

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The early recanalization of occluded vessels in acute ischemic stroke (AIS) has been shown to be associated with improved clinical outcomes and reduced mortality11). Yet until 2004, the only FDA-approved treatment modality for AIS was an intravenous administration with tissue plasminogen activator (tPA). However, because tPA is associated with a low recanalization rate for large vessel occlusions, intraarterial endovascular therapy (EVT), with various mechanical devices such as a retriever stent or aspiration catheter, was developed and has resulted in better recanalization of these larger vessels4712).
Recently, manual aspiration thrombectomy (MAT), using a new generation of easy-to-track large-bore aspiration catheters, as a first approach for AIS has been reported with favorable outcomes5616). However, the benefit of aggressive EVT for occlusion of an isolated M2 segment of a middle cerebral artery (MCA) remains unclear. The purpose of this study was to describe safety, angiographic and clinical outcomes of MAT using Penumbra reperfusion catheter (Penumbra, Alameda, CA, USA) in patients with a solitary M2 occlusion in a single-center analysis.
Go to : 
MATERIALS AND METHODS
This retrospective study was approved by our institutional review board.
Patient selection
From January 2013 to November 2014, 32 patients with AIS secondary to a solitary M2 occlusion were treated with MAT using a penumbra reperfusion catheter as a first-line EVT. All patients were initially evaluated using computed tomography (CT) or magnetic resonance (MR) imaging, and angiographic status of patients was assessed routinely on MR angiography or three-dimensional CT angiography. Inclusion criteria for EVT were an initial National Institutes of Health Stroke Scale (NIHSS) ≥4, no evidence of intracerebral hemorrhage, obvious major vessel occlusion on CT or MR angiography, infarct core volume less than one-third of the MCA territory, perfusion deficit more than two-third of the MCA territory or perfusion deficit volume on MR at least 30% larger than the lesion volume shown on diffusion-weighted MR, and patients within 8 hours from onset of symptoms. A CT scan was routinely performed immediately after the procedure.
On admission, the NIHSS score was assessed by a stroke neurologist. Eligible patients who met standard National Institute of Neurologic Disorders and Stroke criteria were treated with 0.9 mg/kg of IV rtPA3). Subsequent EVT was considered for patients with no neurological improvement within 1 h of IV rtPA, defined as an unchanged NIHSS score from baseline or a worsening neurological deficit.
Recanalization procedure
All procedures were performed under conscious sedation by the same interventional neuroradiologist with 10 years of experience. Written informed consent for the EVT was obtained from all patients or next of kin. After femoral artery puncture, a 100-cm 8 Fr guide catheter (Guider Softip; Stryker, Natick, MA, USA) was advanced as distally as possible through a triple coaxial system, which was assembled by combining the outermost 80-cm 8 Fr shuttle sheath (Shuttle-SL; Cook, Bloomington, ID, USA) and inner 125-cm selection catheter (Headhunter; Cook, Bloomington, ID, USA). Then, systemic anticoagulation was initiated with a 3000-U bolus of intravenous heparin followed by 1000 U/hr infusion. After occlusion of the M2 branch was defined by angiography, a 4MAX Penumbra reperfusion catheter was advanced to the level of the thrombus triaxially over a Rebar 18 microcatheter (EV3, Irvine, CA, USA) and Synchro 0.014-inch guidewire (Stryker, Freemont, CA, USA) under roadmap guidance. At the level of the thrombus, the guidewire and microcatheter were advanced more distally through the thrombus up to the distal M2 segment of the MCA in order to achieve sufficient support to track the reperfusion catheter. Next, we gently advanced the Penumbra catheter and wedged it tightly against the thrombus. Subsequently, the microcatheter and wire were removed and a 20-mL syringe was connected to the proximal hub of the reperfusion catheter. Continuous manual aspiration was performed, maintaining the vacuum state between the tip of catheter and the thrombus while gently withdrawing the Penumbra catheter through the guide catheter (Fig. 1).
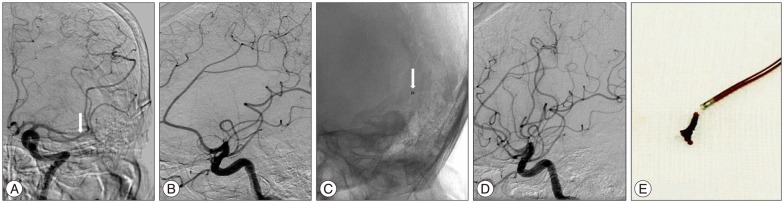 | Fig. 1Patient No. 27. Occlusion of the left M2 superior division. A : An initial anteroposterior angiogram shows occlusion of the proximal portion of the left M2 superior division (arrow). B : An initial lateral projection of angiography shows no visualization of M2 superior branch. C : Positioning of the Penumbra 4 MAX catheter in relation to the clot (arrow). D : An immediate post-procedural angiogram shows complete revascularization (TICI 3). E : Image of the clot retrieved by MAT. TICI : Thrombolysis in Cerebral Infarction, MAT : manual aspiration thrombectomy.
|
Outcome measures
We retrospectively analyzed patient medical records to determine demographic, clinical and angiographic data. The degree of vessel occlusion after treatment was defined by the Thrombolysis in Cerebral Infarction (TICI) scale; successful recanalization after treatment was defined as TICI scale score ≥2b. The NIHSS and modified Rankin scale (mRS) were checked on admission and at 3 months for all patients and a favorable functional outcome was defined as a mRS score of ≤2. Procedure-related symptomatic intracerebral hemorrhage (ICH) was defined as the presence of hemorrhage after treatment with any indication of increasing NIHSS compared to baseline on admission. Mortality was defined as death within 90 days from initial attack. Demographics and outcomes were analyzed using the paired t-test with PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA). Statistically significant differences were defined as p<0.05.
Go to :
RESULTS
From January 2013 to November 2014, one hundred twenty-two patients with AIS in the MCA territory were treated with MAT using a Penumbra reperfusion catheter as a first-line EVT. Of these patients, 32 with solitary M2 occlusions received MAS with Penumbra 4 Max.
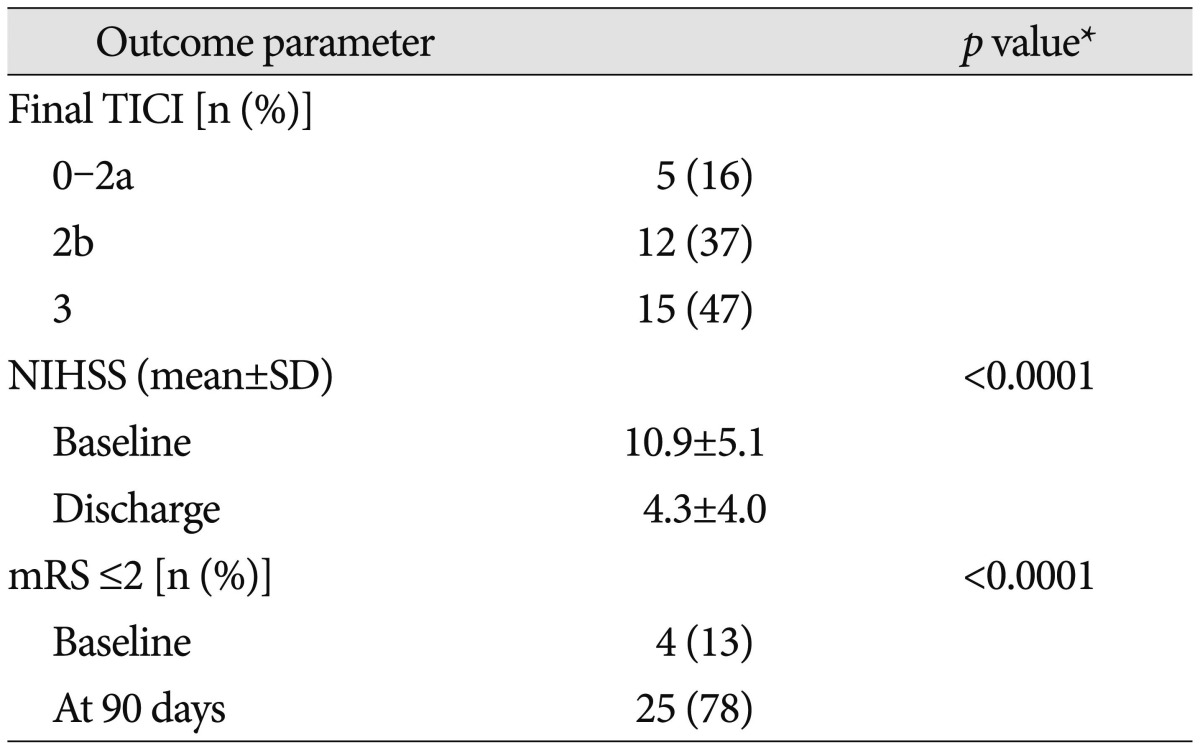
Baseline, clinical and radiologic characteristics of 32 total subjects are shown in Table 1, 2. The mean age of the patients was 70.1±10.8 years (mean±standard deviation); 56% were men (18/32). Sites of occlusion were as follows : right M2 superior division, 37% (12/32); right M2 inferior division, 31% (10/32); left M2 superior division, 16% (5/32); left M2 inferior division, 16% (5/32). The mean interval from the onset of symptoms to groin puncture was 3.9±1.5 hours, and mean procedure time was 33.2±12.6 minutes. Final recanalization result of TICI ≥2b was achieved in 84% (27/32), and TICI 3 in 47% (15/32) of patients. Baseline NIHSS score was 10.9±5.1, and improved to 4.3±4.0 by the time of discharge. Favorable functional outcomes (mRS score ≤2 at 3 months) resulted in 25 out of 32 (78%) patients, with one death occurring after discharge (Table 3). There were three cases of procedure-related small ICH, but without neurologic deterioration.


Go to :
DISCUSSION
Infarction of the MCA territory accounts for the largest proportion of AIS populations. Depending on the specific MCA occlusion site, initial presentations and clinical outcomes can manifest very differently. The patients with a MCA main trunk (M1) infarction demonstrated a severe neurological deficit and had poor functional outcomes similar to occlusions in the internal carotid artery (ICA)14). Thus, early recanalization of M1 occlusion is crucial in order to achieve good functional outcomes, regardless of treatment modality. Comparatively, isolated M2 segment infarctions tend to display relatively mild neurological symptoms compared to M1 occlusions. This is because the M2 division usually separates into at least two branches and involves a more limited vascular territory910). For this reason, the benefit of aggressive EVT for M2 occlusions remains a controversial issue. However, the prognosis of AIS due to M2 occlusions is not always favorable, and a small, yet strategic cerebral infarction may still lead to permanent disabilities. Sheth et al.13) reported that half of patients with M2 occlusions were discharged with moderately severe disability or death; a rate comparable to that of patients with M1 occlusions. Also, Wolpert et al.17) reported an insufficient efficacy of IV tPA for M2 occlusions; a recanalization rate of only 30%. Given these facts, solitary M2 occlusions should be considered as potential targets for EVT.
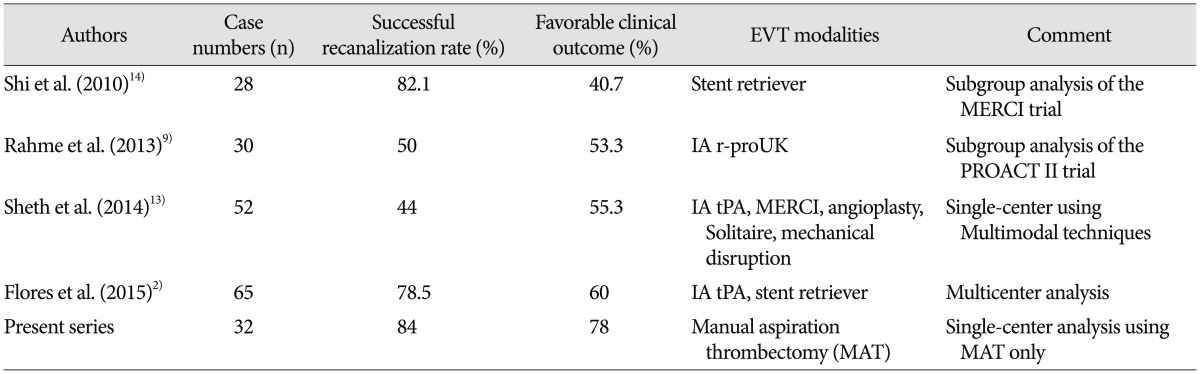
Despite this, previous studies have reported conflicting results about the efficacy of early recanalization of M2 occlusions11015). Broderick et al.1) reported similar safety outcomes and no significant differences in functional independence with EVT after IV tPA, as compared with IV tPA alone. Rahme et al.10) and Tomsick et al.15) concluded that a positive correlation between successful early reperfusion and a favorable outcome could not be applied to patients with M2 occlusions. Yet, more recently, some other studies presenting a positive correlation between early recanalization via EVT and favorable outcomes in patients with M2 occlusions have been reported 291314). Although reported recanalization rates and favorable functional outcomes in the literature have a variable range, these results overall showed comparative or favorable outcomes compared with traditional IV tPA treatment (Table 4). In particular, our work using a penumbra 4 MAX catheter showed a higher recanalization rate compared with other solitary M2 occlusion case series. We felt it was very important that the reperfusion catheter tip be brought into close contact with the thrombus in order to increase the recanalization rate. Thus, the authors advanced a relatively large-bore 8 Fr shuttle sheath and guiding catheter as distally as possible for proximal support, and used a 153-cm long Rebar 18 microcatheter (EV3, Irvine, CA, USA), which is more than 3 cm longer compared with other commercial microcatheters, to achieve sufficient distal support. Through these technical measures, we could easily track and advance the Penumbra catheter into the thrombus during procedures and consequently, obtain higher recanalization rates and favorable outcomes.
Currently, the main instruments of EVT for AIS are stent-retrievers that displayed device efficacy and favorable clinical outcomes in several comparative randomized trials 7812). However, most of the patients in those trials were diagnosed with AIS due to large vessel occlusion, so the efficacy and favorable outcomes of stent-retrievers are not applicable to solitary occlusions in relatively smaller vessels, such as the MCA-M2. Indeed, M2 divisions of the MCA are more distal vessels with a smaller caliber and thinner walls compared with the ICA or M1 trunk, rendering them more vulnerable to possible vessel wall damage during retraction of the deployed stent210).
Recently, several reports have described a manual aspiration technique known as MAT, forced-suction thrombectomy, or the ADAPT technique with promising results regarding recanalization rate, cost effectiveness, procedure duration and functional outcomes5616). These techniques are generally carried out using the newest generation of flexible and large-bore catheters. In our study, we applied MAT for solitary M2 occlusions with the Penumbra 4 MAX catheter. Our preliminary results indicate that this technique is feasible as a first-line therapy for relatively thin and small M2 lesions. In addition, the evolution of devices, such as more supportive microcatheters and more flexible catheters, is expected to provide an expanding scope of application for the manual aspiration technique in EVT for AIS.
To our knowledge, this report is the first single-center case analysis describing the safety and favorable outcomes of MAT using large-bore and flexible catheters for solitary M2 occlusions. However, our study has several limitations. First, it lacks a prospective design; second, our study is a relatively small case series; third, we lack a control group, such as patients treated with other EVT modalities or medical therapy.
Go to :
CONCLUSION
In our experience, MAT using the Penumbra 4 MAX catheter can achieve good angiographic and functional outcomes without serious complications in patients with solitary M2 occlusions. Further well-designed prospective randomized studies should provide definitive evidence regarding this approach compared with other treatment modalities in M2 occlusion.
Go to :
 XML Download
XML Download