

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Meningiomas are the most common type of primary intracranial or spinal tumors10). The majority of meningiomas are benign, with malignant meningiomas comprising only 1 to 2% of all diagnoses. In the current World Health Organization (WHO) criteria, benign meningiomas are recognized by their histologic subtype and lack of anaplastic features10). WHO grade III malignant meningiomas have rhabdoid or papillary subtypes, histological features of frank malignancy resembling that of carcinomas, melanomas, or high-grade sarcomas, or 20 or more mitoses per 10 high-power fields (HPFs)10).
Meningiomas with rhabdoid or papillary components are aggressive clinically and biologically, leading to high mortality46815). All patients with malignant meningiomas have poor prognoses, but neither clinical courses nor pathologic and radiologic characteristics of rhabdoid or papillary meningiomas are known due to low incidences1).
In this study, meningiomas with rhabdoid or papillary components were divided into two groups, those with and without predominant rhabdoid or papillary components. We analyzed clinical, radiologic, and pathologic findings in patients with meningiomas with and without predominant rhabdoid or papillary components and compared those findings to those for anaplastic meningiomas.
MATERIALS AND METHODS
Clinical characteristics
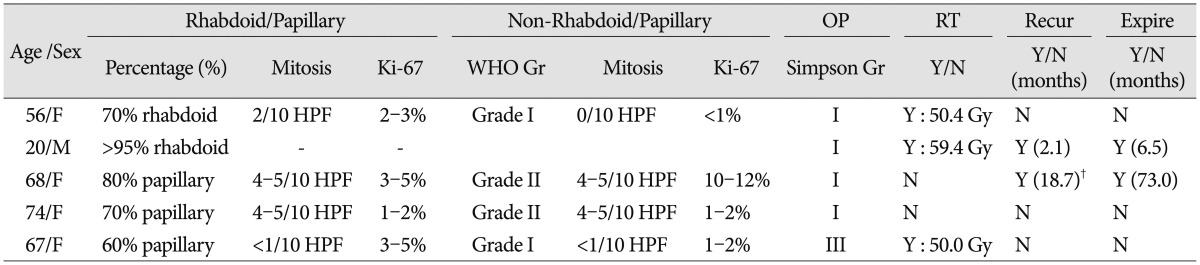
Twenty-five patients were diagnosed with malignant meningiomas from 1994 to June 2013. This retrospective study was approved by our institutional review board (IRB No: CNUHH-2015-100), and the need for written informed consent was waived. Pathologic diagnoses, according the WHO classification, were anaplastic meningioma (n=14), meningioma with a rhabdoid component (n=6), and meningioma with a papillary component (n=5)10). The meningiomas with a rhabdoid or papillary component (total=11) were further divided into meningiomas with a predominant (≥50%) rhabdoid (n=2) or papillary (n=3) component and meningiomas without a predominant (<50%) rhabdoid (n=4) or papillary (n=2) component. In total, all patients were divided into three groups. Group A patients had anaplastic meningiomas. Patients with meningiomas containing a predominant (≥50%) papillary or rhabdoid component were in group B1, and patients with meningiomas not containing a predominant (<50%) rhabdoid or papillary component were in group B2.
The mean age of the patients was 52.9 years (range, 20–74 years), and there were 15 women and 10 men. The mean symptom duration was 3.4 months (range, 0.1–12 months). The main clinical symptoms included headache in 12 patients, nausea and vomiting in 3 patients, seizures in 4 patients, altered mental state in 4 patients, hemiparesis in 1 patient, and visual disturbance in 1 patient. The Eastern Cooperative Oncology Group (ECOG) performance status (PS) scale (0 to 3) was used to assess patients before and after surgery14). Pre-operative ECOG PS scores were 0 in 8 patients, 1 in 8 patients, 2 in 7 patients, and 3 in 2 patients.
Pre-operative magnetic resonance imaging (MRI) was performed with gadolinium enhancement. Lesions were classified according to size, location, severity of peri-tumoral edema (none, mild, moderate, or severe), shape of tumor (well circumscribed or mushroom pattern), signal intensity (low, iso, or high) on T2-weighted images (T2WI), and enhancement pattern (homogeneous or heterogeneous). Mild peri-tumoral edema measured less than half of the longest tumor diameter on the axial view; moderate edema measured more than half, but less than twice and severe edema measured more than twice.
The extent of tumor removal was estimated by the Simpson grading system and was primarily determined according to the judgment of the neurosurgeons. The extent of tumor removal was validated by reviewing post-operative gadolinium-enhanced computed tomography scans16). After surgery, patients underwent follow-up gadolinium-enhanced MRI every 6 months. New lesion development or remnant mass enlargement was considered recurrence.
Statistical methods
We defined the mean range as the follow-up length and determined the effects of single variables on progression-free survival (PFS) and overall survival (OS) via univariate and multivariate analyses. The variables were radiologic parameters, extent of removal, pathologic subtype, and adjuvant treatment. PFS was calculated from the date of surgery to the date of radiological progression or last follow-up visit, and OS was calculated from the date of surgery to the date of death or last follow-up. We calculated survival probability using the Kaplan-Meier method and performed comparisons using the log-rank test. We examined all variables using the Cox proportional hazard analysis to identify independent predictors of survival. All statistical analyses were performed at a significance level of p<0.05 using the statistical package SPSS 21.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Radiologic findings, extent of tumor removal, and adjuvant treatment
The clinical characteristics are summarized in Table 1.
Among the 14 group A anaplastic meningiomas, the mean tumor size was 4.1 cm (range, 1.1–8.8 cm). The mass was in the convexity in 6 patients, in the parasagittal area in 4 patients, at the sphenoid ridge in 3 patients, and at the jugular foramen in 1 patient. Three patients had mild peri-tumoral edema, 6 patients moderate edema and 2 patients severe edema. Tumors were well-circumscribed in 13 of 14 patients. T2WI signal intensity was low for 4 tumors, iso for 5 tumors, and high for 5 tumors, with 9 tumors having homogenous enhancement and 5 having heterogeneous enhancement. Among the 5 group B1 meningiomas with ≥50% rhabdoid or papillary component, the mean size of tumor was 2.9 cm (range, 0.7–5.7 cm). The mass was in the convexity in 3 patients, in the parasagittal area in 1 patient, and periventricular in 1 patient. Peri-tumoral edema was present in 4 of 5 patients (1 mild, 2 moderate, and 1 severe), and 4 of the 5 tumors were well-circumscribed. The T2WI signal was low for 2 tumors, iso for 1 tumor, and high for 2 tumors, with 2 tumors having homogenous enhancement and 3 having heterogeneous enhancement. Among the 6 group B2 meningiomas with <50% rhabdoid or papillary component, the mean tumor size was 3.15 cm (range, 2.1–4.4 cm). The mass was in the convexity in 3 patients, in the parasagittal area in 1 patient, in the periventricular in 1 patient, and in the olfactory groove in 1 patient. There was peri-tumoral edema in 5 of 6 patients (mild in 3, moderate in 1, and severe in 1). Tumors were well-circumscribed in 6 patients. The T2WI signal intensity was low for 2 tumors, iso for 1 tumor, and high for 3 tumors. Four of the tumors had homogenous enhancement, and 2 had heterogeneous enhancement.
Gross total resections, which were Simpson grades I and II, were achieved in 24 (grade I, n=18; grade II, n=6) of the total 25 patients (96%). The remaining patient (n=1) had a Simpson grade III resection. The post-operative ECOG PS scores were 0 in 8 patients, 1 in 8 patients, 2 in 7 patients, and 3 in 2 patients. Post-operative complications included the low cranial nerve symptoms of swallowing difficulty in 1 patient, seizures in 1 patient, hemiparesis in 2 patients, and cerebrospinal fluid leakage in 2 patients.
Among group A patients (n=14), Simpson grade I resection was achieved in 10 patients, and grade II resection was achieved in 4 patients. All 14 patients in this group received adjuvant radiotherapy (mean dose, 54.2 Gy; range, 36.0–60.0 Gy). Among group B1 patients (n=5), Simpson grade I resection was achieved in 4 patients, and grade III resection was achieved in 1 patient because of tumoral adhesion to cranial nerves. Three of 5 patients received post-operative radiotherapy (mean dose, 53.3 Gy; range, 50.4–59.4 Gy). Two patients refused radiotherapy because of their old age. Among group B2 patients (n=6), Simpson grade I resection was achieved in 4 patients, and grade II resection was achieved in 2 patients. Two patients received adjuvant radiotherapy (mean dose, 52.2 Gy; range, 50.4–54.0 Gy) because of atypical meningioma in the non-rhabdoid/papillary portion.
Progression-free survival and overall survival
Among all 25 patients with meningiomas, the mean follow-up duration was 72.5 months (range, 5.6–214.9 months). The mean PFS was 49.9±12.1 months, and the mean OS was 59.7±16.8 months.
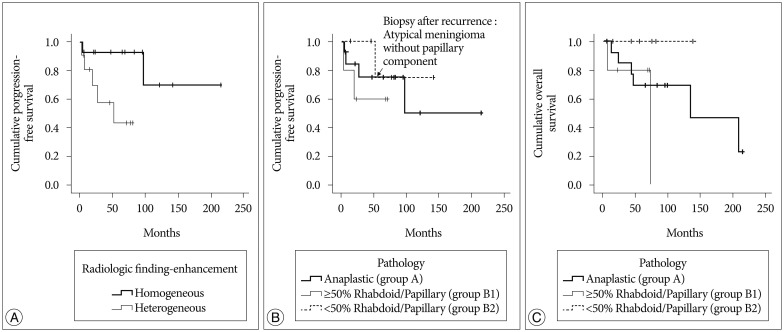
With respect to radiologic tumor characteristics (Table 1), homogenous enhancement was associated with better PFS (172.3±26.8 months) than heterogeneous enhancement (48.4±10.3 months) (p=0.025) (Fig. 1A), and patients with tumors with heterogeneous enhancement had poorer PFS compared to patients with tumors with homogeneous enhancement by multivariate analysis (hazard ratio : 18.432, 95% confidence interval, 1.723–198.195, p=0.016).
Based on pathologic subtypes, the mean PFS was 134.9±31.6 months for group A patients, 46.64±13.4 months for group B1 patients, and 118.7±19.2 months for group B2 patients (p=0.514) (Fig. 1B).
The mean OS was 138.5±24.6 months for group A patients and 59.7±16.8 months for group B1 patients. There was the different OS between group B1 and B2 patients without statistical significance (p=0.05) (Fig. 1C).
World Health Organization pathologic classification and clinical course of meningiomas with a rhabdoid or papillary component
Eleven of 25 meningiomas had a rhabdoid or papillary component. Five of these 11 meningiomas had ≥50% rhabdoid or papillary components (Group B1). Among these, the non-rhabdoid or non-papillary component was WHO grade I in 2 patients and grade II in 2 patients. One tumor was comprised mostly of rhabdoid components. Three of these 5 patients received post-operative radiotherapy, and two patients refused adjuvant treatment. There were 2 disease-related deaths during follow-up. One patient whose tumor was mostly rhabdoid had tumor dissemination into the cerebrospinal fluid. Another patient whose tumor was mostly papillary component had local recurrence with distant metastases to the spine.
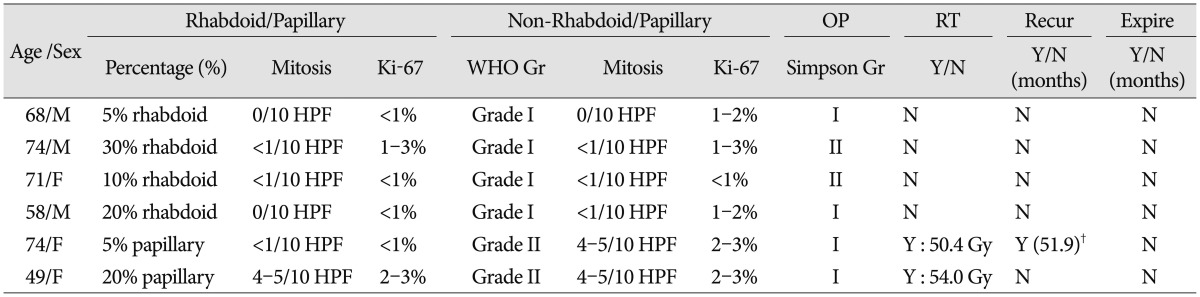
Among the 6 meningiomas with <50% rhabdoid or papillary components (Group B2), the non-rhabdoid or non-papillary tumor components were WHO grade I in 4 patients and grade II in 2 patients. Two patients with WHO grade II meningiomas underwent post-operative radiotherapy. One patient in this group experienced tumor recurrence, and the recurrent tumor was an atypical meningioma without a papillary component.
DISCUSSION
Most meningiomas are benign, and malignant meningiomas are uncommon. Because of low incidences, the clinical information of malignant meningiomas is limited even though it is generally known that they have a poor prognoses compared to benign meningiomas. Malignant meningioma commonly occurs in men and is located in the cerebral convexities11). Previously reported malignant meningioma radiologic characteristics include heterogeneous appearance, irregular cerebral surface, irregular borders (mushroom appearance), destruction of adjacent bone, and marked edema51113). However, conventional MRI is not sufficient to discriminate between benign and malignant lesions18). In this study, the MRI finding of heterogeneous enhancement was noted in 10 of 25 cases, and it was associated with early recurrence. The histopathology of malignant meningioma includes frank morphologic anaplasia, which is defined as >20 mitotic figures per 10 HPFs10). WHO classification highlights the increased malignant potential of rhabdoid and papillary meningiomas, which are WHO grade III tumors10).
Papillary meningiomas are characterized by a dominant pseudopapillary pattern, and they usually exhibit brain invasion, local or distant recurrence, and leptomeningeal dissemination71020). Rhabdoid meningiomas have a rhabdoid morphology in the background of other meningioma subtypes and usually develop early recurrence and leptomeningeal dissemination919). In the present study, one meningioma with a dominant papillary component metastasized distantly to the spine, and one meningioma with a dominant rhabdoid component disseminated into the cerebrospinal fluid. To date, there have been few studies about rhabdoid and papillary meningiomas. Some authors have stated that WHO grade III meningiomas have predominant rhabdoid or papillary components, but this is controversial17). Here, we have focused on clinical course in relation to the dominance of rhabdoid or papillary components or the pathologic findings of non-rhabdoid or non-papillary components.
Based on retrospective studies, adjuvant radiotherapy after resection of malignant meningiomas is recommended, and post-operative adjuvant radiotherapy is associated with increased OS21721). Conformal radiotherapy with dose escalation has shown a benefit for local control and survival in patients with malignant meningiomas, and it is important to identify WHO grade III tumors when making adjuvant treatment decisions312). In this study, patients were divided into three groups depending on the pathology. Group A patients had anaplastic meningiomas. Patients with meningiomas containing a predominant (≥50%) papillary or rhabdoid component were in group B1, and patients with meningiomas not containing a predominant (<50%) rhabdoid or papillary component were in group B2. We recommended radiotherapy for group A and B1 patients, and did not recommend radiotherapy for group B2. Four patients did not follow these recommendations. Two group B1 patients chose not to undergo post-operative radiotherapy because of their advanced ages, and two group B2 patients received radiotherapy for atypical meningiomas of non-rhabdoid/papillary lesion. The limitations of this study were the small number of patients and the short-term follow-up. However, we found that group A and B1 patients had similar prognoses, and group B2 patients had relatively more favorable prognoses. There were 2 recurrent tumors in group B1 patients in which the pathology of the recurrent tumors was the same as that of the original lesions. While in one recurrent group B2 tumor, the recurrent tumor was an atypical meningioma without rhabdoid/papillary components.
CONCLUSION
Meningiomas with ≥50% papillary or rhabdoid components (group B1) were more aggressive than those with <50% rhabdoid or papillary components (group B2). In group B2 patients, the pathologic findings of non-rhabdoid/papillary portion could be considered when exploring further adjuvant treatment.

 XML Download
XML Download