

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although this generation of mechanical thrombectomy (MT) techniques, including stent retriever and direct thrombus aspiration, has resulted in higher recanalization rates compared to previous generations6811161821), acute internal carotid artery (ICA) occlusion with extensive clot-burden still can result in poor outcomes, perhaps as a result of difficult recanalization, higher complication rate, or non-involved-territory embolization41019). There have been a few attempts to introduce a method for reducing clot-burden by manual clot aspiration, either through a balloon-tipped guide catheter (BGC) or a non-BGC31222).
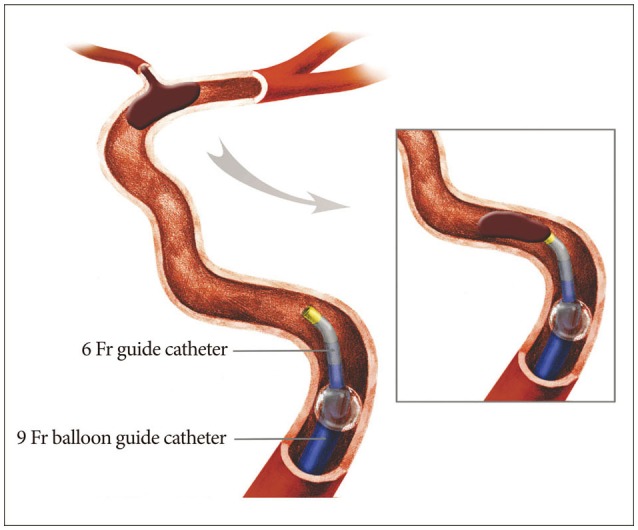
We routinely practiced proximal aspiration thrombectomy (PAT) for clot-burden reduction in the cases of intracranial ICA occlusion since the BGC was introduced in Korea. Our method PAT involved manual clot aspiration using a 50 cc syringe at the cervical segment ICA through a 6 Fr coaxial guide catheter, while the balloon of the outer 9 Fr BGC was inflated. After a few attempts of PAT, our standard MT involving forced arterial suction thrombectomy (FAST) with the Penumbra reperfusion catheter (Penumbra Inc., Alameda, CA, USA) and/or Solitaire stent (Covidien, Irvine, CA, USA) thrombectomy was followed to recanalize the remaining occlusion.
The primary purpose of this study was to evaluate the efficacy of the aforementioned PAT for clot-burden reduction in cases of acute intracranial ICA occlusion by comparing procedure time and angiographic (Thrombolysis in Cerebral Infarction, TICI)5) and functional (modified Rankin Scale, mRS) outcome between two treatment periods (period 1 : standard MT without PAT; period 2 : PAT first, then standard MT for the remaining occlusion).
MATERIALS AND METHODS
Patient selection
The subjects were retrospectively analyzed from a prospectively-maintained stroke registry. We reviewed 112 consecutive patients from a five-year period who received MT for acute intracranial ICA occlusion. The inclusion criteria for MT were as follows : 1) acute ischemic stroke corresponding to intracranial ICA occlusion on CT angiography or MR angiography; 2) infarction volume on DWI or CT less than half of the corresponding vascular territory. We excluded 26 patients with ICA occlusion thought to be caused by preexisting severe stenosis at the carotid bulb where urgent carotid angioplasty and/or stenting for recanalization were required. Local institutional review board approved this study for retrospective analysis.
Endovascular recanalization strategy and assessment
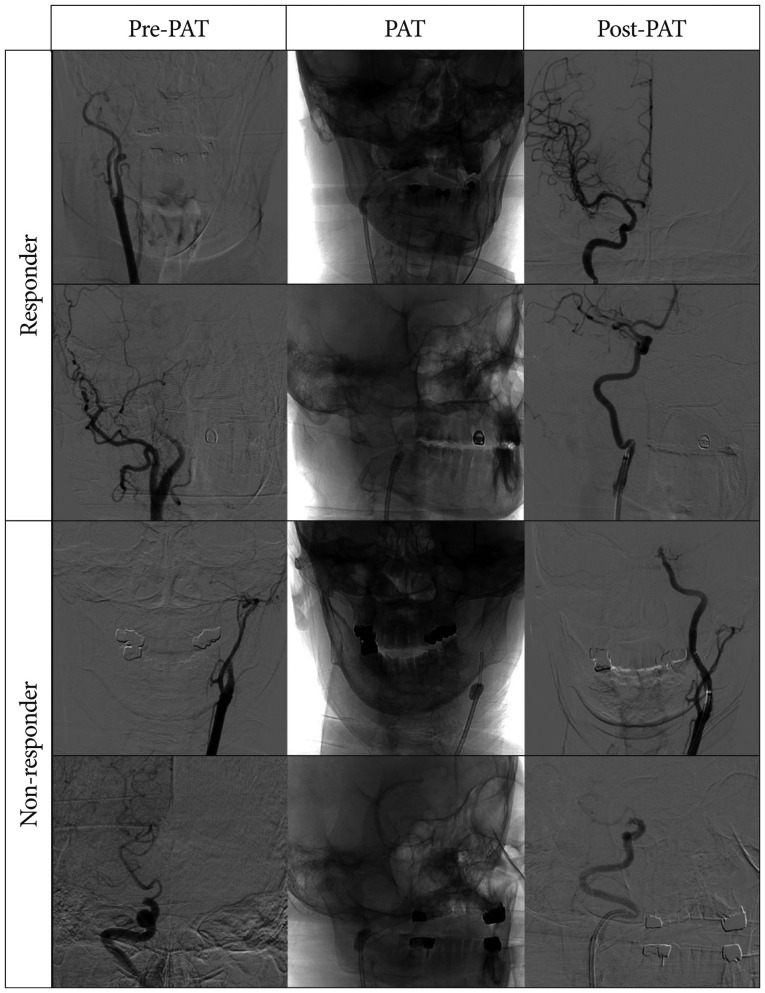
After inspection of treatable ICA occlusion by diagnostic angiography, MT was performed by 2 experienced neurointerventionists under local or general anesthesia. In period 1 (from May 2009 to June 2011), our standard MT with FAST using the Penumbra reperfusion catheter and/or the Solitaire stent was directly performed at the occlusion level of intracranial ICA. Techniques for FAST and Solitaire thrombectomy are the same as previously described81418). In period 2 (from July 2011 to June 2014), the MT procedure was initiated by PAT, which was comprised of manual clot aspiration using a 50 cc syringe at the cervical segment ICA through a 100-cm long 6 Fr coaxial guide catheter (Envoy; Cordis, Miami Lakes, FL, USA) while the balloon of an outer 85-cm long 9 Fr BGC (Optimo; Tokai Medical, Aichi, Japan) was inflated (Fig. 1). We defined 'responder' as a case where some amount of clot was retrieved and the following angiography showed partial or full reperfusion after PAT (Fig. 2, upper two rows). If the following angiography still demonstrated ICA occlusion after PAT, the case was regarded as 'non-responder' (Fig. 2, lower two rows). After a few attempts of PAT, subsequent MT was undertaken to recanalize the remaining occlusion using FAST and/or stent retriever. Once the Solitaire stent became available in October 2010, Solitaire stent thrombectomy followed FAST in refractory cases9).
Neurological deficit was assessed with the National Institute of Health Stroke Scale (NIHSS) at baseline, 1 day, and 7 days. A brain CT scan was performed 24 hours after endovascular treatment and in case of neurological deterioration. Reperfusion was measured using the TICI scale and was counted as successful if TICI 2b-3 was achieved in the final angiography. Symptomatic intracranial hemorrhage (ICH) was defined as any hemorrhage with an increase in NIHSS score of 4 or more within 24 hours18). The mRS was used to evaluate functional outcome at 3 months after index stroke, and mRS 0–2 was defined as a favorable functional outcome.
RESULTS
Eighty-six patients with acute intracranial ICA occlusion were treated with MT and were included in this analysis. There were 33 patients in period 1 and 53 in period 2. PAT was effective in 28.3% (15/53) of patients in period 2, resulting in complete recanalization for 5 and incomplete recanalization for the other 10 (Fig. 2).
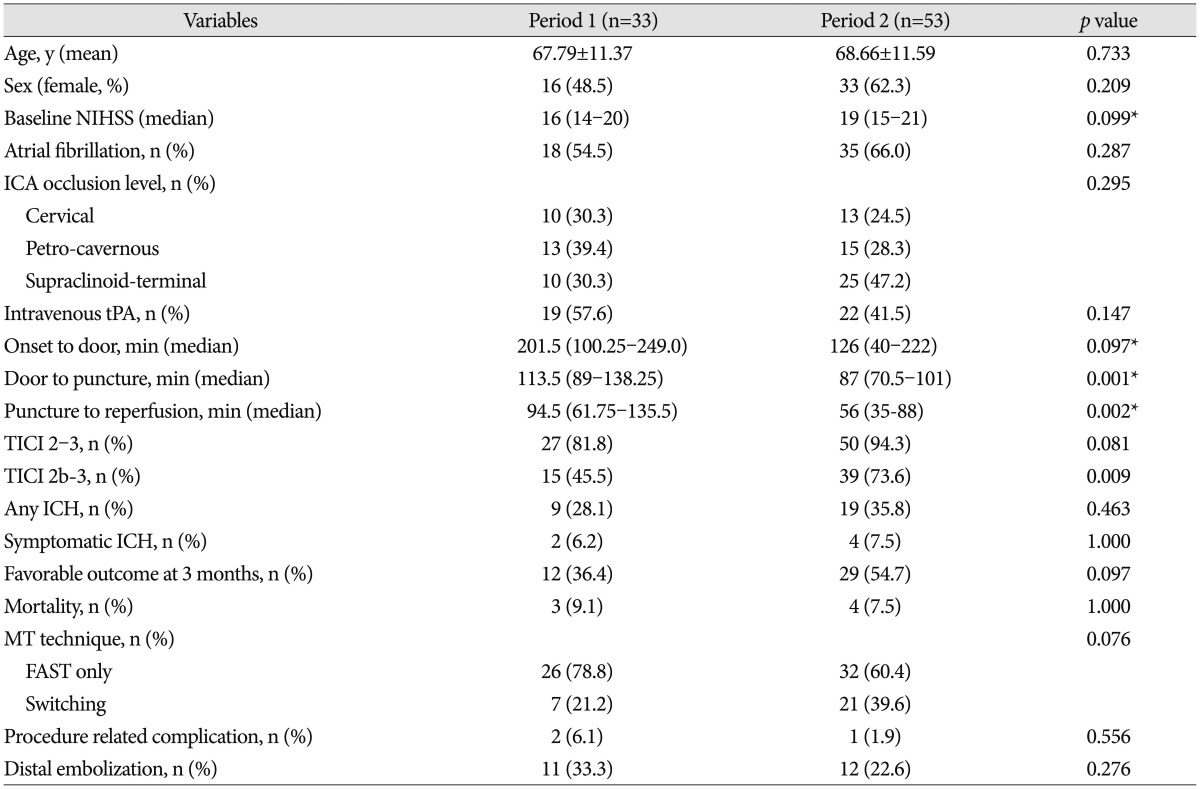
No clinically relevant differences were found in the baseline characteristics between the 2 groups, with the exception of door-to-puncture time (Table 1). The median puncture-to-reperfusion time was 94.5 minutes in period 1 and 56.0 minutes in period 2, a difference that was statistically significant (p=0.002). TICI of 2b-3 reperfusion was achieved in 15 of 33 patients in period 1 and 39 of 53 patients in period 2, with significantly better reperfusion in period 2 (45.5% vs. 73.6%; p=0.009). And also, distal embolization was non-significantly less in the period 2 (33.3% vs. 22.6%; p=0.276). There was only a trend for better 3-month favorable outcome in period 2 (36.4% vs. 54.7%; p=0.097). There were no significant differences between the 2 groups regarding the incidence of procedure-related complications and symptomatic ICH (p=0.556 and p=1.000, respectively). In the subgroup analysis between 'responder' (n=15) and 'non-responder' (n=38) in period 2 (Table 2), there was a significantly higher incidence of atrial fibrillation in the responder subgroup (86.7% vs. 57.9%; p=0.046). The median puncture-to-reperfusion time was significantly shorter in the responder subgroup (31 minutes vs. 71 minutes; p=0.001), and the rate of TICI 2b-3 reperfusion also showed a better tendency in the responder subgroup (93.3% vs. 65.8%; p=0.080). However, there was no significant difference in 3-month favorable outcome (66.7% vs. 50.0%; p=0.272). Regarding the subsequent MT method for the remaining occlusion after PAT, only 6.7% (1/15) of responders were treated with FAST-to-Solitaire switching, compared to 52.6% (20/38) of the non-responders.
DISCUSSION
It is widely known that an occlusion at ICA location itself can be regarded as an important indicator of poor prognosis19). The presence of a larger clot-burden in the ICA occlusion compared to other locations could be one major cause of such a poor clinical course1). A larger thrombus volume results in a smaller surface area-to-thrombus ratio at the occlusion site, which presumably can decrease the efficacy of intravenous thrombolysis with tissue-type plasminogen activator and MT21320). In addition, the potential for non-target embolization of uninvolved territories can be another practical concern during MT in such cases10). To date, timely recanalization is the only procedure that has been shown to improve outcome717). In that regard, there have been several attempts to reduce clot-burden during MTs for acute ICA occlusions to achieve better angiographic and functional outcome31222).
In our practice, standard MT using FAST and/or Solitaire stent was directly undertaken at the occlusion level of the intracranial ICA in period 1. However in period 2, we routinely began with PAT for clot-burden reduction in such cases, which featured manual clot aspiration at the cervical segment ICA with a 6 Fr coaxial guide catheter through a 9 Fr BGC; then we followed with the standard MT as in period 1 for the cases of remaining occlusions. This study highlights the role of PAT with BGC by comparing variables between the 2 periods with different MT protocols for intracranial ICA occlusions.
The main findings of this study were the following : 1) there was a significantly shorter puncture-to-recanalization time (p=0.003), a significantly higher rate of TICI 2b-3 recanalization (p=0.009), but only a trend for better 3-month favorable outcome (p=0.097) in period 2 compared to period 1; 2) PAT was effective in 28.3% (15/53) of the patients in period 2, where complete recanalization occurred in 5 and incomplete recanalization in the other 10 (Fig. 2); 3) in the subgroup analysis between 'responder' and 'non-responder' in period 2, there was a higher incidence of atrial fibrillation (p=0.046) and a significantly shorter puncture-to-recanalization time (p=0.008) in responder subgroup; on the other hand, there was only a trend for higher TICI 2b-3 recanalization (p=0.080) and no significant differences in 3-month favorable outcome (p=0.272).
Regarding the MT techniques used for any remaining occlusion, there was a significantly higher number of FAST-to-Solitaire switching in non-responder subgroup (1/15, 6.7% in responder vs. 20/38, 52.6% in non-responder, p=0.002). This can be explained by noting that most of the subsequent MT in the responder subgroup was simply finished without additional Solitaire thrombectomy; but in the non-responder subgroup, the following MT was not always easy, and 52.6% required FAST-to-Solitaire switching. As previously published9), FAST-to-Solitaire switching can play some role in achieving better angiographic and functional outcome in difficult cases. Thus, we hypothesized that more case numbers of switching in the non-responder subgroup could be one possible explanation of the non-significant differences in TICI 2b-3 recanalization and 3-month favorable outcome in the subgroup analysis between 'responder' and 'non-responder'.
PAT can have several advantages. First, this procedure can be applied easily and quickly. This just requires the advancement of a 6 Fr guide catheter through a 9 Fr BGC, followed by manual aspiration. Two or three attempts of this procedure take only a few minutes; and if the case is refractory, an institutional MT protocol can easily follow. Second, this method was safe without elevating procedure-related complications or ICH. This required no advancement of additional devices to the intracranial artery; thus, the chance of complications may be minimal. Third, this can be more effective than the historically-performed clot aspiration technique under manual compression of the common carotid artery1522) because a BGC can make a definite proximal flow arrest. Finally, we can apply an intermediate guide catheter; for example, Distal Access Catheter (Concentric Medical, Mountain View, CA, USA) or Navien catheter (Covidien, Mansfield, MA, USA), as a substitute for the 6 Fr guide catheter during PAT, which may be more effective because such catheters can be advanced more distally.
The application of BGC played an important role for the PAT and subsequent standard MT. First, in the general aspiration thrombectomy, aspiration using pump or syringe was performed after contact between thrombus and reperfusion catheter. However, PAT was performed distant proximal area without facing between thrombus and reperfusion catheter. Therefore, proximal flow arrest by BGC could establish temporary closed space, which was theoretically better circumstance for PAT. Second, during subsequent standard MT, the rate of distal embolization was non-significantly less in the Period 2 (33.3% vs. 22.6, p=0.276). Although similar MT strategy was applied between periods, time from groin puncture to recanalization was shorter in the period 2. And also, in the comparison between period 1 and non-responder of period 2, time from groin puncture to recanalization revealed shorter tendency in the non-responder of period 2 (94.5 min vs. 71.0 min, p=0.052) and successful recanalization rate demonstrated higher tendency (45.5% vs. 65.85%, p=0.085). These results were comparable with previous studies1415).
However, this study has several potential limitations. Although the patients were enrolled prospectively, the data were analyzed retrospectively. Therefore, the treatment groups were not randomized and concurrent. And, as we previously discussed, the difference in number of switching cases between both periods could be a bias in the interpretation of the present data. In addition, there was a baseline imbalance for door-to-puncture time between the two periods. The door-to-puncture time was significantly reduced in period 2, which might have resulted from increased experience at the system level. Therefore, we could not exclude the possibility that this imbalance influenced the outcome.
CONCLUSION
The present study compared two different strategies for intracranial ICA occlusion with similar baseline characteristics. Based upon the data, PAT effective in 28.3% of the cases, which resulted in shorter puncture-to-recanalization times and significantly higher TICI 2b-3 recanalization rates without increasing the incidence of procedure-related complications or ICH. However, these results should be interpreted cautiously because of the aforementioned limitations, and confirmation by prospective multi-center trials seems necessary.

 XML Download
XML Download