

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hemifacial spasm (HFS) is characterized by frequent involuntary twitching contractions of the unilateral facial muscle, and it is mainly caused by a neurovascular compression on the root exit zone (REZ) of the facial nerve by one or more adjacent arteries4930). As numerous authors have reported that the adequate separation of the compressing vessel from the REZ of the facial nerve is essential for long-term symptomatic relief, the microvascular decompression (MVD) surgery has been used as an effective and curative treatment modality25831).
The posterior inferior cerebellar artery (PICA) and anterior inferior cerebellar artery (AICA) are the two arteries most commonly involved in HFS. The vertebral artery (VA) is also known to cause compression, but instead of direct compression on the REZ, it tends to generate indirect transmission of pulses on the REZ via other arteries, such as PICA or AICA2111920). Unsatisfactory postoperative results have been reported in relation to the involvement of the VA21). Given its larger caliber, and hence greater elasticity, decompression of the VA can be technically challenging with traditional application of Teflon prostheses or other cushions5717). In addition to its naturally larger caliber, the VA or basilar artery (BA) can be associated with vertebrobasilar dolichoectasia (VBD) or atherosclerosis, which would cause greater difficulty for the surgeons22). As excessive amounts of Teflon sponges can be responsible for unnecessary pressure on the brainstem, a different approach is required for lesions involving the VA3637). Several surgical techniques have been introduced for such cases : repositioning procedure using a Teflon sling, anchoring with aneurysmal clips, a dural flap, synthetic vascular graft for transpositioning, the double-stick tape method, and among others13101323273341). Here, we present not only our application of a bioglue-coated Teflon sling on the VA during MVD but also the clinical outcomes, including recurrence rate and postoperative complications. To the best of our knowledge, this is the first report of this technique using a bioglue-coated Teflon sling along with clinical results in cases with a minimum follow-up period of 2 years.
Go to : 
MATERIALS AND METHODS
Patient selection and preoperative evaluation
A total of 234 patients with HFS underwent MVD between 2005 and 2015 at our institute. The VA was thought to account for HFS in 54 patients, to whom our novel technique was applied. Among them, 42 patients with follow-up periods of 2 years or longer were selected for the analysis. For the diagnosis of HFS, the characteristics of facial spasm were evaluated and past medical history was also carefully reviewed. Either a 1.5T magnetic resonance imaging (MRI) system (Signa EXCITE; GE Healthcare, Waukesha, WI, USA) or 3.0T MRI system (Achieva 3.0T TX; Philips Healthcare, Best, the Netherlands) or multi-detector computed tomography angiography (MDCTA) (Brilliance; Philips Healthcare, Best, the Netherlands) was utilized to detect compressing vessels or concomitant lesions near the REZ of the facial nerve. All patients underwent preoperative electromyogram motor nerve conduction velocity (EMG-MCV) examination of the facial nerve to obtain baseline data for comparison of the lateral spread response before and after the operation. Pure tone audiometry (Orbiter 922, Madsen Electronics, Minneapolis, MN, USA), speech audiometry (Orbital 922), and impedance audiometry (Madsen Otoflex 100, GN Otometrics, Taastrup, Denmark) were also carried out to identify any hearing impairments or tinnitus prior to surgery.
Surgical procedure
All patients underwent retromastoid craniotomy under general anesthesia. Additional craniectomy was carried out to allow more medial and ventral exposure of the course of the large vessel. The arachnoid membrane was carefully dissected to fully expose the large vessel responsible for HFS. The relationship between the large vessel and REZ of the facial nerve was visualized using an operative microscope (OPMI Pentero; Carl Zeiss, Oberkocken, Germany) and neuroendoscope (Karl Storz GmbH, Tuttlingen, Germany) if needed. Gentle mobilization on the VA was attempted for better visualization on its course, as well as the presence of concomitant compressing vessels, such as PICA or AICA. Perforating arteries to the brainstem were also thoroughly investigated and carefully protected.
A bioglue-coated Teflon sling was made by the surgeon. Several Teflon threads were prepared and manually twisted together with bioglue (Tisseel®; Baxter Healthcare Corp., Glendale, CA, USA) to make an elongated strand (Fig. 1). The coating procedure enabled the Teflon sling to be lint-free and smooth so it could be manipulated more easily by the surgeon, and it also increased the tensile force of the strand. The sling was approximately 1 mm in width and 5–7 cm in length. The width and length of the sling could be adjusted with the amount of Teflon and bioglue according to the surgical conditions. Using a microscope, the sling was carefully looped around the offending large vessel. The optimal direction of the retracted sling harboring the VA was determined by the surgeon and it was stitched onto the petrosal dura using 5-0 black silk suture. Each end of the sling was stitched to the dura separately (Fig. 2). The stitch was always located between the jugular foramen and acoustic canal as suggested in the literature27). Careful inspection was needed to avoid kinking or stretching of small perforating vessels before the stitch of the sling on the dura. Prior to the stitch, the bioglue was helpful for temporary adhesion of the sling on the dura. After adequate transposition of the large vessel with bioglue-coated Teflon sling, the space between the large vessel and REZ of the facial nerve became sufficient to explore the environment around the neurovascular compression. If there were any other compressing vessels, they were decompressed using small pieces of Tachocomb (Nycomed, Linz, Austria), or Teflon sponge (Fig. 2). The transposed vessel was further secured with fibrin glue (BAXTER, Vienna, Austria) to ensure the REZ of the facial nerve was free from any offending vessels.
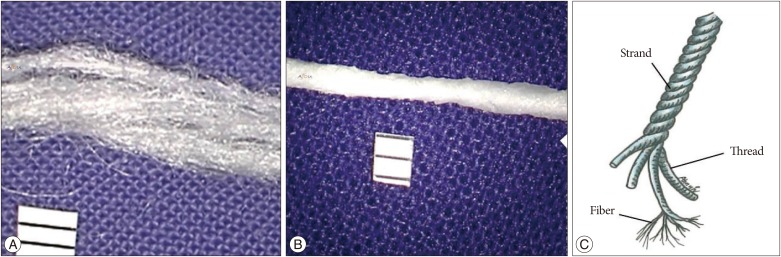 | Fig. 1Preparation of hand-made bioglue-coated Teflon sling. Several Teflon threads were prepared (A) and these were manually twisted with application of bioglue to make an elongated bioglue-coated Teflon strand with a smooth-surface that was lint-free and had good tensile strength (B). Schematic illustration of the stranded Teflon (C). Scale=1 mm.
|
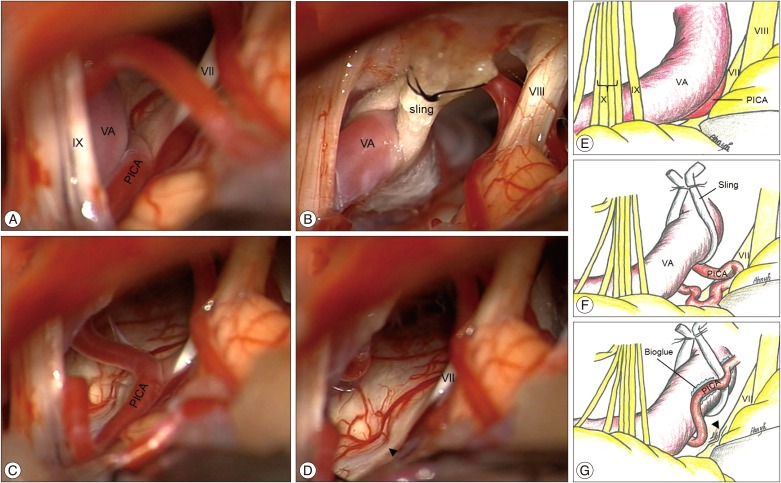 | Fig. 2Intraoperative microscopic view during MVD. A : The loop of the VA and the PICA are seen compressing the root exit zone (REZ) of the facial nerve. B : The VA was adequately lifted using the sling, which was fixed to the 5-0 black silk sutures on the petrosal dura. C : PICA was fully identified on the REZ only after transposition of the VA. D : An indentation was seen on the REZ after the decompression (arrowhead). E : Schematic illustration showing compression of the facial nerve by the VA and the PICA. F : After transposition of the VA using a bioglue-coated Teflon sling, the PICA compressing on the REZ of the facial nerve is fully identified. G : The PICA was fixed to the transposed VA with applications of several pieces of TachoSil (Takeda GmbH, Linz) and Tisseel bioglue (Baxter). MVD : microvascular decompression, VA : vertebral artery, PICA : posterior inferior cerebellar artery.
|
Intraoperative electromyogram (EMG) (Endeavor CR; Natus Medical, Pleasanton, CA, USA) was performed to monitor the changes in lateral spread response according to operative progression and the brainstem auditory evoked potential (BAEP) (Viasys Healthcare, Conshohocken, PA, USA) was also monitored throughout the operation. All operations were performed by a single surgeon.
Postoperative evaluation
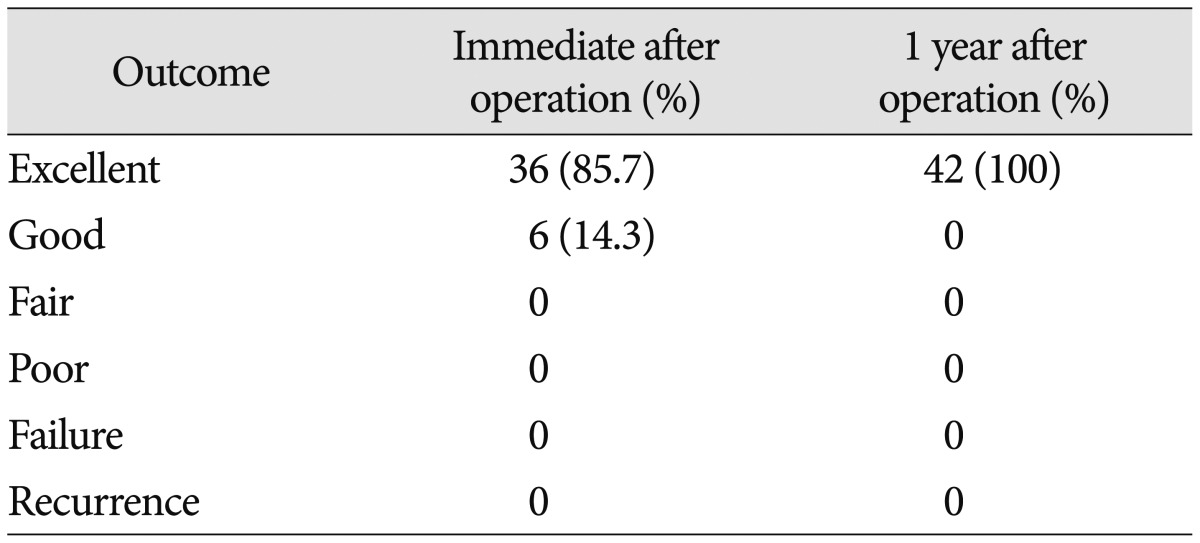
To evaluate postoperative outcomes, the assessment system based on the degree of HFS was used17). The degree of HFS was divided into five categories depending on remaining grade of facial spam following surgery (excellent : no HFS remained, good : more than 90% of HFS resolved, fair : more than 50% HFS resolved, poor : less than 50% HFS resolved, failure : no improvement)17). Clinical outcomes classified as excellent or good on the postoperative grading system were defined as successful.
Go to :
RESULTS
Demographic distribution
There was no sex-related bias (22 men and 20 women) and the mean age of the patients was 52 years (range 22–71 years). The mean duration of preoperative symptom was 3.2 years. HFS was predominantly located on the left side (32 patients, 76.1%). The mean follow-up duration was 76 months (24–132 months) after surgery. Concomitant medical diseases included hypertension (16 patients, 38.1%), diabetes mellitus (3 patients, 7.1%), and cardiac disease (0 patients, 0%). Atherosclerotic changes in the large vessels were observed during the surgery in 21 cases (50%).
Concomitant compressing vessels or conditions
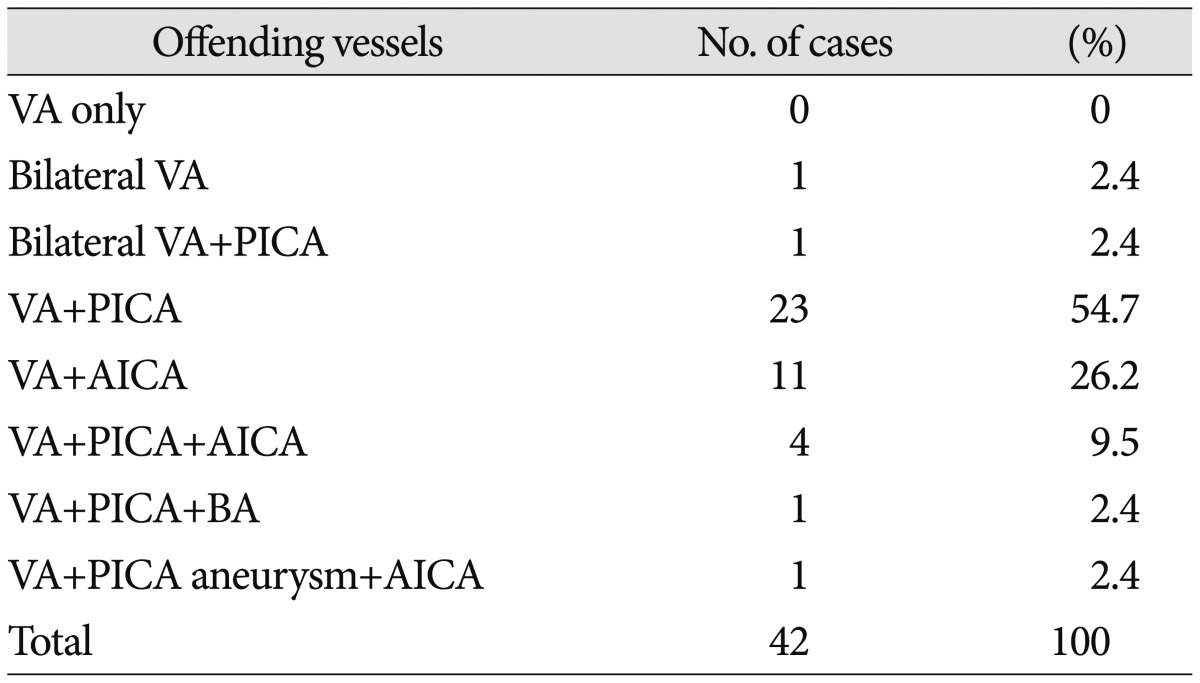
There were always one or more other compressing vessels in addition to the VA in all cases (Table 1). Among another compressing arteries involved in tandem with the VA, PICA was the most common (54.7%) followed by AICA (26.2%). VA-PICA aneurysm was also found in one patient.
Postoperative outcomes
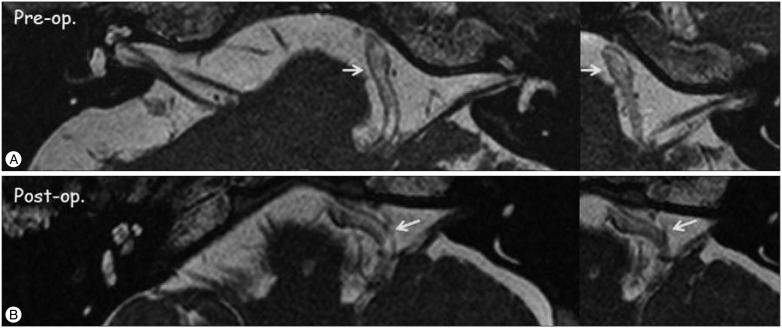
All 42 patients became asymptomatic after the MVD (Table 2). Of the 42 patients, 36 showed complete recovery immediately after MVD, whereas the remaining 6 patients experienced residual spasm to a reduced extent only in the periorbital area. By the 2-month postoperative follow-up, however, these six patients had become spasm-free. None of the 42 patients experienced recurrence for 2 years after the surgery. Pre- and postoperative MRI showed a VA compressed REZ of the facial nerve (upper panel) and a transposed VA with a sling after operation, respectively (Fig. 3).
Complications
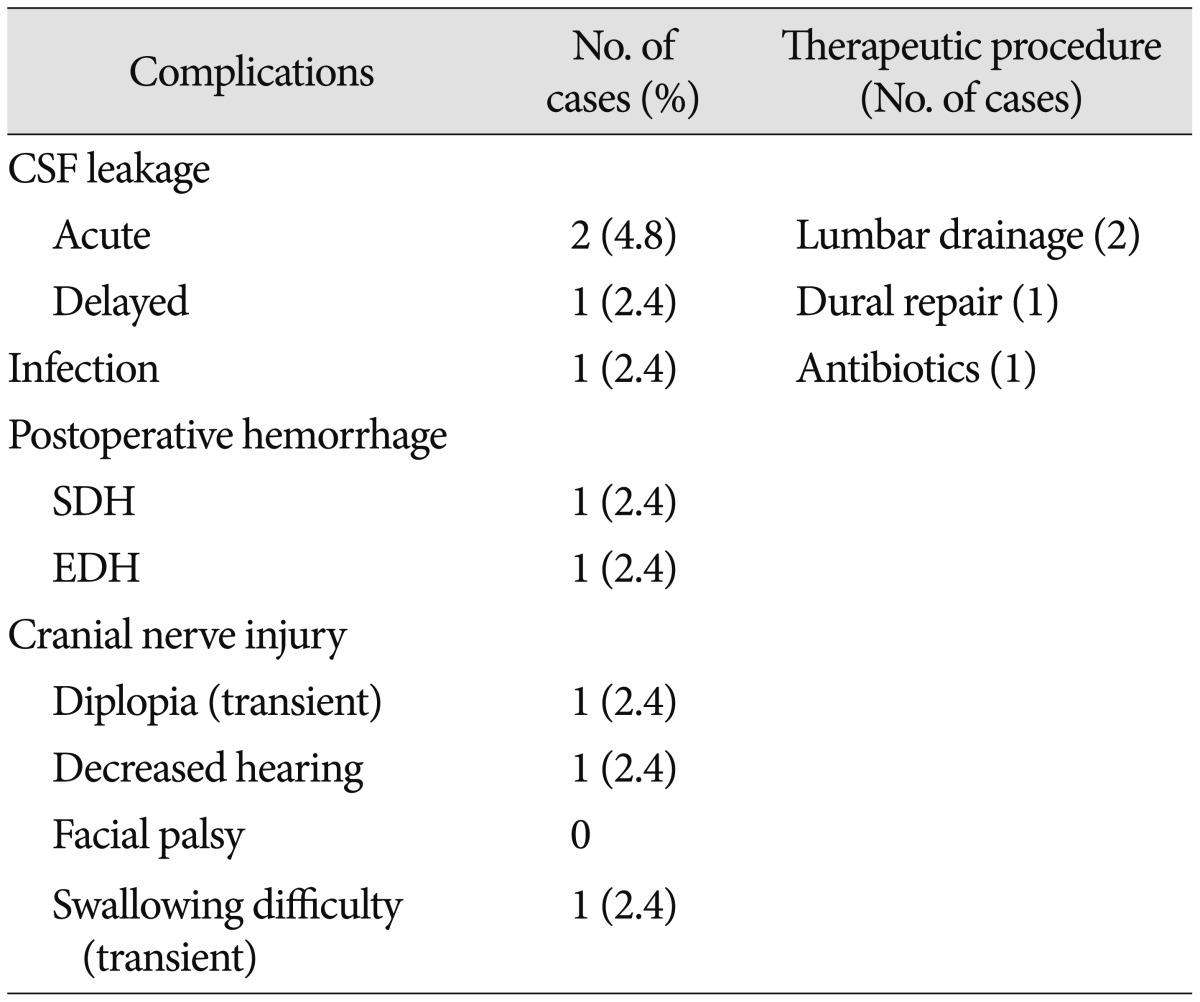
There were no cases of either symptomatic perioperative stroke or postoperative mortality. No postoperative facial palsy was noted (Table 3). One patient developed permanent deafness despite thorough monitoring of AEP throughout the MVD. One epidural and one subdural hematoma developed after MVD in one case each, but neither required evacuation surgery. One patient experienced temporary postoperative dysphagia for 2 months and another patient complained diplopia, which lasted 3 months after the MVD. CSF leak developed in three patients (7.1%); two of them were noted in early postoperative stage, whereas the remaining one occurred 2 years after the MVD. The CSF leaks in the early postoperative stage were treated successfully with lumbar drain for 1 week, while the delayed onset CSF leak required dural repair surgery.
Go to :
DISCUSSION
Although MVD has become the gold standard treatment for HFS, individualized and specific techniques are still being developed3102228293039). For example, when the VA is involved in neurovascular compression, manipulation of other compressing arteries, arachnoid membranes, or perforating arteries can be challenging or even impossible due to its greater size and low elasticity. Acknowledging that HFS where the VA is involved deserves special attention, we have employed a novel material to decompress the VA since 2005.
Using a bioglue-coated Teflon sling crafted by the surgeon, the VA was safely lifted such that it no longer compressed other arteries. This technique not only provides more room for surgeons to explore around the REZ but also results in indirect additional decompression on the REZ. Without this additional decompression, too much Teflon sponges may have been required, which could potentially cause injuries to the facial nerve and the brainstem. Complete remission of HFS was achieved in all patients by 1 year after the surgery, and no significant surgery-related neurological deficits were noted, except in one case of postoperative deafness. No recurrence was reported during the 2-year follow-up period.
Larger vessel transposition techniques
Although MVD is a widely accepted procedure, there is still debate regarding the surgical technique, particularly for large vessels to achieve adequate decompression, and the materials used. Surgical techniques to decompress the offending vessels can be categorized into three major types : interposition, shielding, and transposition23). The transposition method, particularly when used for large vessels such as the vertebral artery, could be ideal to keep them away from the facial nerve. Several variants of the transposition technique have been introduced110131821232427333541). Rawlinson and Coakham33) reported sling retraction as a new technique for hemifacial spasm caused by large vessels, such as the VA. They used thin silastic rubber slings in two patients, but experienced one recurrence with serious complications. Aneurysmal clips, such as fenestrated type clips and Sundt aneurysmal clips, were also used as anchoring materials124). However, the long-term follow-up results for this procedure are still unavailable. An anchoring method using a dural sling has been introduced, where the dural sling is harvested from the convexity and is anchored to the dural bridge originating from the petrous dura; an aneurysmal clip is used to anchor the dural sling in this procedure23). A synthetic vascular graft (GORE-TEX) has also been used instead of the dural sling3541). Direct fixation of the offending vessels to the dura using adhesives, such as fibrin glue and collagen fleece-coated fibrin glue, has also been reported as a transposition method1321). This technique, however, may not be suitable for the VA because the adhesives alone may not be sufficiently strong to hold the VA permanently away from the REZ. A technique with direct stitches on the vascular wall of the offending vessel using an 8-0 nylon suture has been reported, where the stitches on the vessel are fixed to the petrosal dura10). A stitched sling retraction technique has also been reported27). However, the sling is not fixed to the vessel, which could cause slippage or kinking of the vessel.
On the other hand, the bioglue-coated Teflon sling used in our series is easy to manipulate even in a narrow surgical space as it has a smooth surface without any lint. Moreover, with this sling, we can avoid any unexpected slippage or uncoiling of the transposed vessel through the sling as it is coated with bioglue, which may help it to adhere to the transposed vessel.
For the suturing procedure, in cases with a narrow surgical field, a half-cut needle could be used with a rubber dam over the cerebellum and cranial nerves. For fixation of the bioglue-coated sling, both ends of the sling are tied to the 5-0 black silk-sutured dura. We have applied this technique since 2005, and the average duration of follow-up has been more than 2 years.
Preoperative consideration
More accurate identification of neurovascular conflicts has become possible with advances in MRI technology. Prior to an MVD, surgeons could predict whether an ordinary surgical technique placing Teflon sponges between the vessel and brainstem would be sufficient or even possible. If preoperative MRI indicates that an ectasic VA is attributed to neurovascular compression, surgeons could assume that traditional MVD may not be sufficient to decompress the nerve. As delayed recurrence of HFS more than 2 years following MVD is extremely rare, our results with zero recurrence during the 2-year follow-up period suggest that lifting the VA using the bioglue-coated Teflon sling is both effective and safe432).
Postoperative complication
The main neurological complication risks of MVD for HFS are facial paralysis, hearing loss, brainstem stroke, vocal cord palsy, cerebrospinal fluid leakage, wound infection, meningitis, intracranial hemorrhage, and reduced cranial nerve dysfunction41125282934). The reported rate of a facial palsy due to MVD ranges from 0.6% to 1.2%12141626). Facial dysfunction may be correlated with unnecessary manipulation of the facial nerve or insufficient decompression10). With the additional effects of decompression due to lifting of the VA using the bioglue-coated Teflon sling, excessive use of Teflon sponges on the REZ can be avoided and successful decompression can be achieved without manipulating the facial nerve, thus minimizing the risk of postoperative facial palsy.
Hearing loss in the ipsilateral ear has been reported in 0.5–8.2% of cases1214162640). Some groups have reported a higher rate of hearing loss when the VA is the offending vessel29). Possible causes of hearing loss following MVD include cerebellar retraction-induced stretching of the acoustic nerve, vascular injury, manipulation-related injury to the nerve, iatrogenic compression on the nerve by the Teflon prosthesis, and even overinfused saline during dural closure25). It would be advisable to carefully place a retractor on the cerebellum, perpendicular to the axis of the acoustic nerve25). Intermittent release of the retractor, based on the intraoperative BAEP monitoring, would also help to prevent possible hearing loss25). Some authors have suggested that performing the procedure without the use of fixed retraction may help reduce hearing loss38). We have also performed MVD surgery using a retractor, and particularly when the VA is the causative offending vessel, intermittent retraction on the cerebellum was needed to prevent the development of hearing loss. During the stitching procedures on the petrosal dura, as a needle could injure surrounding tissue, a rubber dam was applied over the cerebellar surface and cranial nerves. Frequent irrigation with warm saline to prevent tissue drying was also applied to prevent hearing loss.
Pragmatic suggestion
Wide dissection of the arachnoid membrane is crucial for the current procedure using a bioblue-coated Teflon sling. The VA, in addition to its greater diameter by nature, can be associated with ectasis, aneurysm, or atherosclerosis, thus precludes proper access around the REZ. Application of the Teflon sling to the VA should be attempted only after wide and thorough dissection of the arachnoid membrane. Wider dissection can help to prevent not only possible damage to the cranial nerves derived from saline overinfusion, but also ischemic injury to the brainstem due to disruption of the perforating arteries39). Our results indicated that there were one or more other compressing arteries or conditions in tandem with the VA. The VA as the single cause of neurovascular compression has been reported in 1.1–8.5% of cases, whereas the frequency of the VA as one cause of compression along with other arteries has been estimated to be 7.5–18%612151636). In the present study, all patients had one or more other compressing arteries along with the VA. Therefore, additional procedures for REZ decompression were needed after completion of VA transposition with a bioglue-coated Teflon sling in all cases. Both our results and those described in the literature indicate that the VA only rarely contributes to neurovascular compression as the single cause.
Therefore, the decompression procedure should not be finished after removal of only one cause of neurovascular compression without a thorough investigation of other possible causes, particularly when the VA is suspected to be involved prior to surgery.
This study had some limitations in that it was a retrospective review with a relatively small number of patients. Therefore, further prospective comparative studies between groups with and without use of the bioglue-coated Teflon sling are required.
Go to :
 XML Download
XML Download