records; then, the characteristics were categorized according to their parasellar extension grades in the preoperative MR images. By including single surgeon's data, we sought to minimize the bias from different surgical skills of endoscopic operators.
The grading was performed by two neurosurgeons and one neuroradiologist using the coronal section of preoperative T2 and gadolinium-enhanced T1 images by the modified Knosp's grading system21). The grading results of the raters were blinded to each other during the procedure. The extent of resection rate was evaluated by the neuroradiologist's comparison of the pre- and postoperative MR images and review of the operation records. GTR was rated in cases when there was no remaining tumor in the postoperative MR image. Subtotal tumor removal (STR), partial tumor removal (PR), and biopsy were rated when >90%, 50–90%, and <50% of the tumor volume was removed in the postoperative MR image.
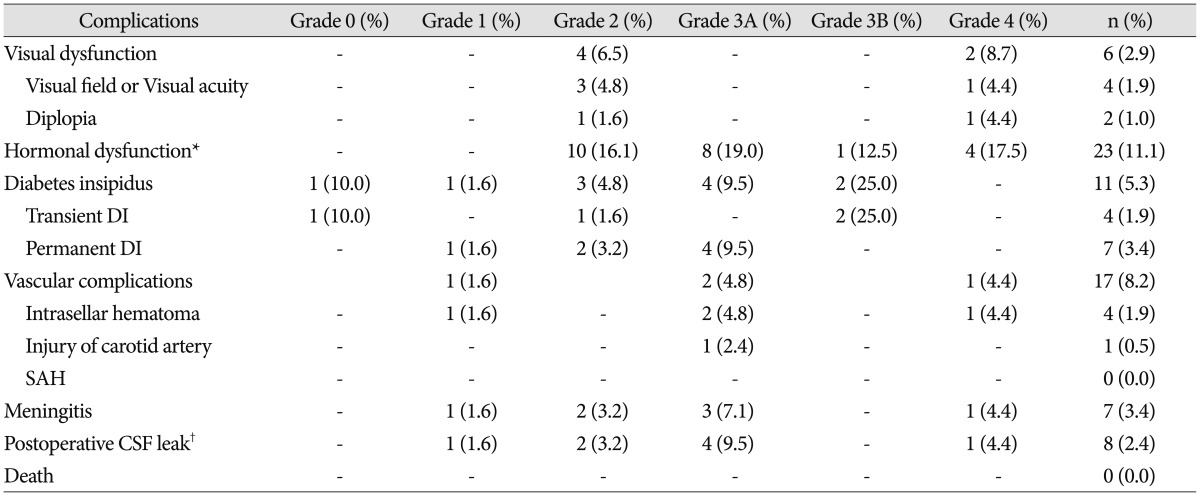
Furthermore, we collected additional data about neurovascular and endocrinologic complications and evaluated the relationship between the parasellar extension and surgical complication rates. These complications included visual and endocrine dysfunctions, vascular complication, cerebrospinal fluid (CSF) leakage, and meningitis (Table 2). A condition was considered as 'serious' in cases when the patient 1) had to receive prolonged hospitalization with or without further invasive procedures or medication; 2) had remaining neurologic deficit even after a long-term follow-up done at least six months after discharge; or 3) had endocrinologic dysfunction that required supplementary medication.
Surgical technique
The surgical technique was identical to the method described in a recent publication of the author group24). All operations were performed via the binostrils-four hands technique. In this technique, the main surgeon uses two hands to use surgical instruments, while an assistant neurosurgeon uses two hands to hold the endoscope. A rhinology surgeon performed surgery in the nasal and sphenoid stage, neurosurgeon performed surgery in the sellar stage; sellar repair was performed by both surgeons.
The patient's head was placed on a horseshoe-shaped headrest and an electromagnetic frameless navigation system (Medtronics®, Louisville, KY, USA) was used. On taking proper measures to the superior, middle, and inferior turbinates on both sides for visualization, the natural orifice of the sphenoid sinus was identified. Bilateral modified "rescue" flaps introduced by Kim et al.17) were used. We attempted to harvest the posterior septal bone in an en-bloc fashion to further use in the sellar floor reconstruction. The sellar floor was revealed after the procedure and a modified "rescue" flap was made along the removed septal bone.
The sellar floor was drilled out until the blue-colored dura, supposedly CS, was observed. After coagulation of the dura, it was opened using a de DIVITIIS-CAPPABIANCA Scalpel (Karl Storz®, Mittelstrasse, Tuttlingen, Germany). The initial dural incision was made horizontally on the lower part of the dura with perpendicular excisions superiorly most of the times (for further detail, see Dusick et al.)9). Doppler sonography, DVM-4300 Doppler Volume Flowmeter (Hadeco®, Kawasaki, Japan), was used to identify the exact location of the cavernous internal carotid artery (ICA) and care was taken not to injure. In cases with suspected CS invasion, the bony opening and the dural opening needed to be sufficiently lateral, without making injuries to the cavernous ICA.
After the dural opening, the tumor was removed using the binostrils-four hands technique performed by two neurosurgeons using various endoscopic instruments (Karl Storz®, Mittelstrasse, Tuttlingen, Germany). Whenever possible, en-bloc tumor removal was performed. When the tumor was removed in the piecemeal fashion, the mass was removed from the inferior to the superior direction in order to prevent blocking of the view by bulging of the diaphragm sellae. Finally, the mass suspected for the CS invasion was removed to avoid hindering the operative view from sinus bleeding after tumor removal.
If the CSF leakage occurred after tumor removal, the sellar floor was reconstructed using the previously reported modified CSF leakage repair technique17).
Data analysis
Inter-rater reliability was statistically assessed by measuring intraclass correlation coefficient (ICC) from a two-way ANOVA. The reliability was ranked as excellent, good, moderate, and poor for ICC>0.75, 0.60–0.75, 0.40–0.59, and <0.40, respectively11).
The GTR rates were measured in each parasellar extension grade and their statistical differences were calculated. Pearson's χ2 test (Fisher's exact test) was performed; p-values <0.05 were considered to be statistically significant. Bonferroni correction was applied 5 times to calculate significant differences between adjacent grades (G0/G1, G1/G2, G2/G3A, G3A/G3B, and G3B/G4). In post-hoc test, p<0.01 (0.05/5) was considered to be statistically significant.
The relationships among 'serious' complication rates regarding parasellar extension and extents of resection were also analyzed using a logistic regression test.
All statistical analyses were performed using the SPSS 18.0 software (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
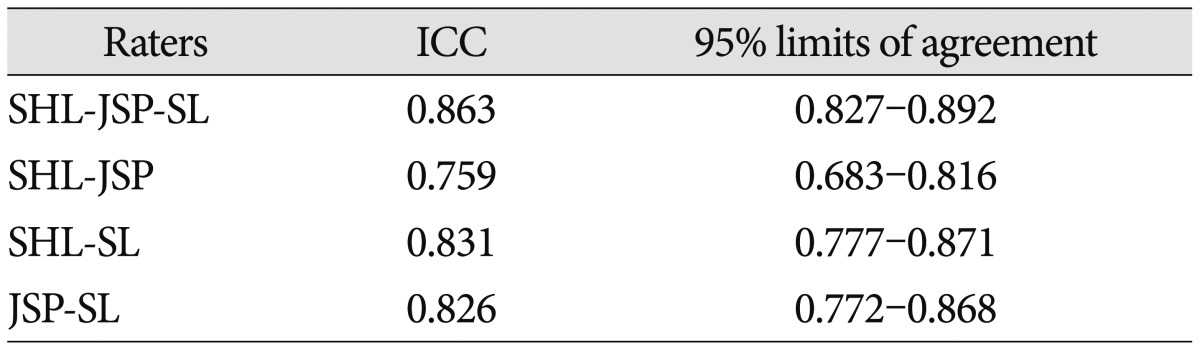
Comparing the grading performed by three different raters (SHL, JSP, and SL), the reliability value of ICC amounted to 0.863, suggesting an excellent agreement across the raters. The inter-rater reliability values between two raters were also calculated using the Kohen's kappa method; the obtained value amounted to 0.759 between SHL and JSP, 0.831 between SHL and SL, and 0.826 between JSP and SL; therefore, all values suggested excellent agreement (Table 3).
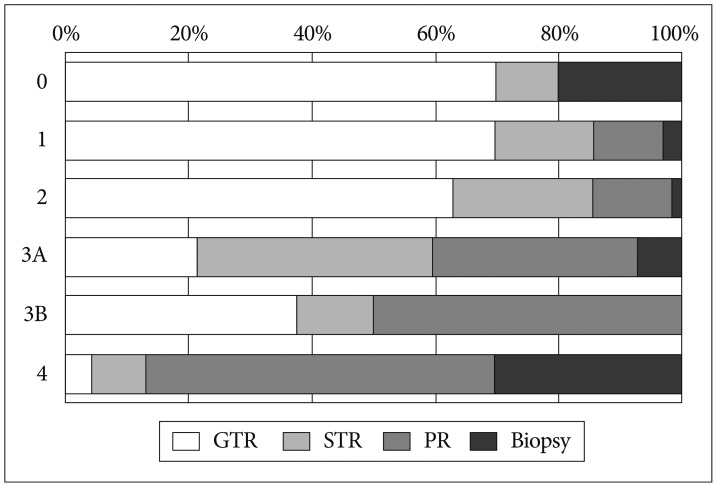
The distribution between the grades was 4.8, 30.3, 29.8, 20.2, 3.8, and 11.1% for Grades 0, 1, 2, 3A, 3B, and 4, respectively. The GTR rates achieved in each grade were 70.0, 69.8, 62.9, 21.4, 37.5, and 4.3% for Grades 0, 1, 2, 3A, 3B, and 4, respectively. The extent of resection according to the parasellar extension grade is shown in Fig. 4. The specific numeric data are presented in Table 4. This table shows inverse proportional relationships between parasellar extension grades and the rates of GTR.
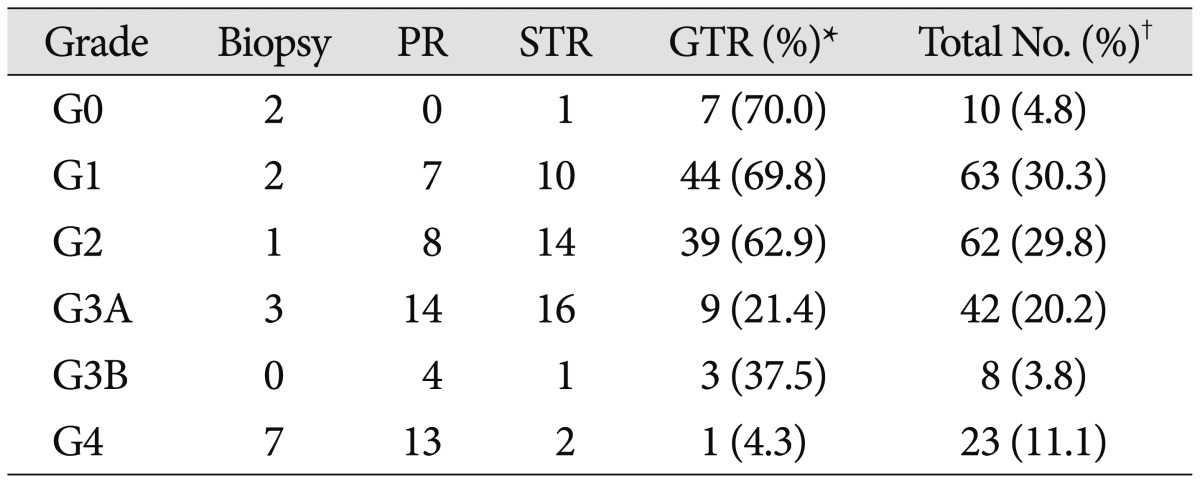
In post-hoc test between adjacent grades regarding the GTR rates, Grade 2 adenomas had a significantly higher GTR rate as compared to Grade 3A adenomas (p<0.001). No statistically significant differences of GTR rate were observed across other grades; p-values were 0.992, 0.412, 0.329 and 0.016 for G0/1, G1/2, G3A/3B, and G3B/4, respectively. In this post-hoc test, p<0.01 was considered to be statistically significant.
Regarding 'serious' complications rates, significantly higher rates of complications were revealed in the groups above Grade 3A [odds ratio (OR)=2.862, p=0.007, 95% confidence interval 1.325–6.185]. No significant differences of complication rates among the extents of resection subgroups were observed (OR= 1.146, p=0.730, 95% confidence interval 0.529–2.483).
Go to :
DISCUSSION
To predict the CS invasion, we used the parasellar extension grading system suggested by Micko et al.21). The newly proposed grading system is valuable in that it further categorizes the extent of the CS invasion. The preoperative grading was applied to help make surgical plans, whether or not to remove the tumor with CS invasion. However, when applied in clinical settings, the distinction between each grade remains relatively unclear in many cases. Several aspects, including technical, tumor, and interpreter factors, underpin the reasons for this discrepancy. Technical factors include the available type of preoperative image, the quality of the image, and the slice gained for coronal imaging. The tumor factors refer to the shape of the tumor, thickening of the tumor capsule, the tortuosity of cavernous ICA, and the type of the previous treatment received. The interpreter factors include the interpreter's experience and interpretation of the exact tumor extent.
Due to the complexity of the aforementioned grading system, the parasellar extension grade between different raters has, in some cases, remained inconsistent. In order to statistically evaluate the reliability of this grading system, we assessed the inter-rater reliability across different raters, which, to the best of our knowledge, has never been done in previous literature. In evaluating reliability, test-retest reliability and inter-rater reliability are both commonly used2625). The reason underpinning our decision to evaluate only the inter-rater reliability is that, in clinical settings, such as measuring the parasellar extension grades, retesting is not necessary in most cases. Since the parasellar extension by Knosp's classification is based on preoperative images, the image findings are unlikely to change over time. Rather, they are used only for communication before surgery to predict the extent of resection. For that reason, many previous studies checked only inter-rater reliability for assessing reliability of a diagnostic tool320).
In the present study, inter-rater reliability was assessed by calculating ICC by two-way ANOVA. The reliability value amounted to 0.863, suggesting an excellent agreement across the raters. This finding highlights that the modified Knosp's classification, however complex it might appear, can be reliably used as a new standard of evaluating parasellar extension, replacing thus the previous version of the classification system. Therefore, we would like to encourage the usage of this classification by other institutes and further comparisons the new findings with those reported in the present study.
Next, we attempted to verify the clinical validity of the grading system by assessing the extents of resection and complication rates among parasellar extension grades. Regarding the GTR rate among the grades, a statistically significant difference was observed only between Grades 2 and 3A. While the grading system by Micko et al. showed lower GTR rates as the grade ascends, with a significant difference between Grade 3A and 3B, our results showed more decreased GTR rates on Grade 3A patients than Grade 3B patients. However, this finding was statistically insignificant, probably due to the diminished case number on each subgroup. Although our study population was relatively large, after dividing the studied cases into 6 parasellar extension grades, the proportion of each grade got smaller. If the study had been conducted on a larger scale, with a sufficient proportion of cases in each grade, more significant differences might have been observed between other subgroups as well.
However, the present study showed a significant difference between Grades 2 and 3A in the GTR rate. Additionally, we performed 2 more post-hoc tests between Grades 0 and 2, Grades 3A and 4 (p=0.665 and 0.068, respectively) to further analyze the statistically significant differences in non-adjacent grades. These findings suggest that, in cases with parasellar extension of the grades higher than 3A, the likeliness of GTR will significantly decrease. The CS invasion has already been reported to have a negative predictive value on the tumor removal rate, although most previous studies do not set distinct criteria for the parasellar extension grade affecting the tumor removal rate1,810). Hereby, we would like to propose the negative predictive value of Grades 3A, 3B, and 4 regarding the tumor removal rate.
According to the initial Knosp's classification, only Grades 3 and 4 premise that there is a genuine CS invasion18). Although Micko et al.21) reported some portion of the CS invasions with grades lower than Grade 3, our findings suggest that parasellar extension grades above Grade 3A have a clinically relevant CS invasion.
We also analyzed the complication rates among parasellar extension grades. In our results, the cases with Grades 3A, 3B, and 4 showed significantly higher complication rates as compared to other cases. Considering that, in higher grades, an attempted GTR can lead to further neurologic sequelae to the cranial nerves III, IV, and VI, we also analyzed the relationship between complication rates and extents of resection. No significant differences among extent of resection subgroups were observed. Therefore, we can safely assume that parasellar extension Grades 3A, 3B, and 4 are related to higher complication rates, regardless of the extents of resection.
In the present study, no microscopic or endoscopic verification of parasellar extension grading was performed. Owing to this procedure, the study could have obtained a more detailed description of the CS invasion among each of the studied parasellar extension grades. Due to the retrospective nature of the present study, this limitation could not have been overcome. Further prospective studies should be warranted to amend for this limitation.
Besides the presence of the CS invasion, the surgical goal and skills are also important to predict the extent of resection16). The surgical goals for functioning and non-functioning pituitary adenomas are slightly different in our institution. In cases of functioning pituitary adenoma, the surgical goal would be endocrinologic remission without considerable operative morbidity. When endocrinologic remission was not achieved, medical treatment, such as bromocriptine, cabergoline in prolactinoma, or somatostatin in the GH-producing pituitary adenoma, was applied to the patient427). On the other hand, in the cases of non-functioning pituitary adenomas, the surgical goal was symptom relief by decompression with a maximally safe resection without complications13). Due to this difference between the surgical goals in functioning and non-functioning pituitary adenoma surgery, the GTR rate should have been evaluated in the subgroup analysis. Considering the purpose of the present study and due to the sufficient number of the analyzed cases, we assumed that this negligence of analysis would not affect the results. The difference of the GTR rates between the two groups is one of the factors intended for inclusion in our future research.
In addition, the skills of the operating surgeon, novice or expert, are also important. The study population of our research was operated by an endoscopic surgeon in our institute with over several hundred cases of experience. Moreover, the complication rates in the present study can be considered to be equivalent to other international series19). The operations were performed in the fully endoscopic manner, which is now widely acknowledged as the most popular method for transsphenoidal surgery 71422).
Go to :
CONCLUSION
The modified Knosp's grading system shows a high inter-rater reliability with an excellent agreement across the raters. Preoperative parasellar extension grading is valuable in predicting the extents of resection and surgical complication rates in EETS for pituitary adenomas. Parasellar extension Grades 3A, 3B, and 4 have a negative predictive value for the GTR rate, with higher complication rates.
Go to :
 XML Download
XML Download